
Remember me
Cortisol, one of the most important human glucocorticoids, is a powerful modulator of physiological systems, including the central nervous system. When initially discovered in the 1950s, it was applied to rheumatic patients with remarkable results [17]. Subsequent experiments expanded the scope and validated powerful effects in anti-inflammation, anti-allergy and anti-shock.
The HPA axis mainly includes the parvocellular corticotropin-releasing hormone (CRH), argininevasopressin (AVP) neurons of the hypothalamic paraventricular nuclei (PVN), anterior pituitary corticotrophs and adrenal cortisol-producing cells. Altogether they administer the secretion of cortisol through a complex positive and negative feedback system. Normal cortisol management follows a circadian pattern. The amplitude of CRH and AVP pulses surges sharply at dawn, leading to a burst of corticotropin (ACTH) secretion in the systemic circulation [1]. Consequently, cortisol is usually high upon awakening, then rises within 30–40 min and slowly falls throughout the day. It reaches its nadir around midnight, the amount of which is about a quarter of that in the early morning. During the rest of the day, it was secreted in pulses at a frequency of approximately twenty to thirty minutes at a time [18]. The balance of the HPA axis is vital for maintaining physical and mental health, for both overactivity and underactivity of the HPA axis may contribute to diseases.
Cortisol acts as a systemic effector of the HPA axis, whose secretion is closely connected with environmental and empirical events. Stress is a threatened state of homeostasis or dissonance caused by internal or external adverse forces or stressors [2, 19]. Stressful circumstances and other stimuli that may not constitute stress (like exercise, anxiolytics or sexual experience) can elicit cortisol secretion. Stress response is an upward generative, dynamically regulated but evolutionarily conserved response, during which the activation of the HPA axis is mild but brings about amplified and prolonged secretory responses [20].
It is well known as early as the last century that chronic stress influences glucose homeostasis and links to T2DM because of the diabetogenic effects of glucocorticoid and stress hormones [21, 22]. A 1980 study [23] found that stress had a much greater adverse effect on blood glucose regulation in diabetic patients compared with normal subjects. An American article [24] in 1996 suggested that the 24-hour cortisol rhythm is responsible, at least in part, for the circadian variation in glucose tolerance. In recent years, we discovered that elevated plasma cortisol in the morning is associated with greater insulin resistance, reduced β-cell function [25] and a higher risk of diabetes [26]. This result was revalidated in African Americans in 2019 [27], where morning cortisol was associated with a variety of glucose metabolism indicators (increased FPG and HbA1c, decreased β-cell function) and the prevalence of T2DM in AA. Moreover, cortisol is bound up with diabetic complications and long-term prognosis. Roy and Chiodini verified that cortisol concentration is correlated with the degree of diabetic complications, respectively [28, 29].
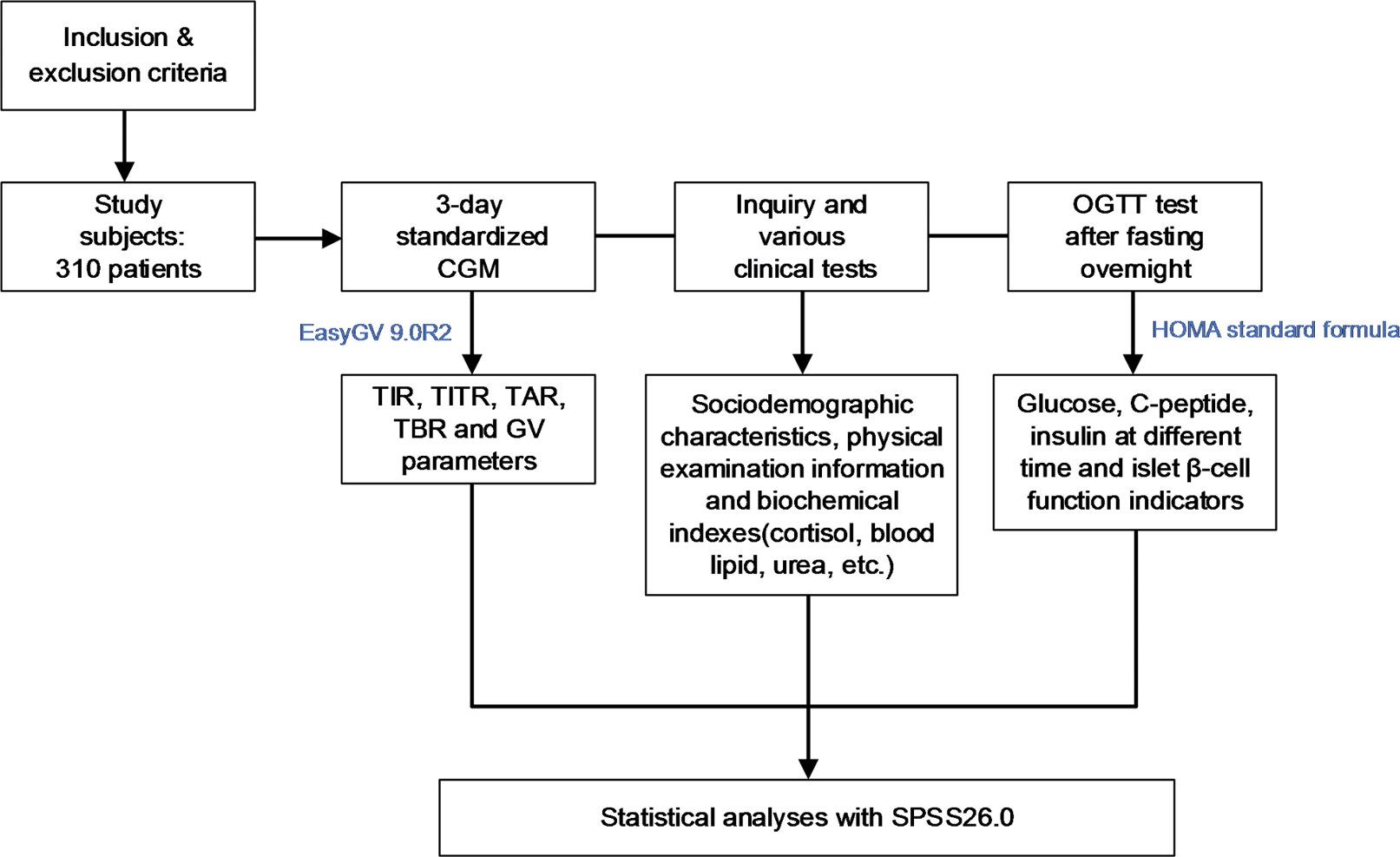
To explore the relationship between cortisol and GV parameters, we employed CGM in our study to monitor blood glucose fluctuations. As an emerging indicator, TIR not only provides comprehensive, continuous and reliable short-term glucose variability information, but can be used to predict diabetic complications and evaluate clinical terminal outcomes as well [11]. Besides, TIR is highly correlated with HbA1C, both of which have been currently recommended as major indicators to assess individual glycemic control [30].
Since plenty of studies have elucidated the unfavourable effects of cortisol on glucose metabolism, our present study added several chief new components. To begin with, we adopted a novel and popular clinical technique, CGM. The traditional hormone cortisol and the brand-new blood glucose assessment index TIR were combined together for the first time. There existed a stronger negative correlation between cortisol and TIR than the current gold standard HbA1C. Compared with previous studies that used to choose FPG and blood glucose at different time points as indexes, GV parameters stemmed from CGM were more comprehensive and detailed. It turned out that higher cortisol was concerned with reduced LBGI and increased TAR, TBR, HbA1c and GV parameters such as TAR, MBG, HBGI and LAGE. Obviously, these results suggested that cortisol was an adverse factor for glucose stability, which added new cogent evidence to this heated issue. In addition, our finding echoed the rhythm of hormone secretion. Based on glycemic profile for three consecutive days, we converted TIR into daytime TIR and nighttime TIR so as to conduct more targeted research. The correlation between cortisol and daytime TIR was obviously stronger than that of overnight TIR. Plus, cortisol was verified an independent contributor of TIR and diurnal TIR, with diurnal TIR of stronger relevance. This implied that the effect of cortisol on blood glucose was closely allied to its circadian rhythm. Dawn phenomenon is defined as a state of hyperglycemia in the early morning (typically 3 to 9 am) without hypoglycemia at night in diabetic patients, which is mainly caused by the unbalanced secretion of various glucose-raising hormones, such as growth hormone, adrenocortical hormone, catecholamines and glucagon [31]. Cortisol reaches its peak at 8 in the morning and drops down gradually throughout the day, roughly in accordance with the occurrence time of the “dawn phenomenon”. The basal insulin secretion of normal people goes up with the increase of glucose-producing hormones, while the insulin secretion of diabetic patients is insufficient, which cannot effectively counteract the glucose-producing effect caused by glucose-producing hormones. Our finding suggested that cortisol had an improved impact on glycemic control during the day than during the night, thanks to the circadian rhythm of cortisol secretion and intenser activities in the daytime. Last but not least, a more comprehensive array of indexes was picked to assess islet β-cell function. Cortisol was negatively associated with C-peptide at different time points after meal, AUCCp0.5 h, AUCCp3h, IGI and HOMA-β. These results provided direct clinical evidence to explain the mechanism by which cortisol influences blood glucose, for it results in reduced β-cell function and insulin secretion. No significant relation was shown between cortisol and HOMA-IR, consistent with previous research findings [27].
Actually, a variety of pathways has been preliminarily studied through which cortisol elevates blood glucose. Glucocorticoids enhance the expression of gluconeogenic enzymes, reduce key mediators of insulin action in peripheral tissues and stimulate skeletal muscle protein and adipose tissue hydrolysis in order to promote gluconeogenesis, leading to hyperglycemia and insulin resistance in the body. Besides, glucocorticoids also regulate gene expression through ribocortin receptors, impairing glucose uptake and metabolism in islet β-cells [32]. Meanwhile, the aggregation of visceral fat, immunosuppression and secretion of various cytokines, as well as the recalibulation of mitochondrial function and the accumulation damage to mitochondrial DNA caused by high cortisol, are all connected to the pathogenesis of hyperglycemia [33].
To delve deeper, alterations in the HPA axis activity spectrum are associated with a series of pathological biomedical conditions, including mental disorders (depression, panic anxiety and anorexia nervosa) [2, 34] and other physiological diseases (T2DM, hypertension, obesity, atherosclerosis and Alzheimer’s disease) [35, 36]. It is not difficult to speculate that there exists a complex interaction between the HPA axis and diabetes status. Apart from the adverse effects of excessive cortisol on blood glucose mentioned above, the glycemic state of diabetic patients has a counterproductive effect on the HPA axis at the same time. Diabetes status is a stress metabolic condition of cells that induces lingering activation of the HPA axis. Enduring distress and depression caused by chronic illness is concerned with the turbulence of the HPA axis as well, for at least 10–15% of patients with diabetes suffer from depression [34]. The centrality hypothesis proposes that hyperglycemia is associated with hippocampal atrophy and a hypothetical decrease in hypothalamic inhibition of the hippocampus. Moreover, patients with diabetes may have impaired pituitary feedback [37]. In the meantime, available literature supports the assumption that modifications in cortisol occur before the onset of insulin resistance and T2DM [27].
In terms of clinical application, cortisol intervention may be a new treatment idea for diabetes. Patients with extravagant cortisol, known as Cushing’s syndrome, have a phenotype similar to metabolic syndrome, making glucocorticoids an attractive therapeutic target. On top of expanding engagement of the sympathetic nervous system and the HPA axis, another common pathological mechanism in diabetes is advanced expression of 11-βHSD 1 in adipose tissue (Fig. 2), which converts inactive cortisone to cortisol, raising local levels of glucocorticoids. Studies conducted in rodents show improved metabolic profiles using 11β-HSD 1 inhibition. In humans, 11β-HSD 1 inhibition (currently mainly the selective compound carbenoxolone) has beneficial metabolic effects, most notably in models of insulin resistance and T2DM [38].
Fig. 2
Partial pathways of interaction between the HPA axis and type 2 diabetes and possible drug targets
Over and above, diabetes is known to damage the nervous system and increase the risk of dementia and depression, for T2DM appears to share common pathophysiological mechanisms with cognitive disorders like Alzheimer’s disease, which is affiliated with insulin resistance. Coincidentally, hypercortisolemia is similarly associated with cognitive dysfunction. The human body requires basal levels of glucocorticoids to maintain neurons, but very high morning cortisol in older adults with T2DM has deleterious effects on cognitive function [26]. It has been perceived that cognitive disorders and depression in diabetic patients may be linked with hyperactivity of the HPA axis, both of which can be ameliorated by normalizing the HPA axis. GLP-1 receptor agonists compensate for the reduction of GLP-1 levels and secretion in diabetic patients, giving an excellent answer in improving cognition and protecting nerves. However, its role in the physiological regulation of the HPA axis is far from fully understood, as Fig. 2 demonstrated. GLP-1 receptor agonists activate circuits engaged in the acute neuroendocrine response to stress, promoting the HPA axis activation and CRH secretion, but appear to be attenuated in humans over a relatively short period of time (like one week), without relevant functional consequences in the long term [39]. The utilize of GLP-1 receptor agonists in patients diagnosed with diabetic encephalopathy along with elevated cortisol is a potential clinical issue to be explored.
To add a little more, there is an interesting result worth discussing that cortisol is thought to have an effect on blood pressure and lipid levels at the same time, while no differences were shown among groups in this study. The number of patients with antihypertensive or lipid medications across groups agrees. Although cortisol dose have some effects on blood pressure, actually it is aldosterone that plays a decisive role. The main function of the renin-angiotensin-aldosterone system (RAAS) is to regulate human blood pressure and maintain water and electrolyte balance, the over activation of which is one of the major causes of hypertension. It is widely accepted that mineralocorticoids play a much more important role than glucocorticoids in regulating blood pressure. Study has revealed that cortisol influences weakly the level of blood pressure independently from plasma aldosterone and that plasma cortisol at 8 is not associated with blood pressure [40]. Analogously, lipolytic rate-limiting enzymes play a major role in the catabolism of lipids. Lipolytic rate-limiting enzymes include hormone-sensitive lipase (HSL) and lipoprotein lipase (LPL), which are affected mostly by medullary hormones such as adrenal and norepinephrine, and glucose-metabolism-related hormones such as insulin and glucagon. Cortisol levels of participants in this study were basically within the normal physiological range, which failed to cause a statistically significant difference in blood serum lipid profiles in different individuals.
Our study has certain limitations, though. First of all, patients in our study received a 3-day CGM testing rather than those of 10–14 days recommended at international level [3, 41]. Besides, the detection of plasma free cortisol was relatively single, with only one time point (8 in the morning). A flattened circadian cortisol rhythm provides forceful evidence for a specific HPA system dysfunction, which requires detection of cortisol at multiple time points like 16 and 24. And hospitalization stress such as unfamiliar environment, insomnia, and anxiety might affect cortisol results. Moreover, cell or animal experiments were requested in order to explore possible mechanisms. Last of all, a retrospective observational study with a rather minor sample size might be considered unconvincing. In the future, a larger multi-center prospective study is demanded to validate the findings.
To recapitulate, serum cortisol at 8 o’ clock is negatively correlated with TIR, especially diurnal TIR due to its circadian rhythm and positively correlated with GV parameters. Immoderate cortisol may have an adverse influence on glucose homeostasis in T2DM, which may become a potential new target for future interference of diabetes and its complications.
Comments (0)