
Remember me



Written informed consent was obtained from each patient for the publication of this case report.
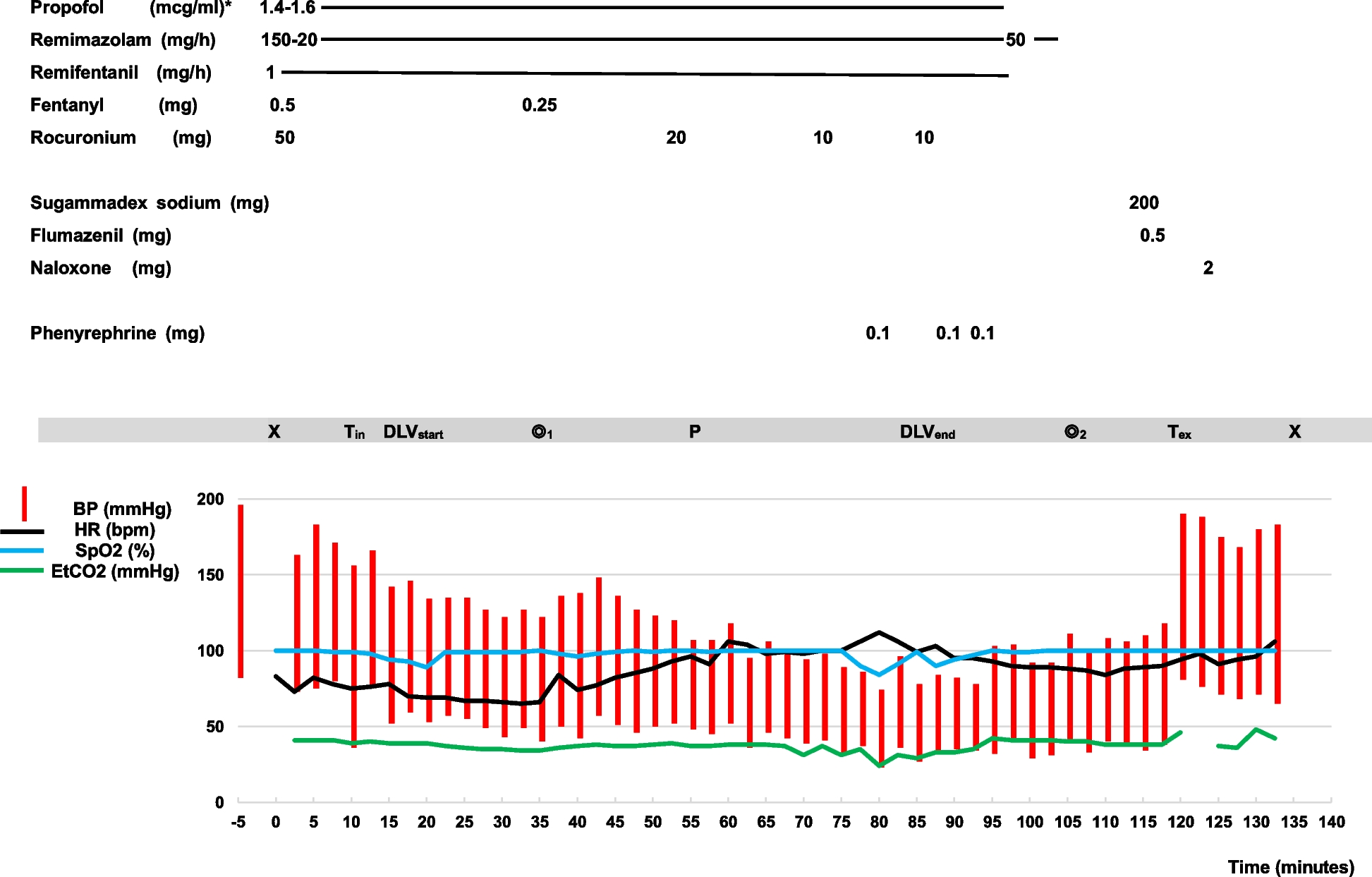
Case 1The patient was a 96-year-old man (height, 160 cm; weight, 47.4 kg) with an enlarged abdominal aortic aneurysm of 53 mm in size, for which invasive treatment was considered. In a preoperative medical examination, transthoracic echocardiography showed severe AS with an aortic valve peak velocity of 4.2 m/s, calculated aortic valve area of 0.52 cm2 and circumferential left ventricular wall thickening. Left ventricular ejection fraction was maintained at 70.4%. Coronary angiography revealed a complex three-vessel coronary artery lesion with a SYNTAX score of 34. In addition, he had anemia with a hemoglobin level of 8.2 g/dL, hypertension, dyslipidemia, and hypokalemia with a potassium level of 2.9 mEq/L. After thorough consultation with the Heart Team, hybrid surgery of TAVI plus OPCABG was scheduled in preference to abdominal aortic aneurysm surgery. The surgical strategy was to first perform revascularization of the left anterior descending artery (LAD) with left internal thoracic artery bypass followed by TAVI via the trans-aortic approach and then perform complete revascularization by bypassing the right coronary artery and left circumflex artery.
An oximetry catheter (PreSep; Edwards Life Sciences, LLC, Irvine, CA, USA) and a continuous arterial pressure line with hemodynamic monitoring (FloTrac; Edwards Life Sciences, LLC, Irvine, CA, USA) were inserted while the patient was awake. A BIS device and a near-infra-red spectroscopy device (INVOS 5100; Somanetics, Troy, MI, USA) were fitted in addition to standard monitoring. General anesthesia was induced with a total of 200 µg of fentanyl in divided doses and remimazolam at 6 mg/kg/h along with continuous administration of noradrenaline at 0.05 µg/kg/min. After the patient lost consciousness, 0.6 mg/kg rocuronium was administered. No significant circulatory changes were observed during tracheal intubation. Anesthesia was maintained with a total of 1000 μg fentanyl in divided doses and remimazolam was adjusted to 0.3–0.4 mg/kg/h to achieve BIS values between 40 and 60. Hemodynamic change during surgery is shown in Fig. 1. During coronary artery bypass to the LAD, hemodynamics were stable with CI 2.6 L/min/m2 and SVRI around 1300 dyne sec/cm5 with the administration of 0.15 μg/kg/min noradrenaline and 2 μg/kg/min dobutamine. TAVI using a balloon-expandable bioprosthetic valve (sapien3; Edwards Lifesciences, Irvine, CA, USA) was then performed. The procedure could be completed without circulatory collapse with an additional 0.01 mg bolus of noradrenaline during pre-dilatation balloon aortic valvuloplasty and deployment under rapid pacing. The surgery was then completed, although vasopressin was temporarily required during the right coronary artery and left circumflex artery bypass. Remimazolam was switched to propofol at 2 mg/kg/h and dexmedetomidine at 0.4 μg/kg/h and the patient was moved to the ICU under sedation with intubation. Total operative time was 210 min and anesthesia time was 281 min. He was extubated the day after surgery and discharged from the ICU on the second postoperative day. He was discharged without complications on postoperative day 34.
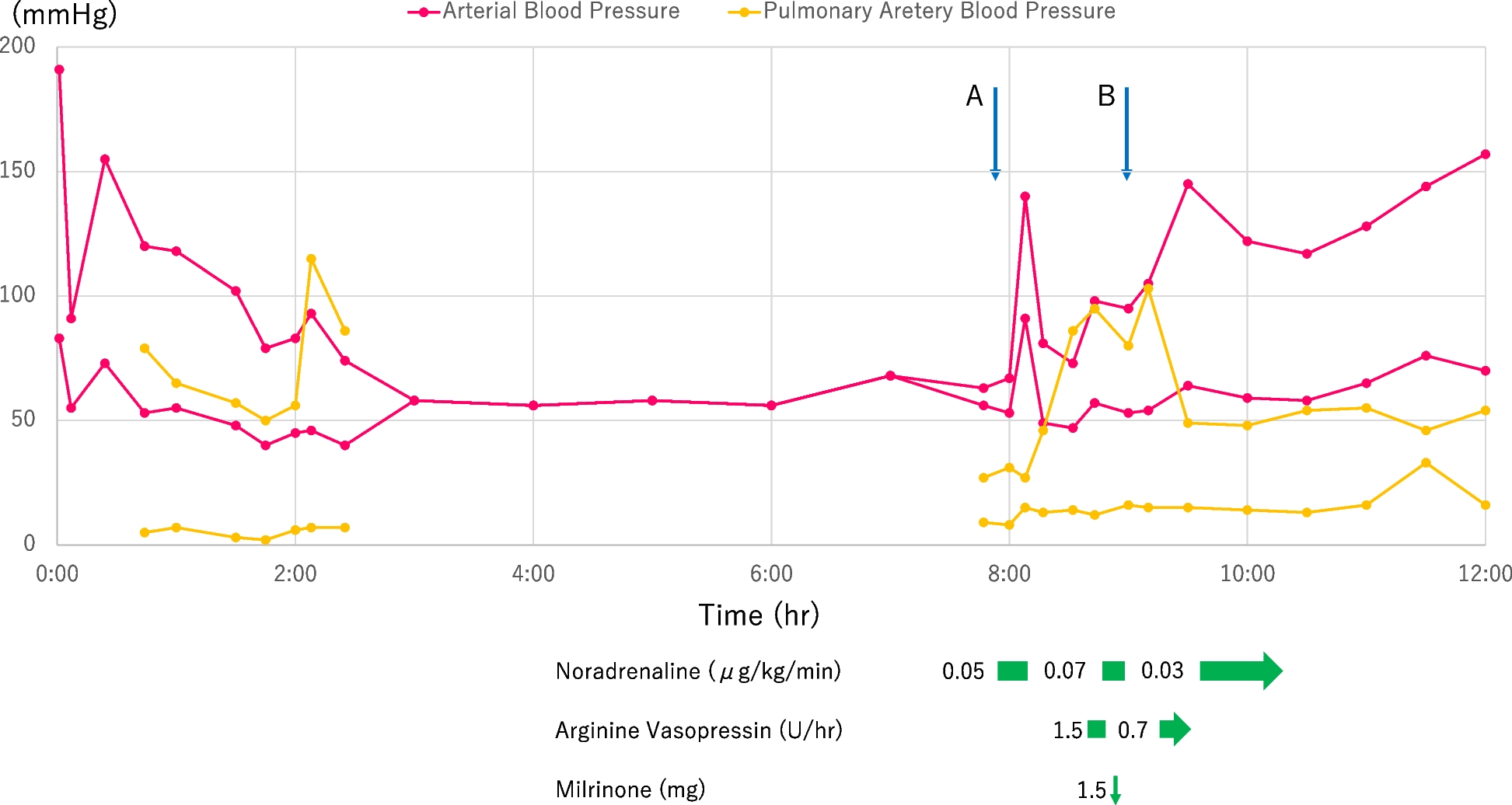
Fig. 1
Anesthesia record for case 1. The down arrow represents intubation. Double circles represent the start/end of surgery. HR: heart rate; sBP: systolic blood pressure; dBP: diastolic blood pressure; BIS: bispectral index; CI: cardiac index; SVRI: systemic vascular resistance index; rSO2: regional cerebral oxygenation measured by near-infrared spectroscopy; CABG: coronary artery bypass grafting; TAVI: transcatheter aortic valve implantation; LAD:left anterior descending; LCx: left circumflex artery; RCA:right coronary artery
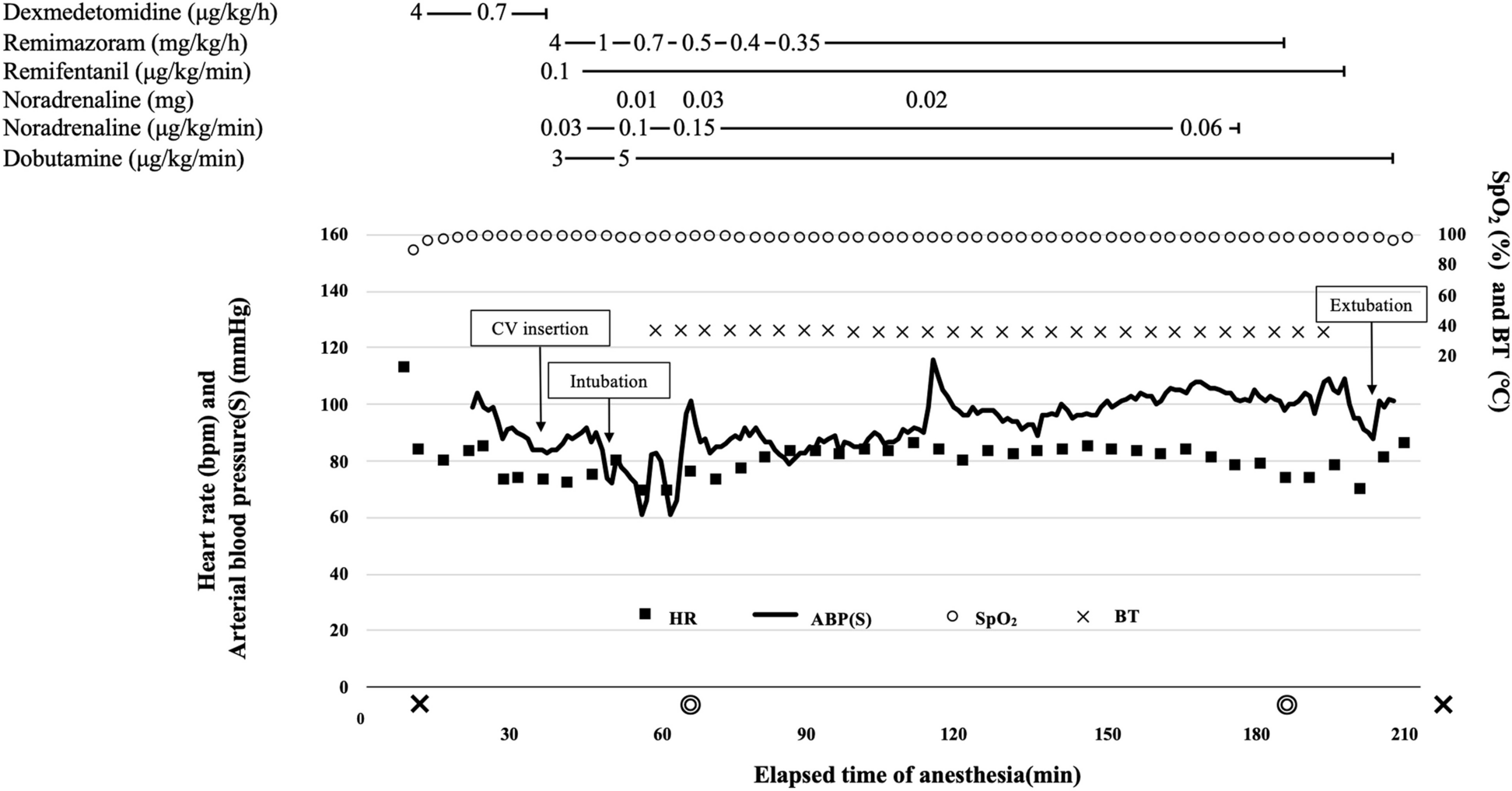
Case 2The patient was a 92-year-old woman (height, 143 cm; weight, 47.1 kg) with dyspnea on exertion. Echocardiography revealed severe AS with an aortic valve peak velocity of 4.2 m/s, calculated aortic valve area of 0.44 cm2, and circumferential left ventricular wall thickening. Left ventricular ejection fraction was 69.4%. Coronary angiography revealed a three-vessel coronary artery lesion. Percutaneous coronary intervention to stenosis at the ostia of the right coronary artery was deemed difficult. Other complications included severe bilateral lower artery stenosis, severe stenosis of the right carotid artery, chronic atrial fibrillation, old cerebral infarction, hypertension, and dyslipidemia.
The surgical and anesthesia strategy was the same as that for case 1. General anesthesia was induced with a total of 300 µg of fentanyl in divided doses and remimazolam at 6 mg/kg/h without any vasopressor. After the patient lost consciousness, 1 mg/kg rocuronium was administered. No significant circulatory changes were observed during tracheal intubation. Anesthesia was maintained with a total of 1000 μg fentanyl in divided doses and remimazolam adjusted to 0.3–0.4 mg/kg/h in order to achieve BIS values between 40 and 60. and remimazolam adjusted to 0.5–0.6 mg/kg/h in order to achieve BIS values between 40 and 60. Hemodynamic change during surgery is shown in Fig. 2. During coronary artery bypass to the LAD, hemodynamics was stable with CI 2.1 L/min/m2 and SVRI around 1800 dyne sec/cm5 with the administration of 0.1 μg/kg/min noradrenaline and 2 μg/kg/min dobutamine. TAVI using a self-expanding supra-annular bioprosthetic valve (Evolut pro; Medtronic Inc., Minneapolis, MN, USA) was then performed. The procedure could be completed without circulatory collapse with an additional 0.01 mg bolus of noradrenaline during deployment under control pacing and three rapid pacing. The surgery was then completed although high-dose catecholamines including vasopressin were temporarily required during the right coronary artery and the left circumflex artery bypass. Remimazolam was switched to propofol at 2 mg/kg/h and dexmedetomidine at 0.4 μg/kg/h and the patient was moved to the ICU under sedation with intubation. The total operative time was 283 min, and the anesthesia time was 360 min. She was extubated the day after surgery and discharged from the ICU on the second postoperative day. She was discharged without complications on postoperative day 18.
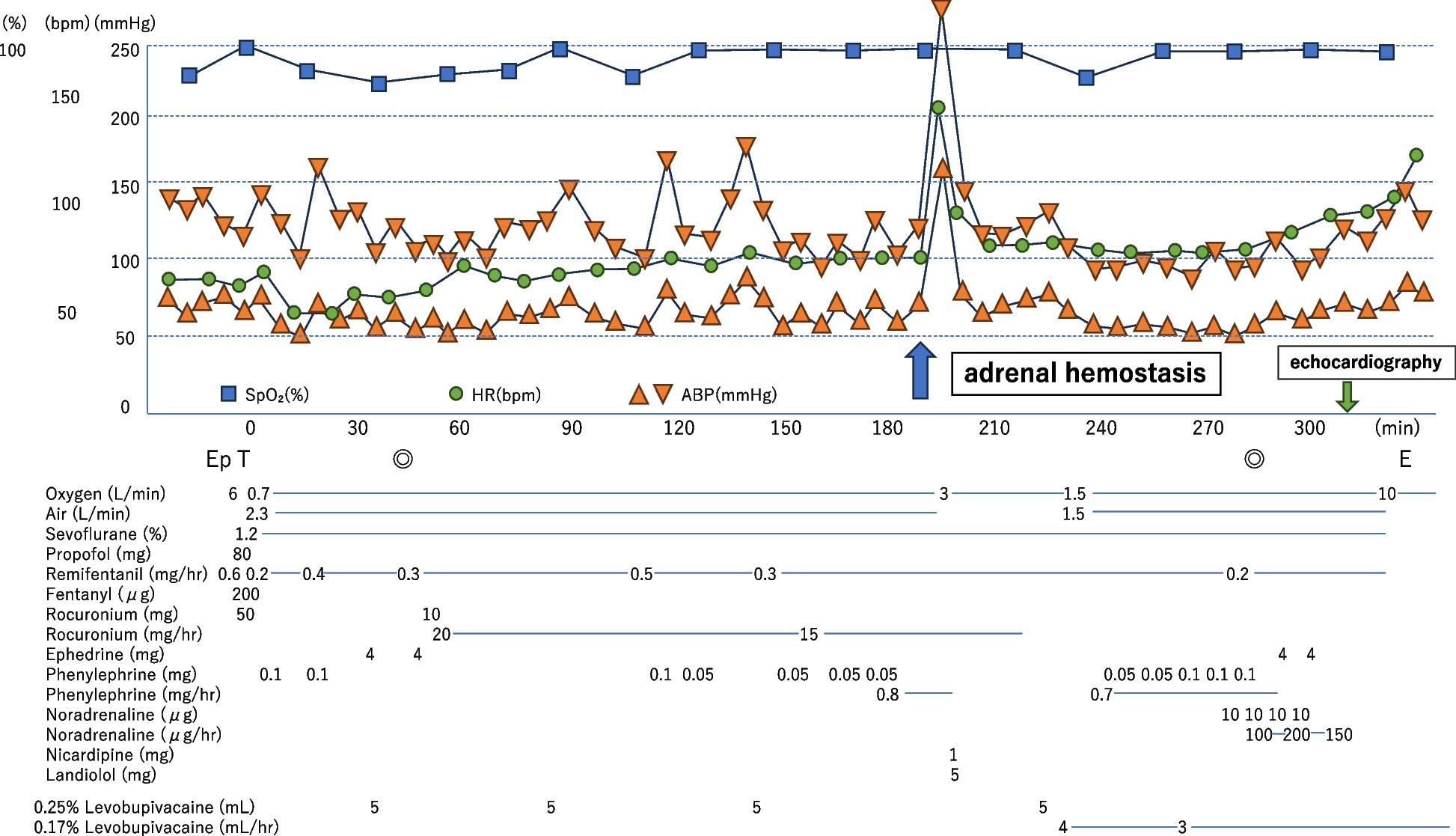
Fig. 2
Anesthesia record for case 2. The down arrow represents intubation. Double circles represent the start/end of surgery. HR: heart rate; sBP: systolic blood pressure; dBP: diastolic blood pressure; BIS: bispectral index; CI: cardiac index; SVRI: systemic vascular resistance index; rSO2: regional cerebral oxygenation measured by near-infrared spectroscopy; CABG: coronary artery bypass grafting; TAVI: transcatheter aortic valve implantation; LAD:left anterior descending; LCx: left circumflex artery; RCA:right coronary artery
Comments (0)