
Remember me




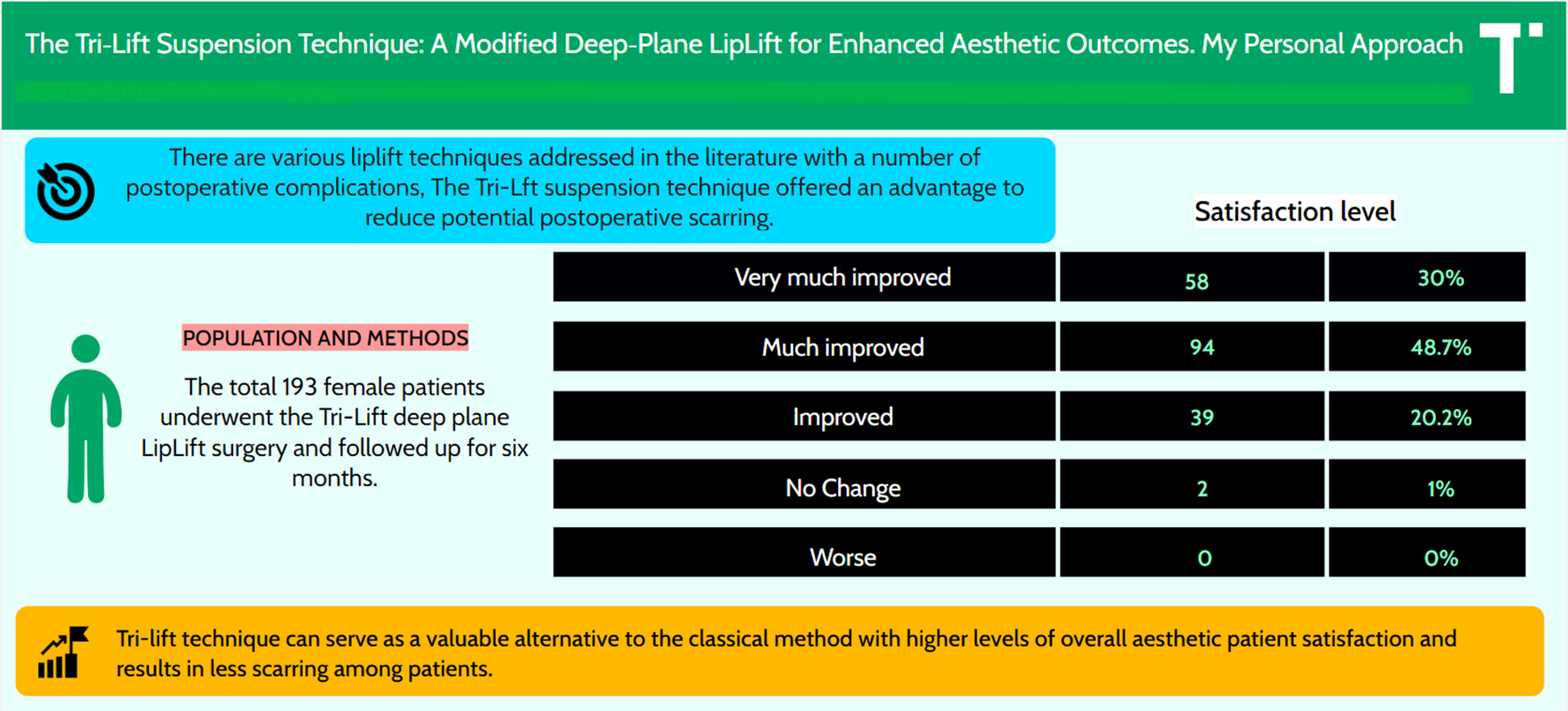
A cross-sectional study was conducted to evaluate the outcomes of the Tri-Lift suspension technique, a modified deep-plane subnasal lip lift designed to optimize aesthetic results through enhanced suspension and deeper dissection. This technique was applied to 193 patients (mean age: 28 years), incorporating triple suspension sutures for secure fixation and minimized postoperative complications. As a comparison, the traditional lip lift (bullhorn technique) was performed on 50 female patients (mean age: 32.48 years) to serve as a control group.
The study was conducted between September 2022 and June 2024 at the Dermodento Cosmetic Center, Sulaymaniyah, Iraq. Patients were selected using convenience sampling. Inclusion criteria consisted of medically healthy individuals with no history of upper lip surgeries, permanent lip fillers, or keloid formation. Written informed consent was obtained from all participants. Data collection included patient demographics, complications, and pre- and postoperative measurements of philtral length, vermilion height, and dental show.
Outcome measures included patient-reported satisfaction, assessed at 6 months postoperatively using the global improvement scale and the WHO Quality of Life Questionnaire. Satisfaction was categorized into four levels:
Very much improved: Significant aesthetic enhancements, with optimal improvements in philtral length, vermilion height, and dental show; no notable complications.
Much improved: Substantial improvements, though less dramatic, are often influenced by anatomical variations or pre-existing conditions.
Improved: Noticeable but subtler changes, potentially due to minor concerns or residual asymmetry.
No change: Minimal impact, likely related to high baseline aesthetics or unmet expectations unrelated to surgery.
Statistical analysis was performed using chi-square tests to compare satisfaction levels and objective outcomes between the two techniques.
The study adhered to the Declaration of Helsinki ethical principles and received institutional approval from the College of Dentistry/Oral and Maxillofacial Department. Quantitative results were presented in a comparative table, demonstrating significantly higher satisfaction rates and fewer complications with the Tri-Lift suspension technique compared to the traditional lip lift (P < 0.05).
Patient selectionLip lift procedures are suitable for individuals with a noticeable distance between the base of the nose and the upper lip vermilion border, regardless of lip fullness. While many seek lip lifts for rejuvenation purposes, some target congenitally long philtra in younger patients. Candidates are identified during preoperative consultations or through photographic reviews.
A novel classification system has been introduced to identify individuals who are appropriate candidates for lip lift surgery (Table 1) [23]. This system classifies patients based on their labial and philtral height and it is supported by two diagnostic tools: (1) A philtral-labial score (PLS), which measures the ratio of philtral height to upper lip height at the midline, and (2) dental show, which indicates the visibility of the upper incisors when the lips are slightly parted at rest. The utilization of this system helped in identifying suitable candidates for the study.
Table 1 The classification system for the upper lip, diagnosis, and surgical management, presuming the absence of maxillary deformities [23]Types 2 and 3 in the classification system feature tall philtra, a philtral-labial score (PLS) of at least 3, and no dental show. These individuals often exhibit upper lip inversion. They are considered ideal candidates for a lip lift surgery if they meet certain health criteria and have normal maxillary height. Corrective measures for skeletal abnormalities should be addressed before soft tissue correction. Another group of candidates includes individuals termed “duckbills,” who have undergone excessive prior lip augmentation, where a lip lift would have been a more beneficial approach [24, 25].
Patients classified as type 0 (defect-free) and type 1 (thin lips) are not ideal candidates for lip lifts. Type 0 patients may consider augmentation, while type 1 lips may show improved vermilion exposure with lifting but risk a shorter philtrum. Additional exclusion criteria include a history of hypertrophic scarring and large ratios of lip width to nasal base or downturned commissures from under correction [13].
Despite the concealing effect of nostril sills in their underlying crease, some surgeons are against indirect lifts for patients with hypoplastic ones [6, 9]. However, in our patient selection process, the presence of prominent sills is not considered necessary, as endonasal scarring eliminates their camouflaging ability. Factors such as age, skin thickness, and Fitzpatrick skin type are regarded as immaterial in our approach [7, 13].
Surgical markingThe precise excision outlines and radial reference markings were meticulously drawn on the patient. These markings, based on the classical “bullhorn” lip lift paradigm, are meticulously applied to determine the optimal upper lip excision and ensure symmetrical alignment of the design (Fig. 1).
Fig. 1
The surgical markings used to define the areas of planned excision for the Tri-Lift suspension technique. The markings ensure symmetrical excision and precise alignment during the procedure (classical bullhorn)
ExcisionThe procedure is performed under local anesthesia with the surgeon positioned at the head of the bed. After prepping the perioral area, the surgeon makes perpendicular lower incisions followed by parallel upper incisions. The skin and subcutaneous flap are then excised over the orbicularis oris muscle, leaving a thin layer of intact fat containing the vasculature (Fig. 2).
Fig. 2
The area after the skin and subcutaneous tissue excision down to the SMAS layer of the upper lip. The excised portion corresponds to the preoperative markings, exposing the underlying musculature for further dissection and suspension
DissectionAfter excision, the labial flap is simply elevated in a deep sub-superficial musculoaponeurotic system (SMAS) plane, releasing the labial SMAS from the orbicularis oris muscle below. Centrally extending halfway down to the central philtrum here one can easily feel the hardness of the anterior nasal septum and laterally expose the periosteum at the lateral wall of the nasal aperture (pyriform fossa) for future suture suspension. Care is taken to maintain a sub-SMAS plane to avoid excessive bleeding or damage to the labial elevator complex. Hemostasis is achieved, preferably with bipolar cautery.
Suspension and closureThe common mistake among clinicians is relying on basic simple dermal closure methods. Optimal results are achieved by releasing tethering structures and suspending dense tissue upwards. This approach enables the liberated skin/SMAS flap to redistribute tension above the contracted orbicularis oris muscle effectively.
The dermis at the base of the nose lacks firm attachment. Firm suspension points are provided by the periosteum, the pyriform ligament, and the anterior nasal spine. The pyriform ligament, consisting of dense fibrous tissue over the periosteum, spans the pyriform aperture and serves as an optimal site for engaging suspensory sutures [7].
The Tri-Lift suspension technique, also known as the triple suspension technique, uses a 5–0 PDS suture, which is resorbable. This is preferred because, after about a month, the labial tissue heals, eliminating the need for non-resorbable materials. The procedure starts by simply passing the needle through the periosteum over the anterior nasal spine at the center, then laterally to the junction of the nasal and oral musculatures. The needle is then positioned deeper to engage the periosteum on the lateral edge of the pyriform aperture, exiting near the alar dermis ensuring not incorporate the dermis (Fig. 3).
Fig. 3
a The triple suspension suture on the periosteum of the anterior nasal spine and pyriform aperture. The sutures are secured at key points to elevate the lip and maintain tension for improved aesthetic outcomes. b A schematic representation showing the periosteal anchor points for the sutures used during the Tri-Lift suspension technique. The figure highlights the exact anatomical sites for secure and effective lip elevation
Subsequently, the needle is directed inferiorly through the SMAS on the undersurface of the labial flap both centrally and laterally. However, caution must be taken to avoid overtightening the knots, as this may lead to inward enrollment of the labial flap. Suturing to the SMAS rather than the dermis enables the skin to approximate without tension or dimpling. This confers a significant advantage by aligning the dermal edges, given that the SMAS of the upper lip is a distinct tissue layer with considerable strength located just deep to the reticular dermis.
The incision is subsequently closed further at the subcutaneous level, starting centrally and progressing laterally using a PDS 6.0 suture. This type of suture material is preferred due to its minimal tissue reaction, which can impact healing and scar development. Upon tying the knots, the skin edges should be closely approximated. Finally, reapproximation of the skin surface is achieved through meticulous suturing using 6–0 nylon sutures, ensuring the resolution of any step-offs from the lower to upper skin flaps, and the case is followed up after 6 months for evaluation (Fig. 4a, b).
Fig. 4
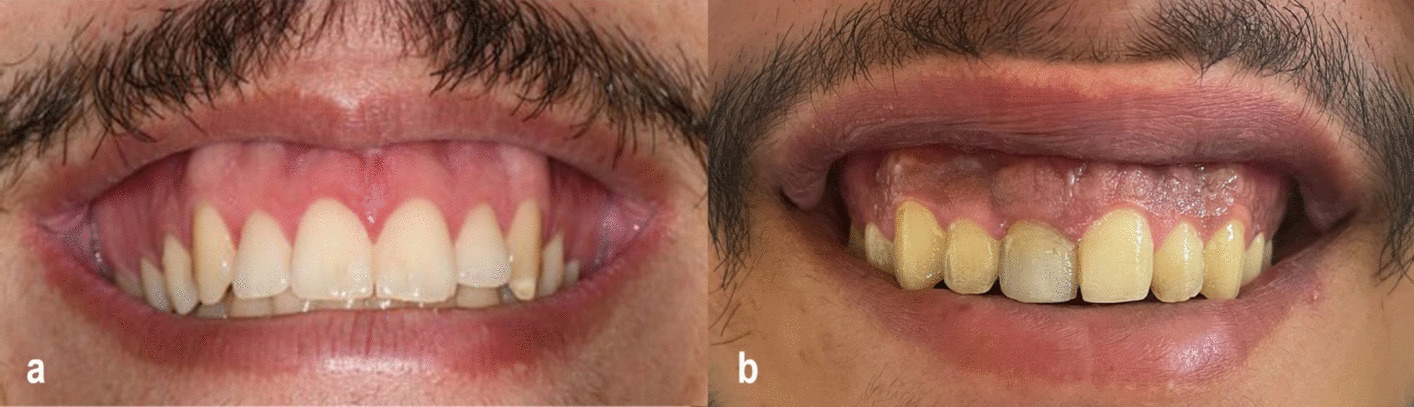
a A 6-month follow-up of a 30-year-old woman who underwent the Tri-Lift suspension technique reveals preoperative measurements of a 16-mm philtral length, reduced to 12 mm postoperatively, an increase in vermilion height from 7 to 10 mm, and an improvement in the dental show from 3 to 6 mm. Reported satisfaction level: very much improved. b A 6-month postoperative image of a patient treated with the Tri-Lift suspension technique demonstrates a reduction in philtral length from 15 to 10 mm, an increase in vermilion height from 6 to 9 mm, and noticeable improvement in overall aesthetics. Reported satisfaction level: much improved
Postoperative careThe surgical site should be consistently moistened with antibiotics and anti-scar ointment during the healing period. Patients should be educated about postoperative instructions to prevent disruption of healing and anticipate significant swelling, which may persist for up to 2 months. This prolonged swelling can be attributed to bilateral lymphatic drainage disruption and postoperative myositis induced by muscle trauma.
During the initial 2 months after surgery, stiffness and swelling can aid in incisional healing by limiting movement along the incision line. Patients should attend follow-up appointments every 3 weeks for potential 5-fluorouracil 50 mg/cc injections into firm orbicularis oris patches and may receive fractionated CO2 laser treatment for the nasal base if needed, typically administered routinely at 60 and 120 days with a low setting.
Comments (0)