
Remember me



A 71-year-old woman (142 cm, 42 kg) with aortic valve stenosis, pulmonary valve stenosis, and angina pectoris underwent aortic valve plasty, pulmonary valve plasty with an autologous pericardium (Ozaki procedure), and coronary artery bypass surgery. Her medical history included bronchial asthma, hypertension, and type II diabetes mellitus. She developed a cerebral infarction at the age of 60 years without sequelae. The patient’s preoperative status was New York Heart Association Class II. A preoperative transthoracic echocardiogram showed a left ventricular ejection fraction of 61%, tricuspid annular plane systolic excursion of 12 mm, severe aortic stenosis with valve area of 0.47 cm2, mean peak gradient of 83 mmHg. Severe pulmonary valve stenosis with maximum velocity of 5 m/s and tricuspid regurgitation with peak gradient of 130 mmHg were also shown. Preoperative catheter examination revealed a pulmonary artery pressure of 26/12/19 mmHg (systolic/diastolic/mean), Right ventricular pressure of 167/7 mmHg, right atrial pressure of 13/4/4 mmHg, and aortic pressure of 158/86/16 mmHg. Blood test results were unremarkable except for N-terminal pro-brain natriuretic peptide of 2756 pg/ml.
With monitoring of arterial blood pressure and electroencephalogram besides standard monitoring, general anesthesia was induced with propofol 60 mg, remifentanil 0.4 µg/kg/min, rocuronium 40 mg, and maintained with sevoflurane 1.0–1.5% with remifentanil 0.15–0.3 µg/kg/min. A pulmonary artery catheter inserted via the right jugular vein was not advanced to the pulmonary artery due to pulmonary valve stenosis and was placed in the right ventricle. The hemodynamic parameters were stable with systolic arterial blood pressure (SAP) of 120 mmHg; central venous pressure (CVP) of 6 mmHg, right intraventricular pressure of 79/5/24 mmHg measured by pulmonary artery catheter, although right intraventricular pressure occasionally exceeded systemic blood pressure.
The surgery was performed as planned preoperatively. First, the aortic valve was repaired with autologous pericardium. Next, the pulmonary valve was also repaired using the Ozaki procedure. The operator removed damaged leaflets and measured intercommissural distance using a sizer. After that, he cut the pericardium on the template. The aortic valve was repaired with autologous pericardium left coronary cusp 21 mm, right coronary cusp 23 mm and non-coronary cusp 23 mm, which formed by using Ozaki template. All three cusps of the pulmonary artery valve were formed 24 mm by the template. Cardiopulmonary bypass was finished 427 min after the start of surgery. The outlet of the pulmonary artery was enlarged, and coronary artery bypass grafting was performed. Before completion of the surgery, the pulmonary artery catheter was advanced into the pulmonary artery by the surgeon.
Upon the weaning of cardiopulmonary bypass, continuous infusion of dopamine 5 µg/kg/min and norepinephrine 0.05 µg/kg/min were initiated. Systemic hypotension persisted despite an increased continuous infusion dose and bolus of norepinephrine. Systemic arterial blood pressure was 99 mmHg; CVP, 16 mmHg; and PAP increased to 98/15/44 mmHg. Bolus milrinone was not effective for decreasing PAP, and norepinephrine was replaced with arginine vasopressin (AVP) 0.2 units bolus repeatedly, followed by continuous infusion at 1.6 units/h, which effectively ameliorated pulmonary hypertension The AVP dose was reduced to 0.7 units/h and totally, administered for 40 min. The total dose was 0.9 units. Systemic arterial pressure was maintained at approximately 100 mmHg, whereas systemic PAP decreased to 44 mmHg. The PaO2/FiO2 ratio remained > 300 throughout the post-CPB period. The surgery time was 639 min. The patient was then transferred to the intensive care unit under sedation and intubated. Systolic PAP was approximately 40 mmHg until the day after surgery (Fig. 1). After admission to the ICU, with administered dopamine and dobutamine continuously, mild pulmonary hypertension (systolic PAP was 44 mmHg) remained, but hemodynamics was maintained (Cardiac Index was 2.3 L/min/m2). The tracheal tube was removed on the first postoperative day. X-rays showed phrenic nerve paralysis, but oxygenation was maintained despite a slight increase in PaCO2. Later, aspartate transaminase (AST) and alanine transaminase (ALT) increased, and right heart failure was suspected, so a transthoracic echocardiogram was performed on postoperative day 10. Then, we revealed a hematoma around the right atrium, and pericardial drainage was performed under local anesthesia. Thereafter, the patient’s condition improved, and he was discharged from the ICU on postoperative day 13.
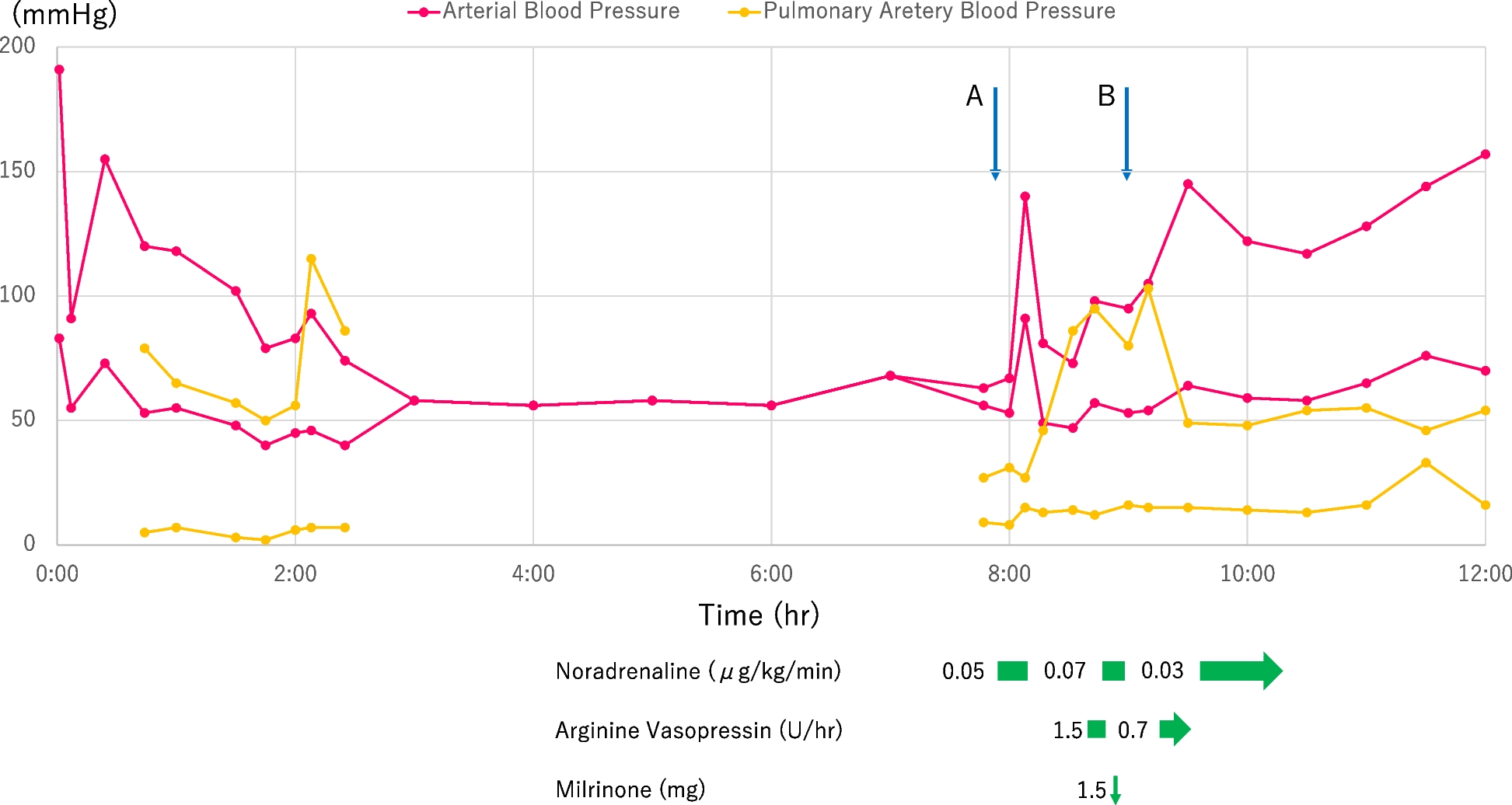
Fig. 1
Time courses of systemic arterial pressure and pulmonary arterial pressure in double-Ozaki surgery. The horizontal axis is the time from the start of anesthesia. A indicates the end of cardiopulmonary bypass. B indicates when the bolus of milrinone and the starting continuous of arginine vasopressin (AVP) was administrated
Comments (0)