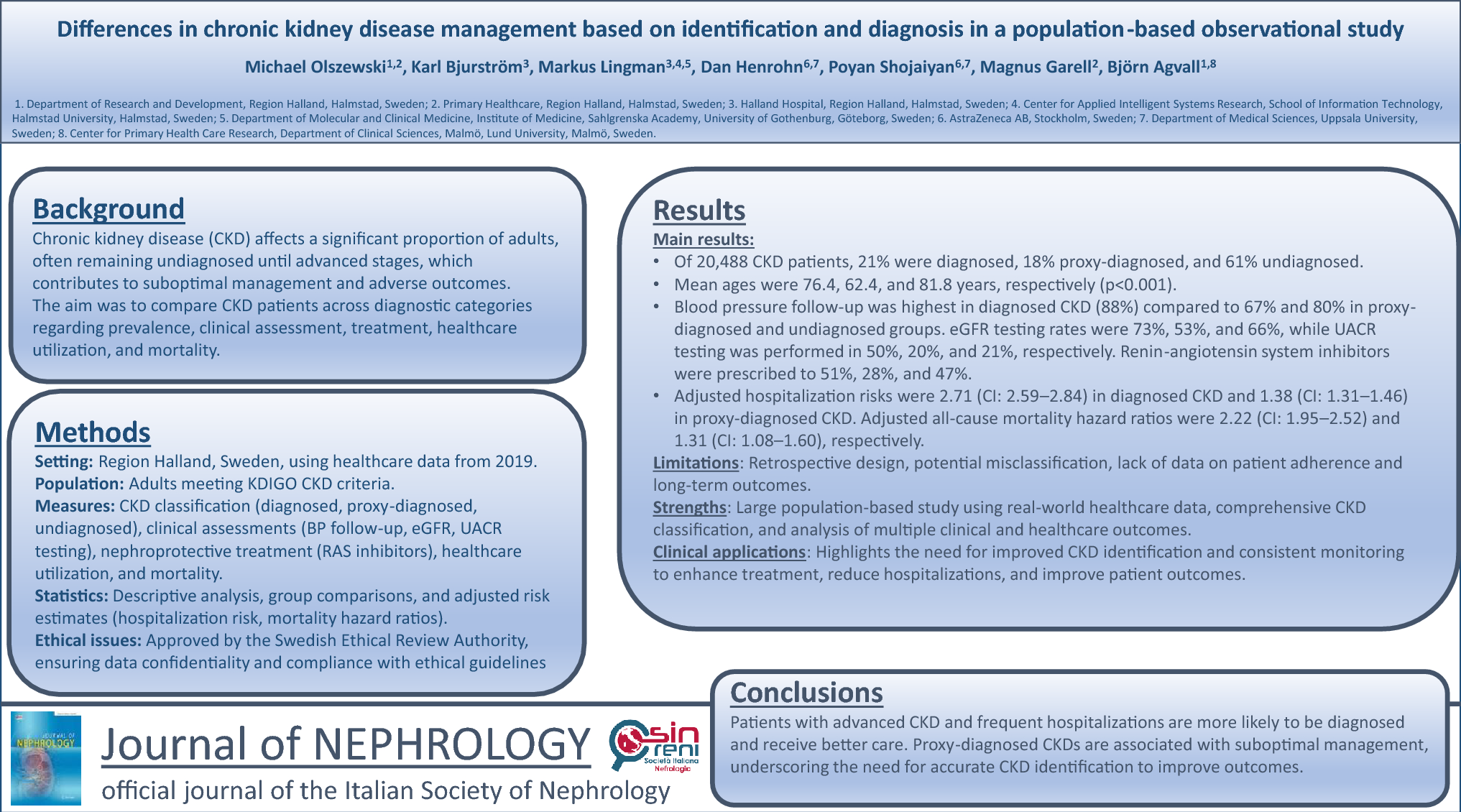
The present study reveals disparities in documentation among CKD patients. Within the cohort, 21% had diagnosed CKD, 18% proxy-diagnosed CKD, and 61% undiagnosed CKD. Patients with undiagnosed CKD were the oldest, followed by those with diagnosed CKD, while the proxy-diagnosed CKD group was the youngest. Patients with more advanced CKD stages and a higher burden of comorbidities were more likely to have diagnosed CKD and receive more comprehensive follow-up care. Both diagnosed CKD and proxy-diagnosed CKD were associated with increased hospitalization rates and greater healthcare utilization compared to undiagnosed CKD. Additionally, diagnosed CKD was associated with a higher risk of mortality than proxy-diagnosed CKD, even after adjusting for age and comorbidities.
A key contribution of this study is the identification of the proxy-diagnosed CKD group, which accounted for 18 percent of the cohort, nearly matching the proportion of formally diagnosed cases. This group likely reflects clinical recognition of kidney dysfunction without formal coding or management. Identifying this intermediate category highlights a gap in care and provides a more nuanced understanding of how CKD is documented and addressed in everyday clinical practice. CKD was diagnosed in 21% of the total cohort, which was slightly higher than the 18% or less reported in previous studies [3, 14]. The group with diagnosed CKD exhibited a higher prevalence of comorbidities and a greater number of individuals with CKD stage 3 to stage 5, which may contribute to improved diagnosis and management. Accurate recording of CKD starting from stage 3 is a crucial initial step in reducing disease progression and minimizing adverse outcomes [16, 23]. However, it is notable that 87% of individuals with undiagnosed CKD had CKD stage 3 or higher. Among those with CKD stages 3 to 5, only two-thirds underwent annual eGFR monitoring, compared to three-quarters in the diagnosed CKD group and approximately half of the patients in the proxy-diagnosed CKD group. This is still a relatively low percentage given the recommendations for annual check-ups [11, 13]. Only two-thirds of patients in the diagnosed CKD group underwent eGFR testing, and UACR testing was performed in just 50% of this group, with even lower rates in the other groups. Although UACR testing was higher in our cohort compared to other studies, these findings highlight the need for a more consistent approach to follow-up for this patient population [3, 24, 25].
RASi have been a cornerstone in the recommended treatment of CKD for many years [14]. Despite these guidelines, only 45% of the overall cohort were found to be using RASi, consistent with prior research. Among patients with diagnosed CKD, more than half were receiving RASi therapy, whereas usage was lower among those with undiagnosed CKD, and notably low (28%) in the proxy-diagnosed CKD group. Despite the proven benefits of RASi in reducing kidney failure, major cardiovascular events, and mortality in patients with CKD, its use has previously been reported at only 20.6% [26, 27]. A similar pattern was observed with statin use, which was highest among patients with a diagnosed CKD. This could be attributed to the higher incidence of ASCVD in this population and to guidelines recommending statin use for patients over 50 with CKD stages 3a to 5, regardless of cholesterol levels, if they are not on dialysis or post-kidney transplant [10, 28]. Since statin therapy was not recommended at the time of the study, there was no sub-analysis of patients eligible for statins. However, the use of RASi and statins has been associated with reduced all-cause mortality and hospital admissions in a previous study [14]. As of 2021, SGLT-2i have been recommended for CKD, but since the present study includes data referring to a period before these recommendations were implemented, it was not possible to draw any clear associations. SGLT-2i were most certainly prescribed primarily for managing diabetes, rather than for addressing renal impairment. Patients with a proxy-diagnosed CKD had lower rates of all the pharmacotherapies compared to other groups, underscoring the importance of receiving both an accurate and timely CKD diagnosis.
Individuals with a diagnosed CKD experienced more frequent hospital admissions and longer hospital stays compared to those with undiagnosed CKD or those having a proxy-diagnosed CKD. Healthcare utilization data revealed that hospital admissions and days of care were highest in the diagnosed CKD group, with rates more than double those of patients with undiagnosed CKD or with a proxy-diagnosed CKD. The relative risk for hospital days regarding the diagnosed CKD group was 2.71 (CI: 2.59–2.84), adjusted for age, sex, CKD stage, and comorbidities. This may suggest that patients were diagnosed at a more advanced stage of CKD, requiring more healthcare, or it may reflect improved recognition of CKD-related complications, prompting increased healthcare interventions. Nevertheless, these findings may partly reflect residual confounding, as diagnosed patients could represent a frailer subgroup with unmeasured factors, such as malnutrition or functional decline, influencing both healthcare use and outcomes. To further explore whether disease severity influenced the observed associations, stratified analyses by CKD stage were conducted for both hospitalization and mortality outcomes. These analyses confirmed that the associations between diagnosis status and outcomes persisted across CKD stages, although the strength of association varied. This supports the interpretation that diagnosis status itself, beyond CKD severity, is associated with differences in healthcare utilization and mortality risk. The proxy-diagnosed CKD group, consisting of younger patients with potentially earlier-stage CKD, had lower hospital admission rates and shorter hospital stays. The frequency of primary care visits showed minimal variation across all CKD groups. Even though a significant difference was observed, the number of primary care visits does not appear to be influenced to a greater extent by whether individuals have undiagnosed CKD, diagnosed CKD, or proxy-diagnosed CKD.
Previous studies have reported that mortality is associated with older age, proteinuria, and a higher prevalence of comorbidities such as ASCVD [29, 30]. The Cox regression model for all-cause mortality showed an HR of 2.22 (CI: 1.95-2.52) for patients with a formal diagnosed CKD and an HR of 1.31 (CI: 1.08-1.60) for those with a proxy-diagnosed CKD, even after adjusting for sex, age, CKD stages, and comorbidities. This suggests that a diagnosed CKD was associated with a greater number of comorbidities, such as ASCVD (HR: 1.42, CI: 1.28-1.39), and that the increased mortality risk is not necessarily driven solely by CKD, as previously reported [13]. Additionally, CKD, at stages 1 and 2, has been associated with an increased risk of both mortality and number of hospitalizations. This association was likely influenced by selection bias, as patients in these early stages often have comorbid conditions that impact these outcomes. Although this finding appears paradoxical, it has been observed in previous studies and cannot be explained by other factors [14]. In the proxy-diagnosed CKD group, the average age is notably lower, with a greater proportion of individuals in CKD stages 1-2 (60%) and a lower incidence of comorbidities. This may influence the findings regarding their need for medical care and potentially reduce the necessity for follow-up.
This study utilizes a comprehensive and well-established data source, RHIP, which provides a broad and detailed view of the CKD population within Region Halland. Moreover, the study design allows for the analysis of real-world data across various healthcare settings, including primary care, emergency departments, and specialized outpatient clinics, offering a holistic understanding of CKD management in routine clinical practice. The proxy-diagnosed CKD classification enables identification of at-risk individuals but may introduce heterogeneity due to the variable specificity of the included ICD-10 codes.
The retrospective nature of the research introduces inherent biases, such as the potential for incomplete or inaccurate ICD coding, which could underestimate the true prevalence of CKD. UACR values were not collected, which could in this context have been of value for assessing the CKD more extensively. The reliance on registry data limits the ability to capture all relevant clinical details, such as patient adherence to treatment or lifestyle factors, which could impact disease progression and outcomes. Despite adjustments for key variables such as age, sex, CKD stage, and major comorbidities, residual confounding may still be present. Unmeasured factors such as frailty, nutritional status, functional decline, or undiagnosed comorbid conditions could influence both the likelihood of receiving a CKD diagnosis and the risk of adverse outcomes. These limitations should be considered when interpreting associations between diagnosis status, healthcare utilization, and mortality. Furthermore, the study is geographically confined to Region Halland, which may limit the generalizability of the findings to other regions or countries with different healthcare systems and population characteristics. Lastly, while the study adjusts for several key variables, unmeasured confounding factors such as socioeconomic status or access to healthcare services may still influence the observed associations between CKD diagnosis and outcomes.
Additionally, since the study period covers only the calendar year 2019, the analysis reflects a time when clinical use of SGLT2 inhibitors was limited, which may affect the interpretation of treatment patterns and outcomes related to this therapy.






Comments (0)