
Remember me



As microsurgery techniques have advanced, the use of free flaps has become common in head and neck reconstruction. The most popular flaps in head and neck reconstruction are RFF flap and ALT flap. The advantages of an RFF flap are that it is easy to harvest, thin, and reliable; therefore, it is always the first free flap that beginner surgeons can master. However, RFF flap has several disadvantages, such as sacrificing a main artery of the forearm, significant donor site morbidity, ugly skin graft scar, skin graft necrosis, and tendon exposure [4] (Fig. 2). As perforator flaps are becoming increasingly popular [7], ALT flap is used in the majority of head and neck reconstruction cases at present. The advantage of the ALT flap is its diversity of applications and that it provides more than enough tissue volume for reconstruction and poses minimal donor site morbidity. However, for medium-sized defects, especially during reconstructing buccal defects and those after semi-glossectomy, the ALT flap seems too bulky and provides too much soft tissue volume to properly restore tongue movement postoperatively. Some researchers [8, 9] have reported that ALT flap can be thinned, but thinning the flap inevitably increases the risk of flap necrosis. Additionally, the thinning process should be done at least 2–3 cm away from the perforators [10]. Apparently, it is not suitable for small- to medium-sized defects.
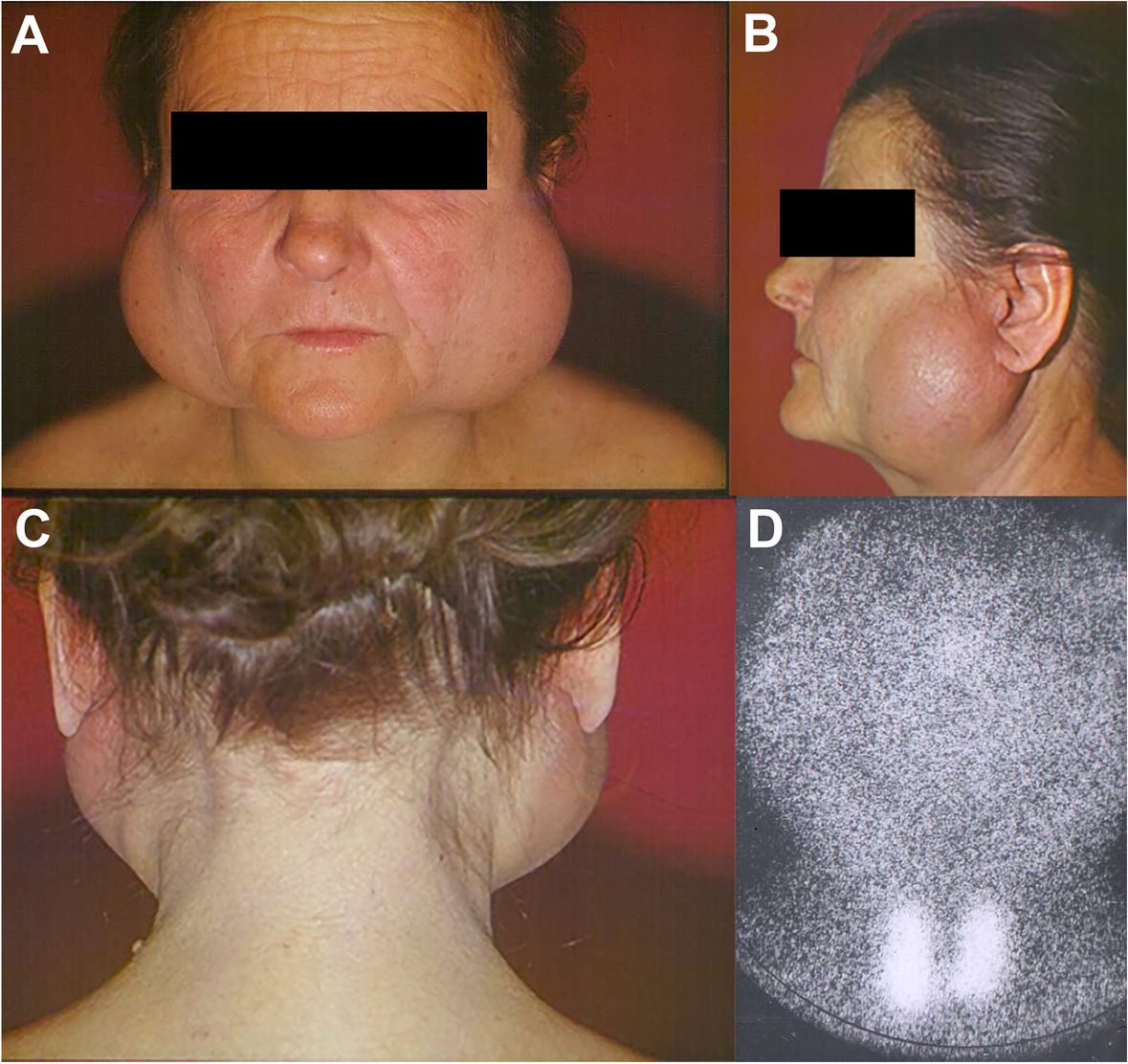
Fig. 2
Significant donor site morbidity of RFF flap. A Ugly skin graft scar, B skin graft necrosis, and C tendon exposure
Since it was first described by Cavadas [11] in 2001, the MSAP flap has drawn attention of many microsurgeons. MSAP flap is a thin, pliable flap, has a long vascular pedicle, less hair-bearing skin, and enables easy dissection with minimal donor-site morbidity. It is also reliable, and there was only one flap necrosis occurred in the MSAP flap group despite only carrying one perforator in our study. Therefore, for a small-medium-sized flap, one perforator is enough for the whole flap blood supply. The survival rate of the MSAP flap in our study is 95.2%; similarly, many other surgeons [12,13,14,15] also reported a high survival rate of the MSAP flap. According to our study, the average pedicle length of the MSAP flap is 11.55 cm, which is longer than the average pedicle length (10.64 cm) of the RFF flap, but there is no significant difference (p = 0.068), both exceed the requirements of head and neck reconstruction [13, 16, 17]. The mean dimensions of the MSAP flap in our case series were 7.33 cm × 4.93 cm, which provides adequate tissue for coverage of medium-sized defects, like half-glossectomy or buccal defect. This is similar to the RFF flap group size, which is 7.44 cm × 5.12 cm (p = 0.787, p = 0.377).
In our study, the flap thickness was 6.05 mm in the MSAP flap group, which seems thicker than the thickness in the RFF group (5.28 mm, p = 0.052), which is a suitable thickness for oral cavity reconstruction, but it did not show significant difference. In our experience, the MSAP flap is better in maintaining the shape of the tongue (Fig. 3A and B), but it is not as pliable as the RFF flap.
Fig. 3
Postoperative morphology of donor and recipient sites of MSAP flap. A and B MSAP flap is better in maintaining the shape of the tongue. C The donor site in the MSAP flap
We selected patients with defects projected narrower than 7 cm preoperatively in our study, so that we could directly close the donor site postoperatively. Some researchers [12, 18] suggested that the width should be less than 5–6 cm to enable primary closure of the donor site. Daar’s [19] analysis revealed that a flap width greater than 5.75 cm would cause more donor site complications if not closed primarily. It would not completely show the advantages of the MSAP flap compared to those of the RFF flap. For patients with defects wider than 7 cm, other flaps are suggested for reconstruction, such as thinned ALT flap or deep inferior epigastric perforator flap. The donor site morbidity in the MSAP flap is a thin linear scar, which is hidden and acceptable (Fig. 3C). In contrast, the donor site in the forearm was frequently exposure site with ugly skin graft scar in the RFF flap group, which aggressively affects the patients’ confidence of participating in social activities. None of the patients in the MSAP flap group had any long-term complications, except for one patient who felt pain in the donor site leg occasionally within 3 months of the operation, which subsided spontaneously. None of the patients have reported any limitations in walking in daily life. Through assessing subjective function and cosmetic satisfaction with our self-made questionnaire, all the patients are satisfied with the minimal donor site morbidity in the MSAP flap group, which is much better than the RFF flap group (8/25, 32%). Kao [12] reported similar results.
The mean harvesting time of the MSAP flap is 46.05 ± 6.05 (range, 40 to 63) min, which is more than the mean harvesting time (30.92 ± 6.11 min, range 20 to 47) of the RFF flap group (p < 0.01), that is because dissecting perforator intramuscular consumes more carefulness and time. When the time of the skin graft is considered, the total time of harvesting flap and donor site closure of two kinds of flaps is almost the same to our experience. Meanwhile, there is no need to do another incision to graft skin in the MSAP group, which increases the donor site morbidity. The poor blood supply of donor site and improper motion of the forearm and hand postoperatively were considered the main factors affecting the healing of skin graft.
The postoperative oral function regards the comparison of swallowing and speech function recovery did not show significant difference (p = 0.547, p = 0.471). In terms of no significant difference in flap size and flap thickness, the postoperative oral function is theoretically consistent with our expectation.
All the cases in the RFF flap group suffered abnormal sensation in donor site, which is related to dysfunction of the superficial branch of the radial nerve. The superficial branch of the radial nerve consists of medial branch and lateral branch, which dominates the sensory function of the ulnar half of the dorsal thumb, dorsal index, long, radial half of the ring finger, and the radial dorsal thumb. We conventionally preserve the superficial branch of the radial nerve when harvesting RFF flap. But the nerve would be pressed for about 7 to 10 days after the skin graft, in order to assure the survival of the skin graft, which could be one of the factors causing the dysfunction of the superficial branch of the radial nerve. That is why all the cases complain the abnormal sensation of donor site. In our experience, the abnormal sensation might be mostly recovered in 2–3 years after surgery. But patients feel uncomfortable before their total recovery, which is not common in the MSAP group. Skin graft also resulted in tendon adhesion in 3 cases, which led to slight limited range of motion of the wrist joint compared to the normal wrist joint.
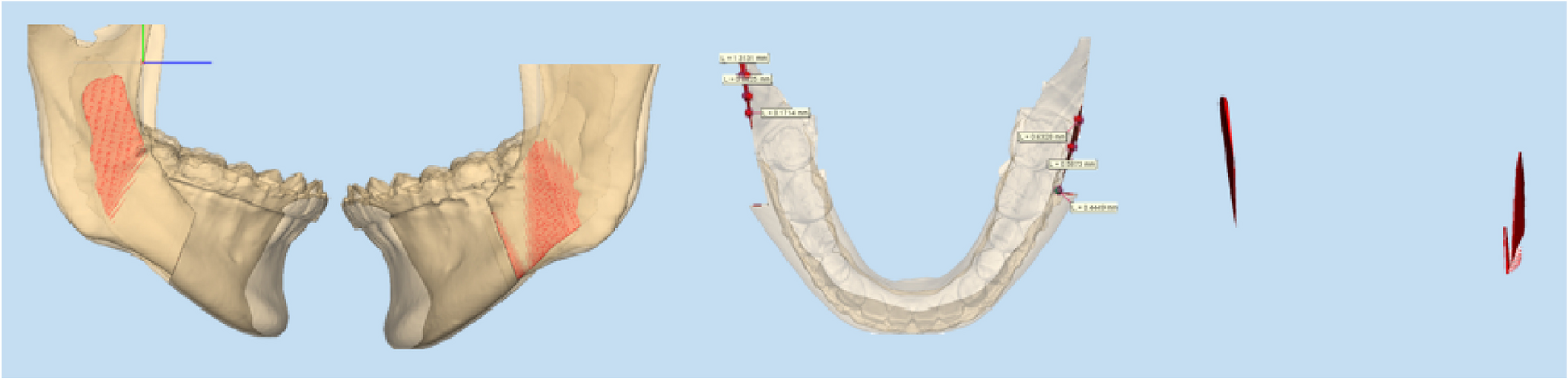
We regularly use color Doppler ultrasound to map the perforator preoperatively and design the flap according to the location where the dominant perforator emerges. This is reliable according to the comparison of the preoperative mark and the location where the perforators actually emerge intraoperatively in our study. So we believe the perforator mark of the other leg also was accurate. We can see the dominant perforator (Fig. 4) mostly emerges near the point which is 15 cm from PF vertically, and 3.15 cm from PML horizontally. This can guide us for flap designing even without perforator mapping preoperatively, which is similar to the research outcomes of Basnet L M [20], but we should leave a route of retreat in case of inaccuracy of perforator mapping. Some authors [21, 22] also have reported an opposite result and have pointed out that Doppler ultrasound is not a reliable technique. Meanwhile, some microsurgeons also locate the perforators using computed tomographic angiography or magnetic resonance angiography, but those need more time and are much more expensive compared to Doppler ultrasound, and their efficacy in mapping perforators is not precise enough. Inaccurate perforator location would misguide the flap design. In this case, the perforators should be explored intraoperatively, and the flap design should be adapted based on the actual location of the perforator. Therefore, we cannot rely completely on machines instead of carefulness.
Fig. 4
Schematic diagram of location of dominant perforator of MSA and MSAP harvesting
Furthermore, MSAP flap also could form a chimeric flap [23] consisting of the conventional medial gastrocnemius muscle flap to reconstruct complex defects, such as floor muscle defect. Similarly, the muscle flap can refill the dead space of the mouth floor to avoid fistula. However, MSAP chimeric flap would increase donor site morbidity.
MSAP flap is reliable, has a suitable thickness of skin paddle, does not need a skin graft, and has minimal donor site morbidity for small- to medium-sized defects compared with RFFF. The question is why is the MSAP flap not as popular as RFF flap? There were three reasons, as mentioned below. First, many microsurgeons are not familiar with the anatomy of the perforator of the medial sural artery (MSA). The MSA and lateral sural artery (LSA) can come directly from the popliteal artery or common sural artery at the popliteal crease level. The MSA and LSA descend to the medial and lateral heads of the gastrocnemius muscle, respectively. Along its course, the MSA has three branching patterns. Type I (31%) exhibit a single main branch, Type II (59%) have a double branching pattern, and Type III (10%) have three or more branches. A dominant medial sural artery perforator can be identified in 92% of cases [24]; Dr.Deek [25] reported 200 consecutive cases of MSAP flap without the absence of the perforator. Also from the perforators’ data, we recorded and analyzed that a reliable MSAP flap can be harvested easily due to the relatively constant anatomy of perforators. Second, most perforators of the MSA are musculocutaneous perforators, which are easily injured intraoperatively, causing flap failure. Third, some surgeons think it is difficult to harvest the MSAP flap with the patient in the supine position as the original vessel of the pedicle is in the popliteal space. In our experience, the supine position with some rotation to the donor site side would enable the surgeon to complete the operation easily.
We present our study here aiming to popularize the MSAP flap in small- to medium-sized defect reconstruction. There might be other major perforators for MSA that need to be identified; we will do further research on them to extend the application of MSAP (chimeric) flap. Due to insufficient cases, further studies are required to accumulate more data and experience.
Comments (0)