In this study, we used a PBPK-based workflow to investigate how sensitive and specific changes in plasma clearance of commonly used CYP probe drugs are in detecting alterations in in vivo CYP enzyme activity, quantified as CLint. This is particularly relevant when the probe drugs are used to assess changes in enzyme activity in the context of (patho)physiological conditions, such as inflammation, obesity, or pregnancy [4,5,6].
Plasma clearance of all probe drugs was sensitive to alterations in CYP enzyme activity, as changes in plasma clearance demonstrated a close to proportional relationship with alterations in CLint, except for midazolam. One of the validation criteria for phenotyping metrics states that the metric should not depend on factors beyond enzyme activity, meaning the metric should not be sensitive to, amongst others, the non-metabolic variables fu, B/P, and Qh that were studied in this work [2]. Importantly, our results highlight that plasma clearance of all probe drugs was equally sensitive to alterations in protein binding as to alterations in CLint, highlighting that alterations in fu might impact the phenotyping metric. This will not affect the use of cocktail approaches to assess differences in enzyme activity in scenarios where fu remains unchanged, for example in traditional pharmacokinetic interaction studies investigating drug–drug and/or drug–gene interactions, since these interactions are linked to changes in the levels or activity of CYP enzymes only and studied in healthy volunteers. However, it does indicate that additional methodological approaches are required to account for changes in fu, if the cocktail approach is applied to study scenarios where fu might change, as illustrated in this work for inflammatory conditions. Taking the alterations in fu into consideration as a confounder that can impact the phenotyping metrics will improve the validity of the metric during (patho)physiological conditions. Practically, this would involve the measurement of fu through measuring both total and unbound drug concentrations in patient populations to evaluate how this parameter is impacted as compared with a healthy population. Subsequently, these values can be used as input for the dispersion model to derive changes in enzyme activity (CLint) from changes in plasma clearance. An R script was provided in Online Resource 3 for the practical implementation of this method.
Midazolam is a widely acknowledged probe for phenotyping in vivo CYP3A4 activity. Interestingly, our results for midazolam show that changes in its plasma clearance are not proportional to changes in CLint, when CLint increases more than 50%. This might not have implications for, for example, inflammatory conditions, since CYP3A4 activity is known to decrease under these conditions [14]. However, midazolam is often utilized to study CYP3A4 induction in clinical DDI studies, when a disproportional relationship between increased CLint and midazolam plasma clearance could become relevant, because with high induction the observed increase in midazolam plasma clearance will be less than the increase in in vivo CYP3A4 activity. We found that midazolam clearance is also sensitive to alterations in fu, B/P, and Qh, which is in line with its intermediate extraction ratio [15]. The importance of this sensitivity towards non-metabolic determinants was recently highlighted in an obese study population [16]. This study showed that midazolam clearance in obese patients was higher as compared with controls, contrary to what would be expected given the decrease in hepatic CYP3A activity with increasing body weight. Given that patients with severe obesity have a higher Qh [17], this study suggested that increased Qh may have a more significant role than CLint changes on plasma clearance of midazolam in this patient population. Particularly for midazolam, it may therefore be required to measure and account for alterations in Qh and B/P, as well as for changes in fu, when using it as a phenotyping probe for measuring in vivo CYP3A4 enzyme activity in (patho)physiological conditions.
Our findings on probe sensitivity and specificity are in line with the general notion that clearance of low extraction ratio drugs is limited by both fu and CLint, while drugs with a high extraction ratio are mainly limited by Qh. It is therefore unlikely that probe drugs that are sensitive to changes in CLint, but not sensitive to changes in fu, will ever be identified. One way to circumvent issues with changes in fu, is to select probe drugs with low protein binding, as our results show that low protein binding probe drugs are likely less impacted by alterations in fu as compared with probe drugs that are highly protein bound. Given that information on alterations in fu during inflammatory or other (patho)physiological conditions is scarce, inclusion of fu measurements in study designs will increase our understanding of the magnitude of alterations in fu during disease and whether they impact clearance of probe drugs. In the absence of (literature) data on disease-driven changes in fu, assumptions can be made. We assumed that all probe drugs exclusively bind to HSA and calculated fu changes based on reported alterations in HSA levels in RA, surgery, and COVID-19 patients. This is a limitation considering inflammation is also characterized by upregulation of α-1-acid glycoprotein (AGP) and other proteins that may impact fu [18]. However, the affinity of probe drugs to AGP is unclear, as is the exact value of upregulation under various (patho)physiological conditions. The effects of alterations in drug binding proteins on fu may contradict and counterbalance each other, potentially clarifying why the fu of midazolam remained unaffected in COVID-19 patients, contrary to reported HSA alterations [19]. Therefore, measured fu values should be considered to be the golden standard in this context.
Incorporation of the impact of (patho)physiological conditions on drug exposure to advance personalized medicine is a long-standing goal. Several phenotyping cocktail studies have been conducted to characterize how (patho)physiological conditions such as non-alcoholic fatty liver disease, obesity, diabetes or inflammatory conditions can affect drug clearance [4, 16, 20,21,22,23,24]. Incorporation of phenotyping results into clinical guidelines has indeed been demonstrated in special patient groups, e.g. pregnant women, where results from phenotyping studies were utilized to estimate alterations in CYP-mediated drug clearance [25]. One important consideration here is that the phenotyping methodology assumes that drug exposure can be predicted by the pharmacokinetics of a relevant probe drug with a shared metabolic pathway. Indeed, the EMA guidelines on DDIs state that results of cocktail studies can be extrapolated to other drugs and can be used to support treatment recommendations in the SmPC [26]; however, these results may not always be directly translatable between drugs. Our result highlighted that plasma clearance of probe drugs might also be impacted by alterations in fu, and to a lesser extent B/P and Qh, with the extraction ratio of the drugs determining which parameters are most influential. When findings from phenotyping cocktails in (patho)physiological conditions are used to make inferences about plasma clearance of other drugs, potential differences in fu, B/P, and Qh need to be accounted for, particularly when the extraction ratio of the drug that the finding is extrapolated to is higher. To achieve this, the equations of the dispersion model can be used.
Our results suggest that alterations in fu observed during inflammatory conditions such as COVID-19, RA, or surgery may influence CLint predictions derived from differences in plasma clearance. Of note, our research did not aim to study the impact of inflammation on CLint, but rather to assess the accuracy of the cocktail approach used to quantify such impact. Inflammation is known to affect liver function, induce oxidative stress, and modulate CYP enzyme activity through the release of proinflammatory cytokines [27]. While the broader question of how inflammation impacts drug clearance and plasma concentrations has been well-studied by others [28, 29], our focus is on providing tools and insights to improve the interpretation of clinical phenotyping studies that assess the overall effects of these inflammation-related mechanisms on CYP enzyme activity.
Our approach focused on the plasma clearance of probe drugs, but the primary metric used in phenotyping studies is the metabolic ratio in plasma or urine at a specific time point. The ratio of metabolite to parent concentrations in plasma indeed increases when plasma clearance increases, however this ratio also changes continuously over time within each individual, causing the method to be sensitive to deviations in sampling time. Moreover, the plasma concentration of both the metabolite and parent drug may be impacted by alterations in distribution volume or equilibration to peripheral tissue, while, in addition, the metabolite concentration may also be impacted by alterations in its elimination rate [26]. Especially in diseased study participants, these processes may all be altered. When employing urine sampling, variations in urinary pH and glomerular filtration rate may further impact the measured metabolic ratio [30, 31]. Considering that all these disease-driven alterations could lead to changes in the metabolic ratio that are independent of changes in enzyme activity, taking multiple plasma samples and calculating plasma clearance may be more appropriate to study in vivo enzyme activity under (patho)physiological conditions. Finally, our approach focused on systemic plasma clearance of probe drugs, while the probe drugs are typically administered orally. Disease-related changes in pre-systemic clearance (i.e., gut and first-pass metabolism) would impact oral bioavailability (F) and thereby the apparent oral clearance (CL/F) that is obtained in cocktail studies. As quantitative information on disease-related changes in pre-systemic clearance pathways is limited, this could not be included in our PBPK assessment.
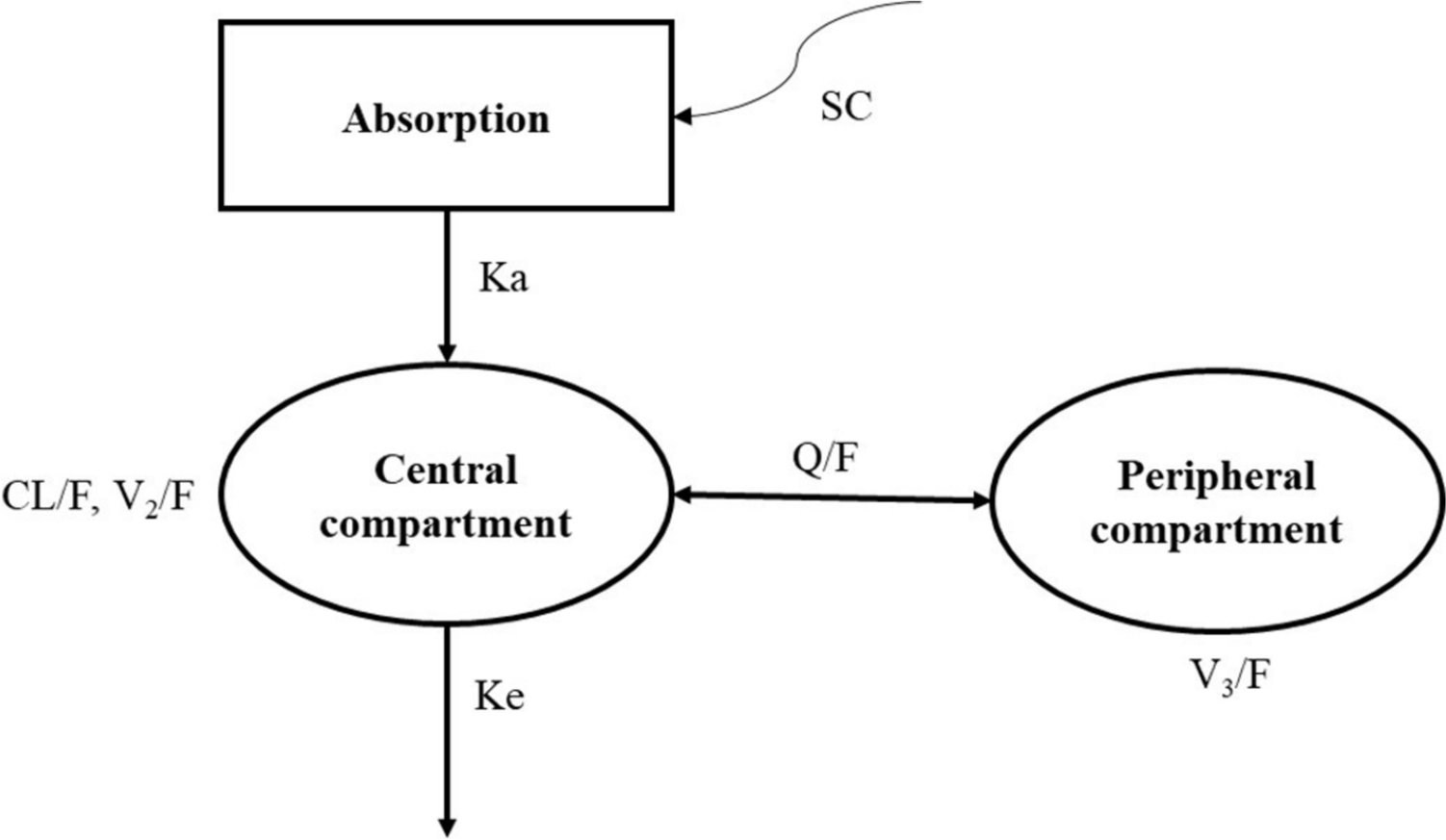
A limitation that applies to clinical plasma clearance values is that probe drugs are never exclusively eliminated through metabolism by a single isoenzyme and that minor elimination pathways will impact the concentration of the parent compound. The PBPK approach applied in the current analysis allows for studying the major elimination routes in isolation, which would be impossible to do in vivo and which is an advantage for establishing sensitivity and specificity of the drugs in phenotyping cocktails. Due to limited information on intrinsic hepatic transporter activity for most probe drugs, the applied PBPK framework does not incorporate the influence of hepatic influx or efflux transporters, but as far as we know, hepatic transporters are not major contributors to the plasma clearance of the studied probe drugs, which reduces the impact of this limitation on our findings. Finally, we describe the influence of univariate changes in CLint, fu, B/P, and Qh on plasma clearance. Multiple parameters could change simultaneously under (patho)physiological conditions, leading to additive, synergistic or antagonistic effects due to the non-linearities in the dispersion model between plasma clearance and the model parameters. Conducting a multivariate analysis investigating all possible combinations of changes in all four variables would exponentially increase the number of scenarios to be evaluated and further challenges the interpretation of the results. Despite the fact that univariate changes in B/P and Qh limitedly impact probe drug plasma clearance, a combination of changes in parameters might have a more significant impact. Specifically, changes in Qh could become more important in scenarios where CLint increases, while changes in B/P will be more relevant when the fu is considerably impacted by altered partitioning of drugs into red blood cells. With the provided R script in Online Resource 3, the reader can derive changes in CLint for any drug, based on the difference in CLp and any possible combination of changes in fu, B/P, and Qh.


Comments (0)