2.1 Study Design
A single-center cross-over study in healthy volunteers was conducted at the University Medical Center Groningen. The study was approved by the Medical Ethics Committee (Stichting Beoordeling Ethiek Biomedisch Onderzoek, METc Assen: July 21st, 2021, NL76998.056.21) and was registered in the Netherlands Trial Register (https://trialsearch.who.int, reference: NL9312). All volunteers provided written informed consent before the study procedures. The main results are described by our colleagues de Keijzer et al [15, 16]. The important aspects of the clinical trial are summarized below.
2.1.1 Inclusion and Exclusion Criteria
Thirty-six healthy volunteers were included in three groups according to age (18–34, 35–50 and 51–70 years) of equal proportion and included a 1:1 male-to-female ratio. Volunteers with the following conditions were excluded: pregnancy, cardiovascular disease, a difference of >15 mmHg between the systolic blood pressure (SBP) or diastolic blood pressure (DBP) measured on the left and right upper arm, increased risk of difficult mask ventilation or tracheal intubation, pulmonary, gastric or endocrinologic disease, end-stage kidney or liver failure, use of tricyclic antidepressants or monoamine oxidase (MAO) inhibitors.
2.1.2 Study Procedures
Standard monitoring was applied to all volunteers including electrocardiography (ECG), pulse-oximetry, non-invasive blood pressure and bispectral index (BIS) (Philips IntelliVue MP50 [Philips, Eindhoven, The Netherlands]; BIS VISTA, Aspect Medical Systems Inc., Norwood, USA). For each volunteer, a peripheral intravenous catheter was placed and a continuous infusion of Ringers Lactate (Baxter B.V., Utrecht, The Netherlands) was initiated at a rate of 10 mL/h–1. Under local anesthesia, a 20G arterial catheter was inserted in the radial artery for every volunteer. A computer system running RUGLOOP II software (Demed, Sinaai, Belgium) was used to synchronize data recording.
The study consisted of two phases: an awake phase and a general anesthesia phase. In the awake phase only NE was administered, whereas in the general anesthesia phase NE was administered in the concomitant presence of propofol and remifentanil. A washout period of 30 minutes was implemented. The general anesthesia phase commenced either when arterial blood pressure (ABP) returned to baseline level (within a 10% variability) or after one hour after the washout phase, whichever occurred first. Preoxygenation was performed for every volunteer using an inspired oxygen fraction of 1.0. Throughout the general anesthesia phase, each volunteer was fitted with a laryngeal mask, and mechanical ventilation was initiated using pressure-controlled ventilation. Tidal volumes of 6–8 mL/kg–1 (ideal body weight) were maintained, and zero positive end-expiratory pressure was applied using the Zeus ventilator (Dräger, Lübeck, Germany) to ensure normocapnia. Surgical incision was simulated by applying a nociceptive electrical stimulus during the general anesthesia phase. The stimulus was generated by EZstim III peripheral nerve stimulator (Halyard, Zaventem, Belgium), lasting 30 seconds (50mA, 100Hz) was administered during the general anesthesia phase following the sampling procedure at each incremental step. After the stimulus, another NE sample was drawn to assess the subclinical response it has triggered (i.e., the release of NE).
2.1.3 Drug Administration
During the awake phase, each volunteer first received a small bolus administration of 5 mcg then a step-up dosing regimen of NE (norepinephrine tartrate CF, Centrafarm, Breda, The Netherlands). The dosing regimen comprised five consecutive steps with doses of 0.04, 0.08, 0.12, 0.16, and 0.20 mcg/kg–1/min–1, each step lasting for 15 minutes. Norepinephrine was administered through peripheral intravenous infusion, utilizing a dilute solution of 20 mcg/mL–1 delivered via a BD Alaris GH plus syringe pump (Becton Dickinson, Eysins, Switzerland). During the procedure, an increase in SBP exceeding 200 mmHg for more than one minute was avoided at all times and was the per protocol reason for ceasing administration of norepinephrine. In addition, if mean arterial pressure (MAP) increased by more than 40% from baseline, the current step was finished and the NE dose was not further increased.
In the general anesthesia phase, propofol (Propofol MCT/LCT 20 mg/mL–1, Fresenius Kabi, Bad Homburg, Germany) and remifentanil (Remifentanil 50 mcg/mL–1 Mylan, Canonsburg, USA) were administered using target controlled infusion (TCI). Propofol dosing was guided by the Eleveld model to attain a 50% age-adjusted drug effect concentration [17] and the Eleveld remifentanil model was used to target an effect-site concentration of 3.6 ng/mL–1 [18]. The dosing combination was chosen to simulate anesthetic doses that are comparable to clinical practice and were shown to be favorable to obtain adequate anesthesia in terms of hemodynamics, noxious stimulation (i.e., movement and electroencephalogram suppression) [19]. Drug administration was managed using BD Alaris GH pumps (Cardinal Health, Basingstoke, UK) controlled by RUGLOOP II software (DEMED, Sinaai, Belgium). Fifteen minutes after general anesthesia induction, a NE bolus of 5 mcg was planned to be administered, followed by the initiation of a step-up NE dosing regimen that is the same as that used in the awake phase. In case MAP dropped below 50 mmHg after general anesthesia induction, NE infusion was initiated immediately instead of waiting for the intended starting point. Following the completion of the final dosing step, the administration of propofol and remifentanil was terminated. Administration of NE was gradually reduced with the goal of maintaining normotension.
2.1.4 Bioanalysis and Sample Collection
In the awake phase, a baseline blood sample was obtained from each volunteer prior to the initiation of any drug administration. A blood sample was collected at the end of every step of the step-up NE dosing scheme. After NE infusion was stopped, more samples were taken at 2, 5, and 30 minutes. During the general anesthesia phase, sample collection was conducted in a similar manner as in the awake state. Additional samples were collected upon cessation of anesthesia and subsequently at 2, 5, 10, 20, 30 minutes thereafter. Following the cessation of the stimulus, an additional blood sample was obtained from each volunteer. Following blood sample collection, the samples were processed and analysed according to previously described methods [20].
2.2 Population PK Modelling
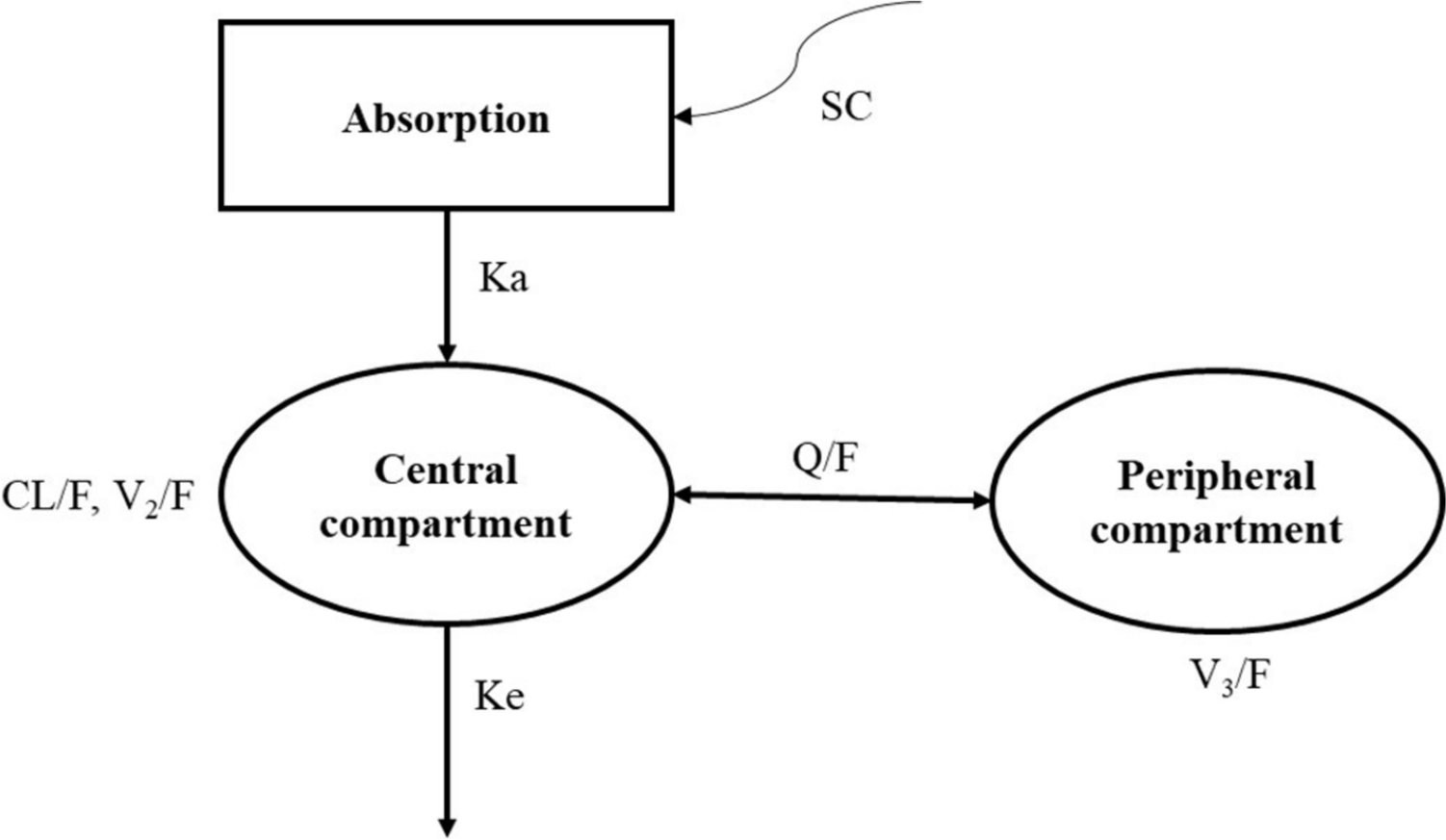
Norepinephrine concentrations were analyzed by developing a non-linear mixed-effect population pharmacokinetic model. Data were fitted using the first-order conditional estimation method with interaction (FOCE-I) algorithm in NONMEM (version 7.5; Icon Development Solutions, Hannover, MD, USA) in combination with Pirana (version 3.0.0; Certara, Lugano, Ticino, Switzerland) as a graphical interface. The model building process started by exploring one-, two- and three-compartmental PK models with first-order elimination. As NE is an endogenous substance, a baseline level of NE, prior to NE administration, was described in the model according to Eq. 1.
$$} = \frac}}}}/}}}.$$
(1)
where baseline denotes the amount of NE in the central compartment before NE administration. Prod (ng/min–1), CL (L/min–1) and Vc (L) denote the endogenous production rate, the clearance and the volume of distribution of the central compartment of NE. To account for the short delay between the time NE travels from the drug administration site to the sampling site in the contralateral arm, we explored the possibility of employing a lag time in the model.
Inter-individual variability (IIV) on the typical population parameters was assumed to be log-normally distributed using an exponential transform of the random effect. Bodyweight (BW) was included in the model a priori using allometric scaling [21]. In accordance with theory based allometric scaling, the exponents were 0.75 for clearance parameters and production rate, 1.00 for volumes of distribution parameters, and 0.25 for the lag time parameter. Age, weight, height, sex, body mass index (BMI), session effect (whether individuals were awake or under general anesthesia) were evaluated by analyzing the correlations between estimated IIV of the population parameters after the basic model was established. Covariates with a correlation coefficient >0.5 were tested in the model using linear, power or exponential functions. Relevant hemodynamic (CO, HR, MAP) and anesthetic (measured propofol concentrations, remifentanil concentrations) variables were explored to account for the session effect should one exist. Proportional, additive and combined error models were explored to describe residual variability.
2.3 Model Evaluation
For each step of model building, a modification of the model is accepted when: (1) the objective function value (as implemented in NONMEM) showed a reduction greater than 3.85, which corresponds to the 5% significance level critical quantile of the chi-square distribution; (2) improvements were seen in the goodness-of-fit plots; (3) precision and plausibility of the estimated parameters were considered reasonable.
Goodness-of-fit of the model was graphically evaluated in R (version 4.2.2; R Foundation for Statistical Computing, Vienna, Austria) using the “tidyverse” package (version 1.3.2). Individual and population predictions were plotted versus the observed data, and bias between the conditionally weighted residuals (CWRES) versus population predictions and time was evaluated. Prediction-variance-corrected visual predictive checks (pvcVPC) based on 1000 simulations were constructed to evaluate the predictive performance of the model [22]. Precision of the parameter estimates were evaluated by estimating the 95% confidence intervals (CIs) using log-likelihood profiling.
To compare the predictive performance of the final model with models from the literature, median prediction error (MdPE) and median absolute prediction error (MdAPE) were calculated according to Varvel and co-workers [23]. A MdPE lower than 20% and a MdAPE between 20 and 40% is considered clinically acceptable [24]. Two population PK models for NE were identified in literature, which are referred to as the Beloeil’s model [9] and the Oualha’s model [10]. When predicting with Beloeil’s model, we made one assumption that the covariate Simplified Acute Physiology Score (SAPS) was set to the lowest value (30) in their dataset. This was due to the fact that Beloeil’s model was built on septic shock and trauma patients and the SAPS does not extrapolate to healthy individuals.
2.4 Simulation
The final PK model was used to predict expected changes in NE PK during general anesthesia at different measured propofol concentrations. The simulation dataset was built based on the model development dataset and included all significant covariates. A typical target concentration of propofol for maintaining general anesthesia (3 mcg/mL–1) was chosen for the simulation, as well as a high concentration (6 mcg/mL–1) and absence of propofol for comparison. An infusion for 15 minutes at a dosage of 0.12 mcg/kg-1/min–1 was used for the simulation. For each patient, 1000 simulations were performed and summarized at a population level. All simulations were performed with the RxODE2 package (version 2.0.14) in R.


Comments (0)