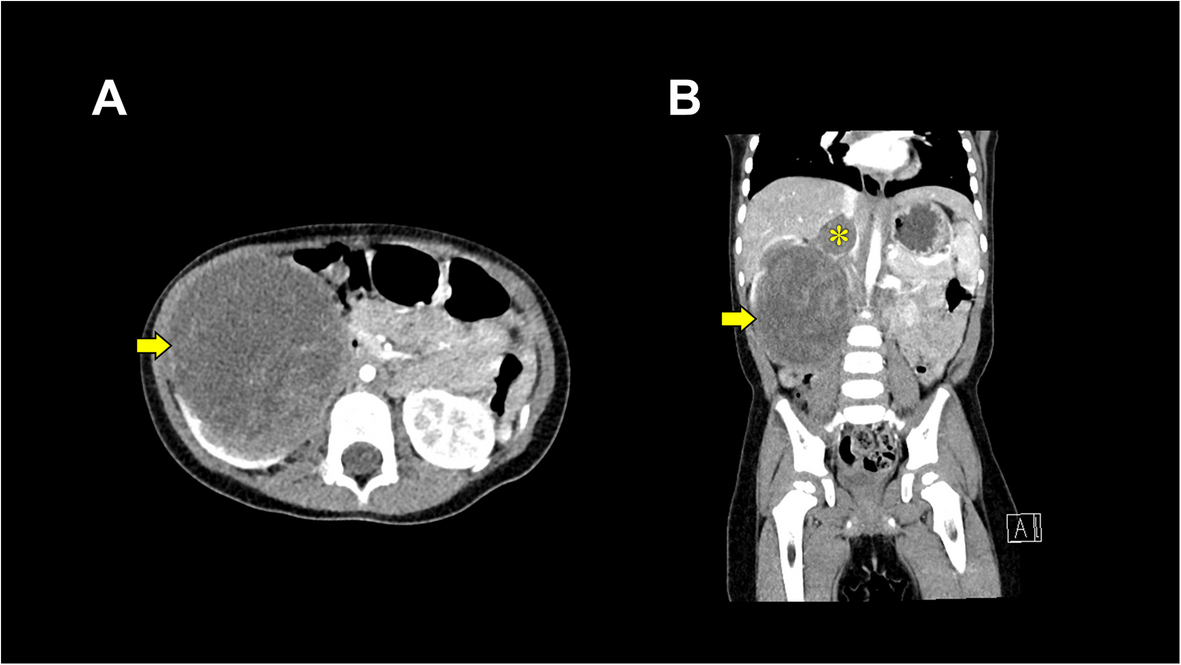
This case involved a 2-year-old boy with Wilms tumor extending into the IVC, who underwent nephrectomy. Anticipating the risk of hemorrhage, a Broviac™ catheter was placed in the right subclavian vein before tumor resection, ensuring readiness for rapid transfusion using the SL One®. We believe this strategy enabled effective management of acute hemorrhage over a short period.
In this case, there was a high risk of acute hemorrhage with significant hemodynamic impact for two primary reasons. First, because the tumor extended into the IVC and required IVC incision, the predicted blood loss was estimated to exceed 500 mL. Second, this anticipated blood loss was disproportionately large relative to the estimated circulatory blood volume of approximately 1125 mL in a 2-year-old child weighing about 15 kg [10]. In anticipation of intraoperative hemorrhage, the preoperative meeting was held with all relevant departments to share information and establish a unified treatment approach. As a result of the meeting, the original plan to place the Broviac™ catheter after the right nephrectomy was revised, and the catheter was instead inserted prior to the procedure. Consequently, we were able to utilize a secure central venous line, minimizing the risk of extravasation, and employ the SL One® for immediate high-volume transfusions.
There are two main types of rapid infusion devices: pressure infusion devices and roller pump infusion devices. An example of a pressure infusion device is the Level 1® Fluid Warming System (Smith Medical ASD, Inc., Minneapolis, MN). In contrast, examples of roller pump infusion devices include the SL One® and Belmont® Rapid Infuser RI-2 (Belmont Medical Technologies, Billerica, MA, USA). All three devices share the ability to monitor infusion pressure, warm infused fluids, and detect air bubbles. However, while the Level 1® Fluid Warming System does not automatically remove air bubbles, both the SL One® and the Belmont® Rapid Infuser RI-2 offer automatic bubble removal. Moreover, because roller pump infusion devices facilitate easier flow-rate adjustments, they may be preferable in cases requiring precise control of infusion and transfusion rates. For instance, according to each device’s instruction manual, the Belmont® Rapid Infuser RI-2 has a minimum flow rate of 2.5 mL/min, whereas the SL One® can be set as low as 0.2 mL/min. Consequently, the SL One® may be the most suitable device for finely controlled infusion and transfusion in pediatric patients. Further investigations into its use in pediatric settings are warranted.
Potential complications of massive transfusion using a rapid infusion device include hemolysis, hypothermia, air embolism, and overtransfusion [12,13,14]. In this case, however, neither hyperkalemia nor hypothermia occurred. Although the hemoglobin level at the end of surgery was 14.8 g/dL—raising concerns about possible overtransfusion of PRBCs—TEE did not reveal any signs of right heart strain during surgery. Likewise, there were no echocardiographic findings suggestive of accidental air infusion associated with the SL One®. Taken together, these observations indicate that the SL One® could be used safely in this case.
In this case, the Broviac™ catheter was inserted before surgery to use as a transfusion route via the SL One®. A Broviac™ catheter, while less infection-prone than a standard central line due to its subcutaneous tunnel, is also more invasive. In this patient, however, Broviac™ catheter placement was already planned for postoperative chemotherapy. If a tunneled central venous catheter is not indicated, a standard central venous catheter would typically suffice for rapid infusion devices, as peripheral routes risk extravasation during high-volume transfusion [15, 16].
In this 2-year-old patient with Wilms tumor predicted to substantially impact hemodynamics, blood transfusion via the SL One® through a central venous catheter successfully stabilized circulation without complications. These findings suggest that the SL One® may be a feasible option in pediatric cases, although further clinical studies are warranted.




Comments (0)