Selecting a model with the appropriate ulcer size and location is crucial for accurately assessing new treatment strategies for oral ulcers. This study demonstrated that diabetic rats with oral burn wounds could be effectively used as an animal model for oral ulcer research. The delayed wound healing observed in these rats provides a reliable framework for evaluating the efficacy of therapeutic agents designed to treat oral ulcers.
Various methods have been reported for creating oral wounds in rats, with most studies using blades or punches to induce traumatic ulcerations [4, 8,9,10]. The healing period varies depending on the location and size of the wound, but these excision wounds generally heal naturally within 7 to 14 days [15, 20]. Additionally, there have been studies that created chemical burn wounds in the oral cavity of rats using substances such as phenol and acetic acid [1,2,3]. One study reported that when phenol was used to create oral wounds in rats, only about 5% of the wounds healed naturally even after 18 days [1]. Chemical or thermal burn wounds tend to heal more slowly compared to traumatic wounds [18]. Animal models for burn wounds have primarily focused on the skin, with no studies reported on creating them in the oral mucosa [21]. The most frequently used animal for burn research is the rat, due to its availability, low cost, resistance to infection, and the ability to replicate various types of burns [22]. Typically, burn wounds have been created by directly applying heated metal or water to the shaved dorsum skin of rats [22,23,24]. When a stainless-steel rod with a diameter of 1 cm was heated to 100 °C and applied to the skin for 5 s, a full-thickness burn occurred, and contact for more than 10 s resulted in damage extending to the entire dermis, subcutaneous tissue, and parts of the underlying skeletal muscle [25]. The severity of the burn was related to the age of the rat and the duration of application; in two-month-old rats, a 1 cm diameter metal rod heated to 100 °C caused a superficial second-degree burn with 3 s of contact and a deep second-degree burn with 5 s of contact [24]. Although there are differences between skin and mucosa, our study also applied a stainless-steel instrument heated to 100–120 °C for 3 s on 8-week-old rats, and it is believed that this likely resulted in superficial to deep second-degree burns.
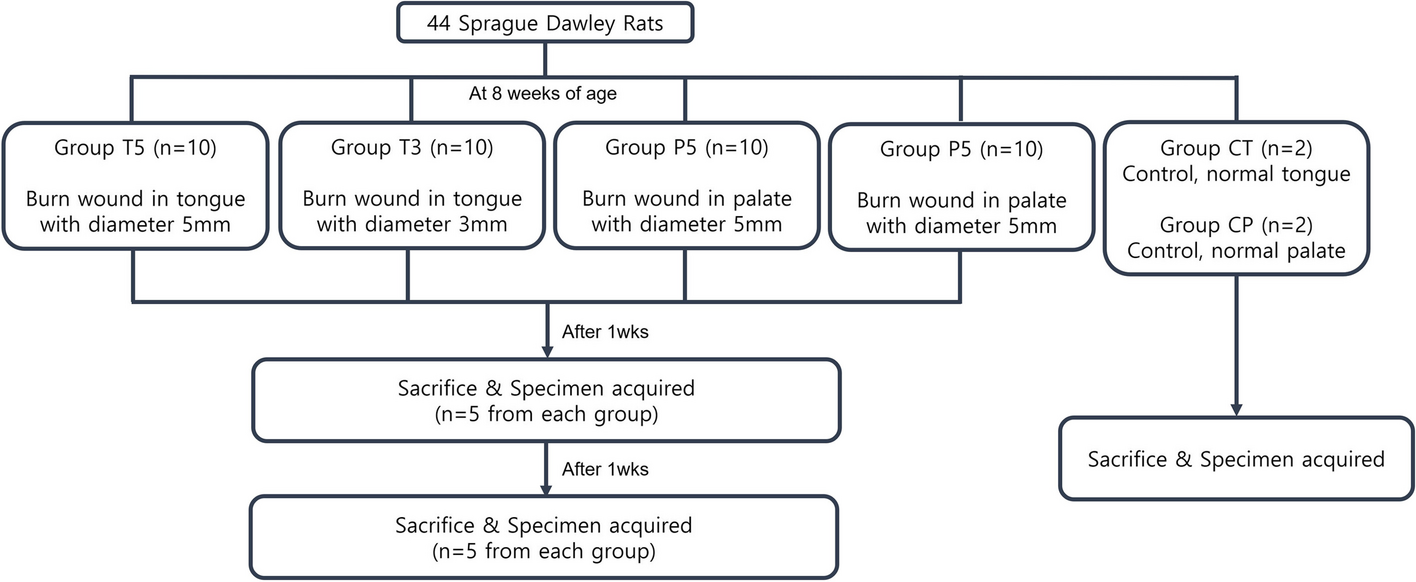
Various sites for creating oral wounds in rats have been reported. Generally, wounds are formed on the palate [8, 9], buccal mucosa [3, 8, 10, 15], tongue [4, 20], and the labial fornix region of the inferior incisors [2, 13]. However, no study has compared the healing of wounds based on the site where they are induced using the same methods. Therefore, this study aimed to establish an experimental animal model with an appropriate healing rate by creating burn-induced oral ulcers of two different sizes at two different sites. We then compared the healing progression over time and analyzed the expression levels of inflammation-associated cytokines TNF-α and IL-1β. The results showed that the expression levels of TNF-α and IL-1β were significantly higher in the group with delayed wound healing, suggesting an enhanced inflammatory response [26]. Excessive inflammation can delay tissue regeneration and impede wound healing [4]. Specifically, elevated TNF-α is associated with chronic and slow-healing acute wounds [27]. The overexpression of TNF-α and IL-1β increases the infiltration and activation of inflammatory cells, leading to a chronic inflammatory state. This process promotes cell apoptosis and accelerates the degradation of the extracellular matrix, acting as a factor that hinders tissue regeneration and recovery [28]. Thus, the observation of high TNF-α and IL-1β expression in the group with impaired wound healing suggests that these inflammatory cytokines were not adequately regulated at the site of tissue damage, preventing the normal progression of the healing process.
Oral tissues share common histological features such as surface epithelium and lamina propria, but the palate differs clinically and histologically from other oral tissues [29, 30]. Wounds on the tongue, which consists of mucosa covering loose connective tissue and muscle, heal more quickly than wounds on the palate, which is attached gingiva covering the alveolar bone, because epithelial coverage progresses rapidly and does not rely on stromal healing [31]. Similarly, in this study, it was observed that wounds on the tongue healed more completely than palatal wounds. Notably, in the 3 mm tongue wound group, complete healing was observed in some rats within just one week. If wounds heal too quickly naturally, the difference in results between the control group and the experimental group is minimal, making it difficult to compare the effectiveness of the new reagents. In contrast, delayed healing was observed in 5 mm tongue wounds after two weeks. Therefore, using a 5 mm tongue model may effectively demonstrate differences in healing patterns between the control group and experimental group, making it suitable for evaluating the effects of new treatment regimens.
Additionally, oral wound healing typically involves the healing of palatal and gingival tissues in the presence of healthy underlying bone and without scar tissue formation. Healing of palatal wounds is more challenging in the absence of healthy underlying bone [32]. A burn wound on the palate may affect the underlying bone due to the thin mucosa, and if thermal osteonecrosis occurs in the bone, the healing of the overlying soft tissue becomes more difficult [33]. In this study, the fact that 3 mm wounds on the tongue healed completely in two weeks, while palatal wounds of the same size remained almost unhealed, may be due to thermal osteonecrosis. In other words, burns on the palate, regardless of size, may affect the underlying bone, making it difficult to assess wound healing with new treatment regimens.
Diabetes increases the risk of wound infection and delays wound healing [34]. Oral ulcers in diabetic patients can experience delayed healing and an increased risk of infection, even if diabetes is well-controlled, necessitating additional treatment measures such as antibiotics or antimicrobial mouthwashes [11, 12]. In a study where an 8 mm diameter oral wound was created in the buccal mucosa of rats, it was observed that diabetic rats took 15 days to heal, whereas normal rats healed after 10 days [15]. Similarly, in another study where a 1.0 by 1.0 by 1.5 mm ulcer was created on the tongue of rats using dental rongeurs, normal rats showed complete epithelialization after 7 days, while diabetic rats still had inflamed wounds by the 14th day [20]. In this study as well, only the group with 3 mm burn wounds on the tongue was completely healed after two weeks, while the other groups showed delayed healing.
The findings from this study suggest that diabetic rats with oral burn wounds, particularly those with larger ulcers on the tongue, represent a suitable model for investigating the healing efficacy of new treatments for oral ulcers. However, palate burn wounds are less reliable due to the high variability in healing outcomes and the technical sensitivity involved in their induction. Additionally, the healing process in tongue burn wounds is more consistent and less variable. For experiments with a 1-week duration, using the tongue model, regardless of ulcer size, is advisable, as neither size typically achieves complete healing within this timeframe. For a 2-week experimental period, the 5 mm tongue model is particularly useful, as it shows a slower healing progression compared to the 3 mm tongue model, allowing for a more detailed evaluation of the therapeutic effects of potential treatments. Future research should focus on evaluating potential therapeutic agents using this model to develop effective treatment strategies for oral ulcer management.
This study has several limitations. First, this study was limited in scope to the analysis of TNF-α and IL-1β as markers of the inflammatory response in diabetic wound healing. Although these cytokines are critical to understanding the inflammatory phase, future studies using this model should consider evaluating a broader range of factors such as EGF, IGF, TGF-β, PDGF, and NGF, which contribute to the regeneration of oral mucosal tissues. Additionally, due to the lack of bone specimen collection and histological analysis, this study could not confirm osteonecrosis in the palatal bone.





Comments (0)