We experienced a case of hypertensive crisis during adrenal hemostasis using an electric scalpel, which resulted in Takotsubo syndrome.
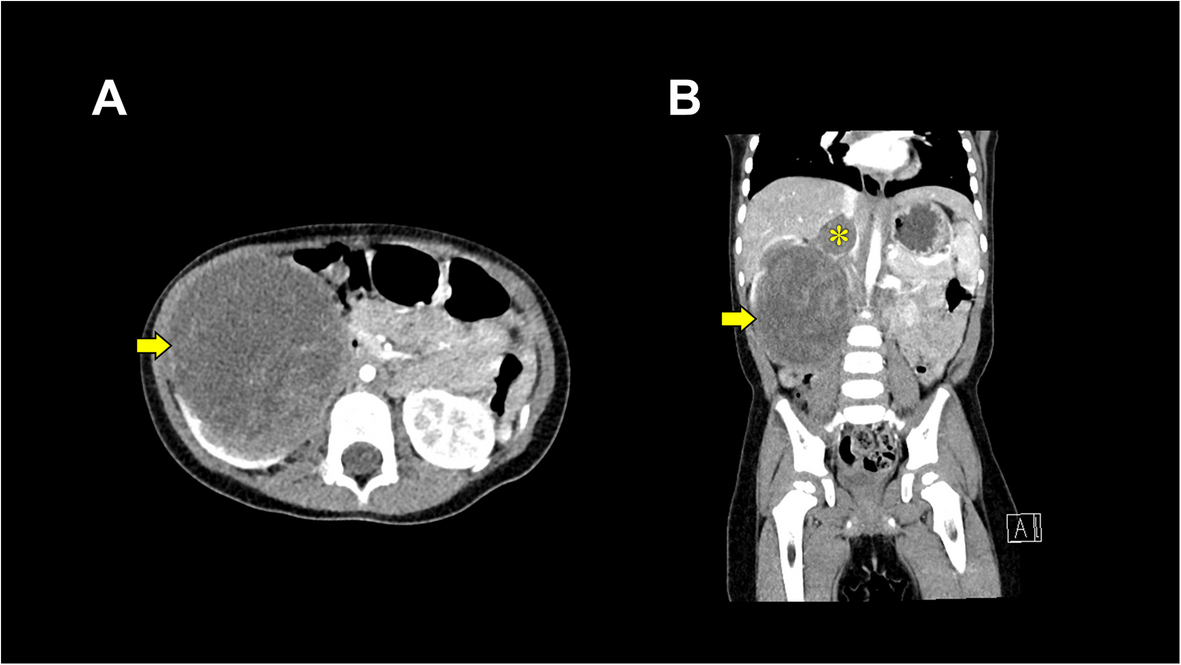
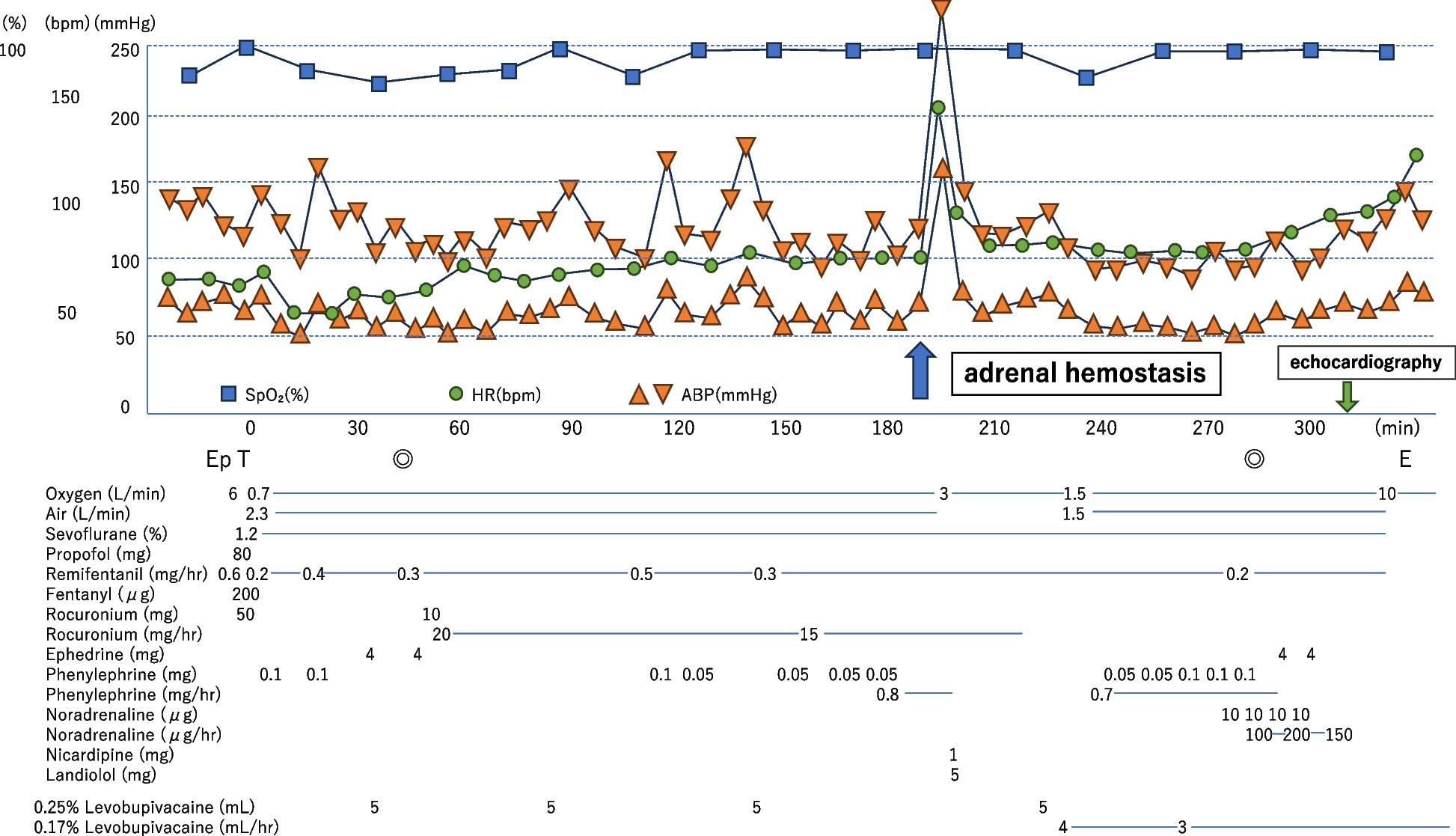
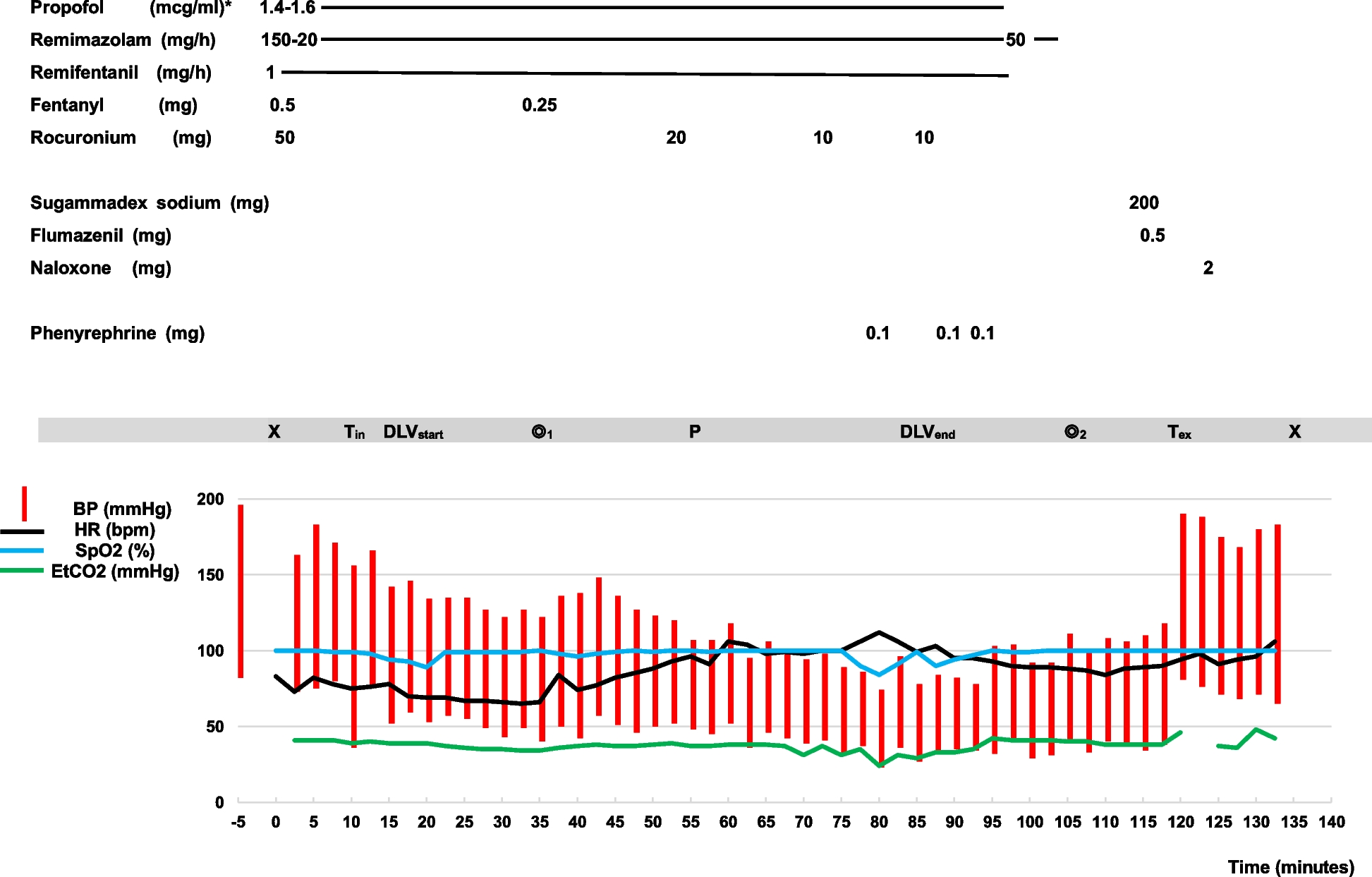
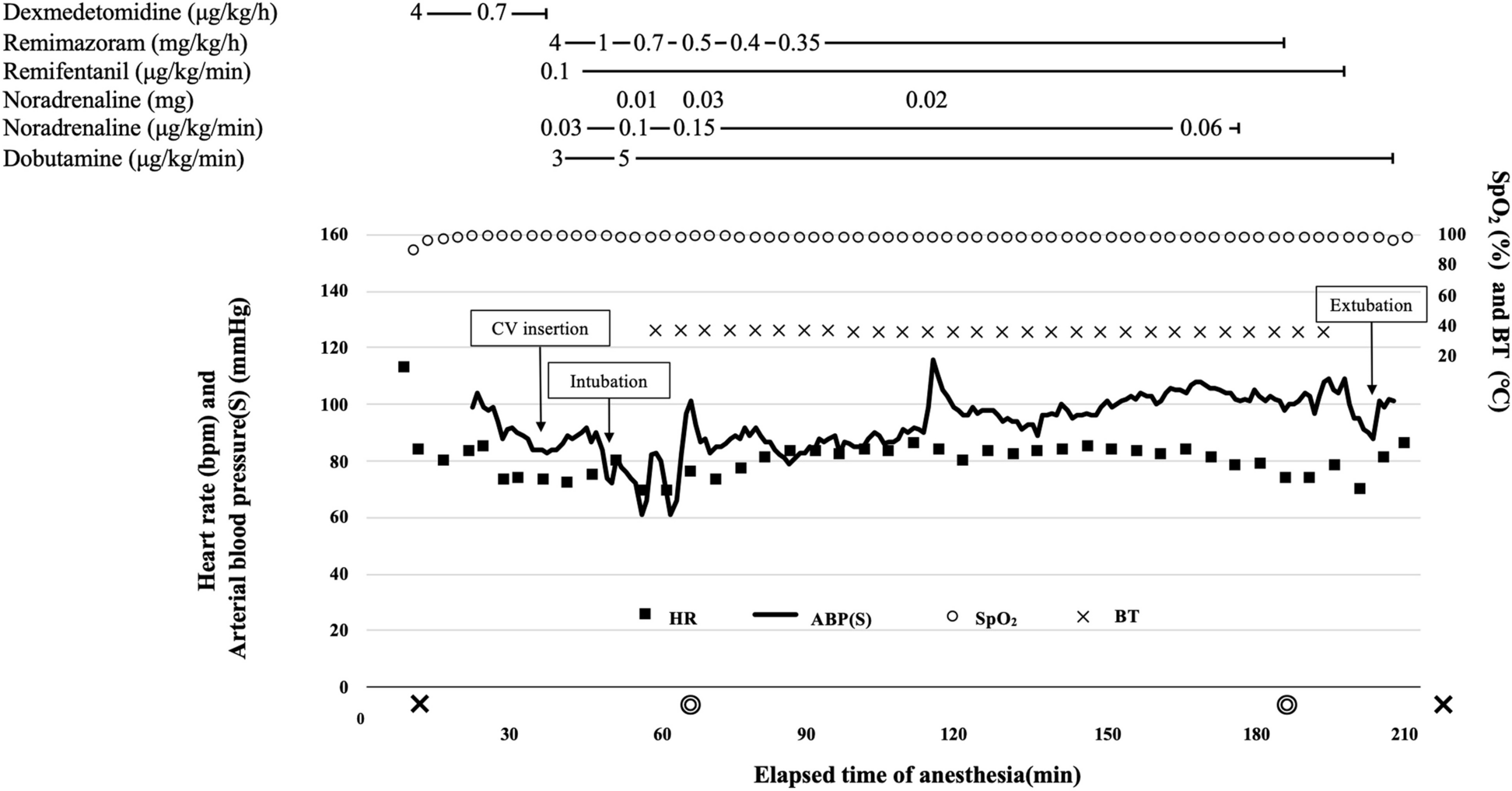
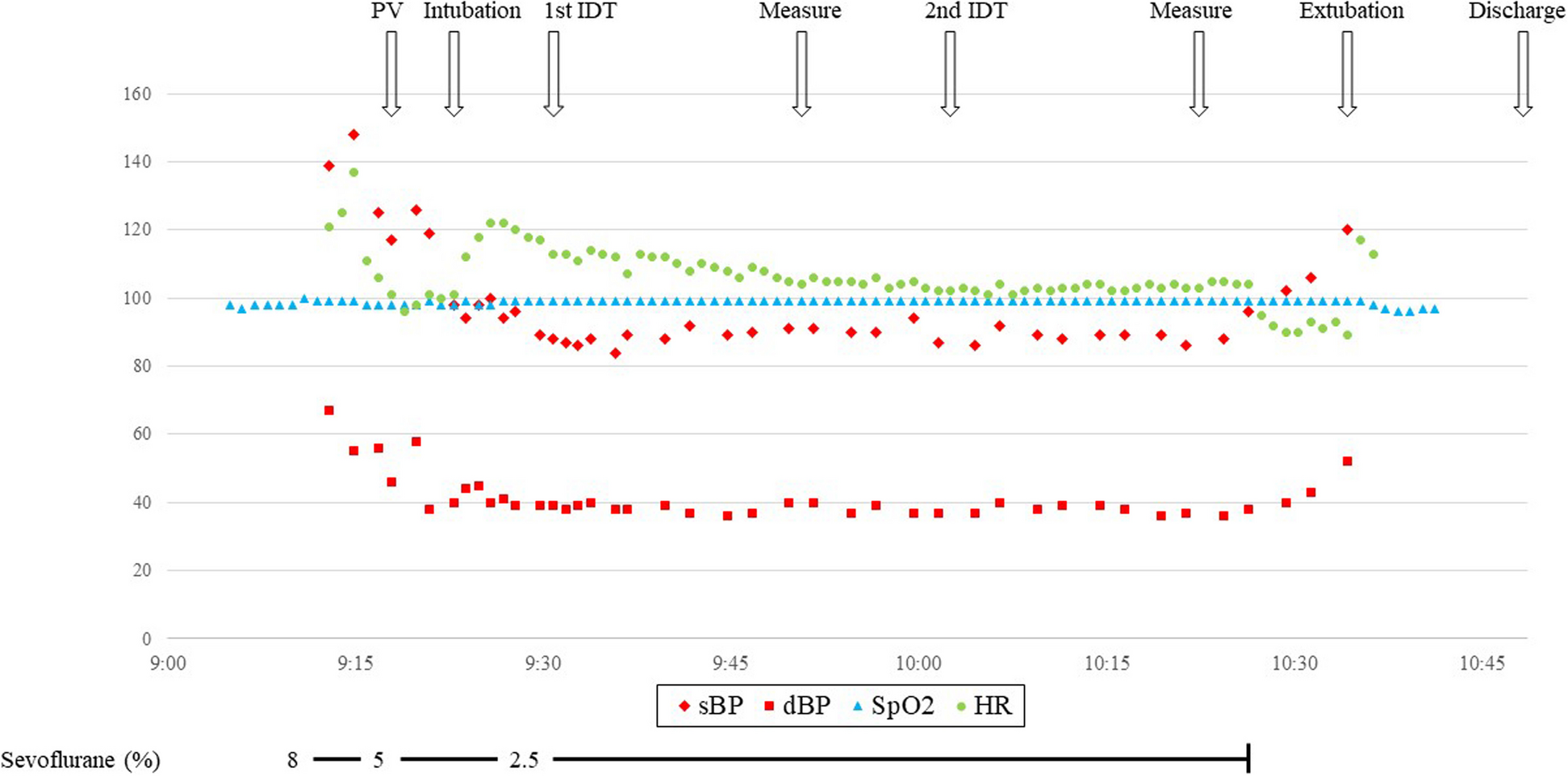
The causes of sudden abnormal intraoperative hypertension include inadequate anesthesia, hypoxia, hypercarbia, and pre-existing diseases such as essential hypertension and pheochromocytoma [7]. In this case, there was no history of hypertension or heart disease, and peripheral oxygen saturation and end-tidal cardon dioxide tension were within normal limits during anesthesia. Although preoperative adrenal hormone levels were not measured, there were no adrenal tumors, ruling out the possibility of pre-existing diseases or inadequate anesthesia for this episode.
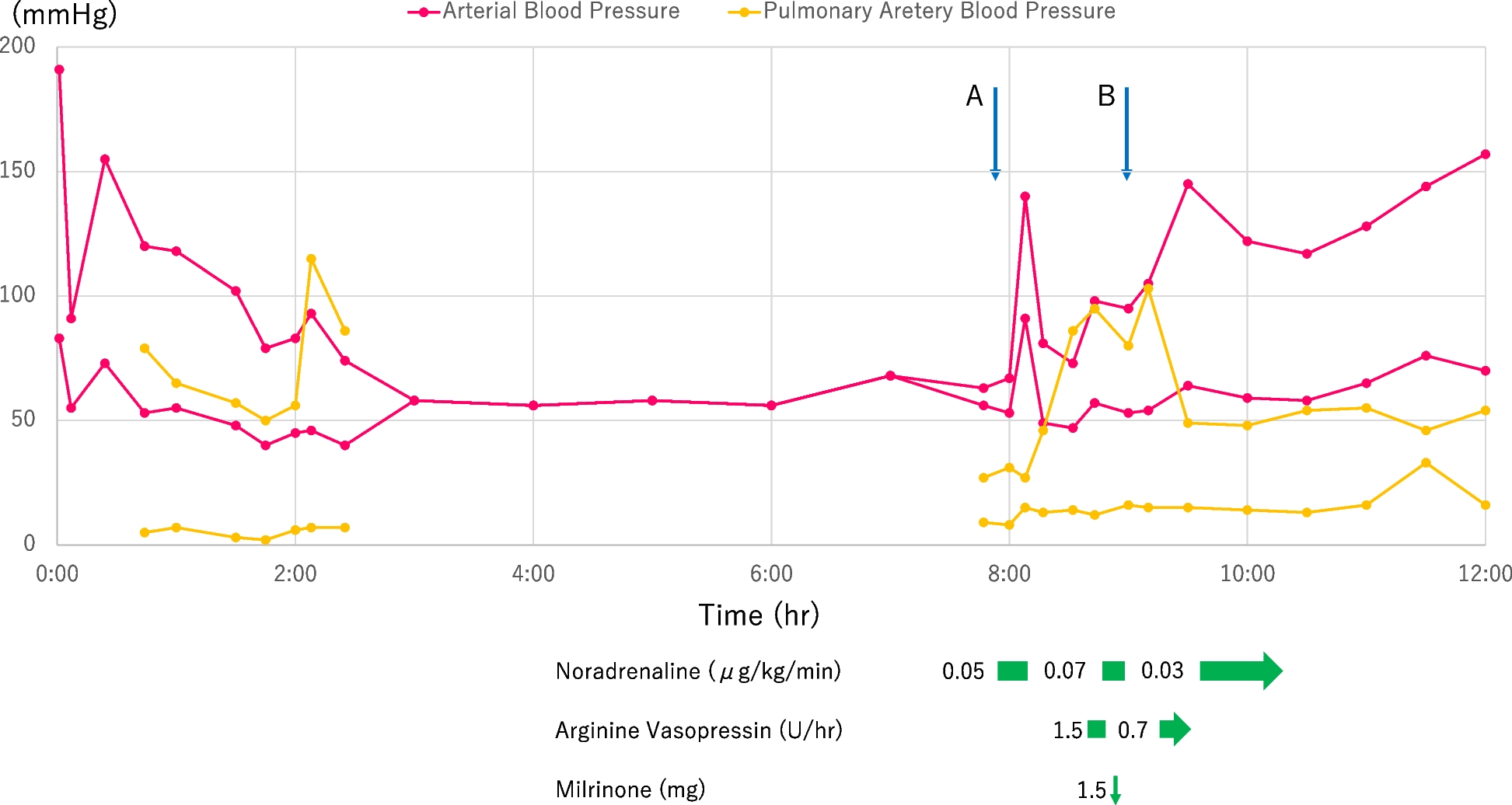
Fransson et al. reported radiofrequency ablation of normal adrenal tissue induced remarkable hypertension by an increase of blood noradrenaline levels in dogs [8]. In that report, systolic blood pressure increased to more than 200 mmHg, and blood norepinephrine levels were 39 times higher than baseline levels. This is similar to a condition caused by intraoperative manipulation of pheochromocytoma. Because catecholamine excess by pheochromocytoma is one of the causes of Takotsubo syndrome [6, 9], hypertensive crisis would be the cause of Takotsubo syndrome in this case.
To manage the abnormal hypertension caused by the release of catecholamines from the adrenal gland, we immediately ceased hemostatic manipulation and administered calcium channel blockers, as is standard in the treatment of pheochromocytoma [10], followed by beta-blockers, although there is no established protocol for dealing with this condition.
The patient was closely monitored for the onset of heart failure symptoms or potentially life-threatening arrhythmias. Fortunately, no severe complications arose, and the patient was subsequently discharged home. Takotsubo syndrome is a well-known form of reversible acute heart failure; however, it was demonstrated that in-hospital complications were comparable between patients with Takotsubo syndrome and those with acute coronary syndrome [11]. As a therapeutic strategy, the use of angiotensin-converting enzyme inhibitors or angiotensin-receptor blockers was associated with improved survival at 1 year [11].
When adrenal hemostasis is performed, it is essential to be aware of the potential risk of developing abnormal hypertension. In such cases, an arterial catheter should be placed and blood pressure should be continuously monitored. Furthermore, any impact on cardiac function may complicate intraoperative circulatory control. Therefore, adrenal hemostatic manipulation without cauterization, such as compression hemostasis and suturing, is necessary to prevent catecholamine release.




Comments (0)