
Remember me
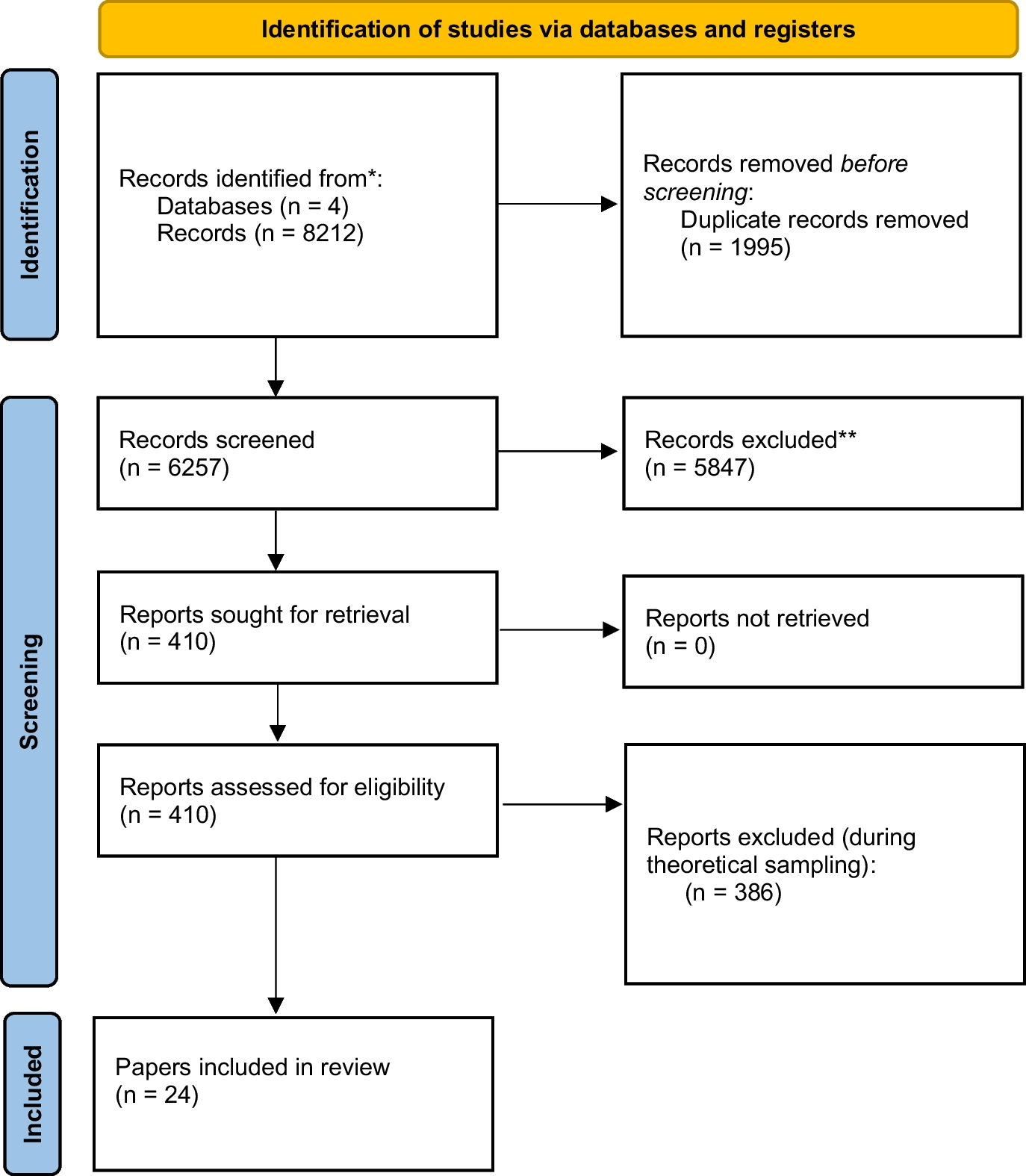
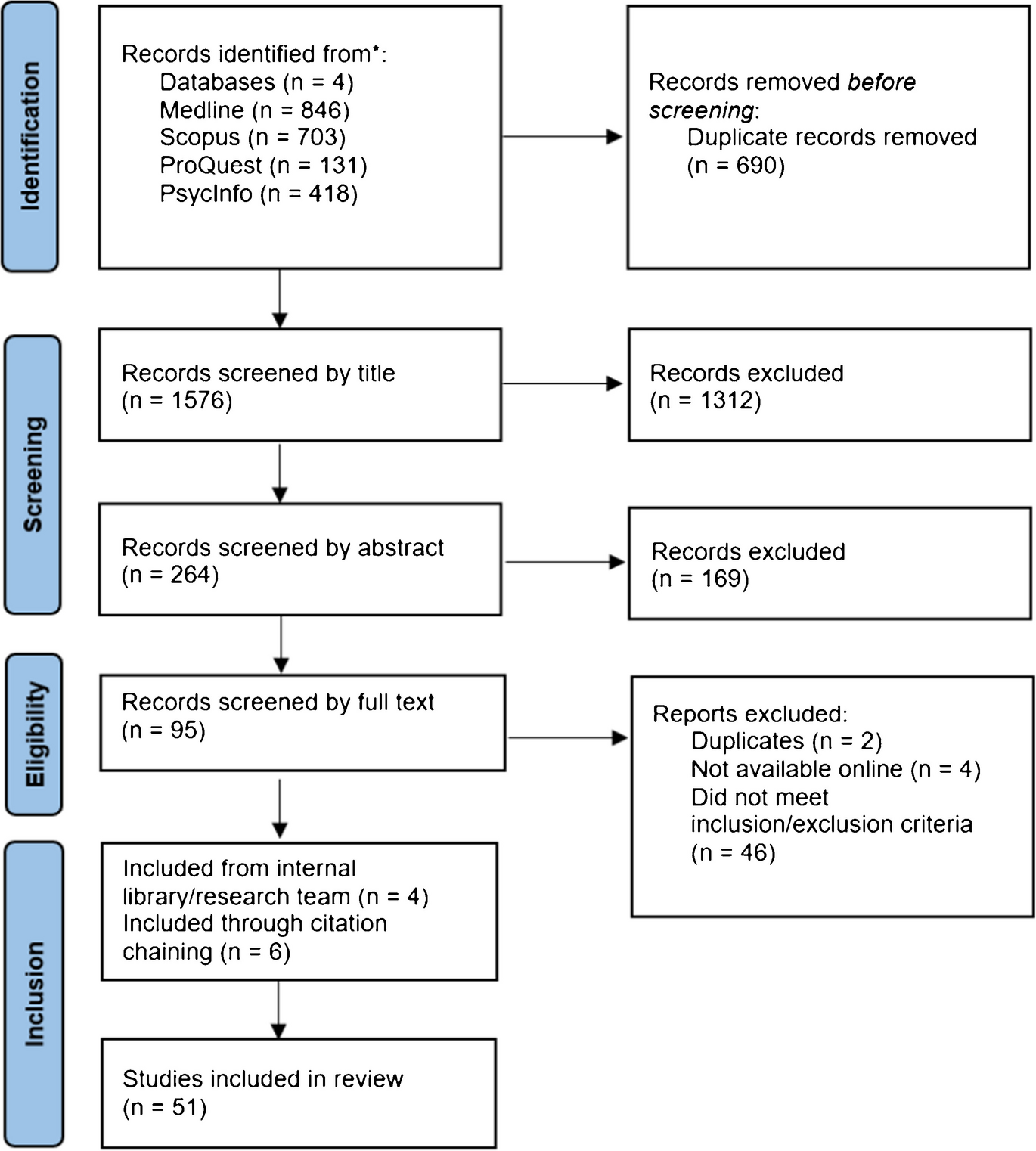



The search identified fifty-one articles discussing ethical issues or practice guidelines in psychedelic research and therapy (see Supplementary Material C). These have been assigned a numerical citation, which have been used throughout the results to refer to key examples of the ethical issues discussed.
All included articles were published in the last five years (see Figure 2). Most articles were led by authors from the United States (55.8 %; Figure 3), Canada (11.5 %), UK (9.6 %), and Australia (7.7 %). Additional articles were published by authors in Brazil, Switzerland, Spain (3.8%), and Hungary (1.9%).
Only nine articles employed empirical methods to understand the ethics of PAT, including five that engaged with stakeholders. Of these, one was led by Indigenous authors (13), one consulted Indigenous stakeholders (45), and two consulted individuals with lived experience—previous trial participants and PAT therapists (9, 14). Two articles also consulted research, industry, and community stakeholders (14, 45), and one article consulted experts in psychology, ethics, religious studies, palliative care, anthropology, and legal studies (40).
Thirteen articles included declarations that one or more of the authors were in paid advisory relationships or receiving other financial support from psychedelics industry/organisations (e.g., COMPASS, Silo Pharma). One author declared that they were a member of an ayahuasca religion (4).
Content AnalysisFive ethical themes were identified through the content analysis: 1) standards of practice (which included sub-themes of beneficence/non-maleficence, competence, informed consent, and therapist attributes), 2) equity, 3) integrity, 4) cultural appropriation, and 5) epistemic justice (see Table 2). There was diversity in the frequency and depth of each article’s discussion of the issues captured within the theme, and the recommendations made to deal with these ethical challenges.
Standards of Practice Non-Maleficence and BeneficenceThe principle of non-maleficence in this context refers to researchers and therapists’ obligation to abstain from causing harm to participants. Non-maleficence was identified in thirty-three articles, and was primarily discussed in terms of the physiological, emotional, and psychological side effects culminating during altered states (e.g., 11, 40, 50). Several articles suggested that potential adverse effects were not fully understood and potentially underreported and underestimated, such as increased heart rate, breathing rate, and psychological distress (e.g., 29, 40). Articles also highlighted the increased vulnerability participants experience during altered states. Vulnerability was described as stemming from the imbalanced power dynamic between practitioner and client, an enhanced sense of intimacy (e.g., 9), participants’ heightened emotional sensitivity and increased suggestibility whilst under the influence of psychedelics (e.g., 1, 47), and the fact that the participant cannot leave the premises during the acute psychedelic experience (e.g., 10).
Several articles suggested that PAT had a favourable risk-benefit ratio (e.g., 2, 44). However, authors generally highlighted the need for more research with priority populations such as Black, Indigenous and people of colour (BIPOC), LGBTQIA+ people, and people with disabilities in order to assess the safety of PAT in these populations (e.g., 6, 32, 38). One article suggested that risk-benefit analyses ignore the challenges individuals from priority populations may face in consenting to PAT, due to factors such as cognitive disabilities, marginalization, or vulnerability to coercion (34).
Beneficence in this context refers to researchers and therapists’ obligation to promote participants’ welfare. Beneficence was only discussed in a few articles, with a focus on the moral obligation to provide treatment to those in need (e.g., 49, 33). One article mentioned post-trial access (6), expressing concern that the legal status of psychedelic drugs constituted a barrier to participants being able to benefit from PAT post-trial.
Suggestions for upholding the principles of non-maleficence and beneficence in PAT research and practice included advising participants of safety guidelines prior to the session (e.g., 40), providing post-session integration care, and providing a safe and supportive “setting” (e.g., 6) (“setting” refers to the physical and social environment of sessions [Schenberg 2018]). One article suggested a public-private partnership, where stakeholders collaborate to create and promote best practice standards for harm reduction, risk mitigation, safety monitoring, and benefit maximization, as well as provide recourse for individuals harmed during PAT (4). Suggested stakeholders were government and non-governmental departments and organisations, representatives of Indigenous communities that traditionally use psychedelic substances, academic researchers, and sponsors of drug development (4).
CompetenceCompetence was discussed in twenty-one articles and highlighted the importance of practicing within one’s area of expertise or training (e.g., 2, 37, 40). Several articles expressed concern that there was no legal credentialing system for PAT practitioners (9, 45). Many articles indicated that cultural safety and/or humility are important competencies in PAT (e.g., 10, 14, 36, 45), including an understanding of racial trauma (42, 16). Strategies for supporting competent and culturally safe practice included having therapist teams who matched the ethnicity of the client (10), having two therapists (43), and creating a culturally safe setting (48, 26). One article also suggested incorporating shamanic practices, which may include healing songs, prayer, and the creation of a personal altar for the participant (36).
Informed ConsentInformed consent was discussed in sixteen articles and revolved around three main topics: 1) gaining informed consent prior to psychedelic sessions, 2) informing participants of the risks and ineffability of the psychedelic experience, and 3) safely engaging in therapeutic touch. Authors questioned whether truly informed consent for PAT could be gained prior to psychedelic sessions (e.g., 9, 40, 45). Reasons driving this doubt were that participants have unrealistic expectations due to media hype (e.g., 20, 43), participants may experience pressure to participate from enthusiastic researchers (22), and the ineffability of the psychedelic experience could not be adequately conveyed to participants prior to the session (e.g., 20, 32, 44). Authors additionally questioned whether informed consent could be gained from individuals with previous psychedelic experience who may underestimate harms (6), and participants with cognitive disabilities, substance addiction, or communication impairments (e.g., 6, 32, 34). The issues with surrogate consent were discussed in circumstances where the participant does not have capacity to consent, such as those with disorders of consciousness (34). One article mentioned the potential for “therapeutic misconception” in PAT research, where participants may not understand that the primary aim of a trial is to advance scientific knowledge and not to directly benefit the participant (6).
Articles suggested several ways of conveying the ineffability and possible harms of the psychedelic experience. These were audio-visual aids (6), sharing testimonials from previous persons who have undergone a psychedelic experience (6, 32), using accessible and agential language (6, 30), and being clear about the evidence base for PAT (43). Authors also suggested making it clear prior to the session that participants could not leave part way through a psychedelic session for safety reasons (6, 43). One article suggested that fully informing participants of an ineffable experience was unrealistic and that simply informing them that it was “epistemically inaccessible” was adequate (20). Several articles expressed the need for standardized informed consent protocols (e.g., 23, 43).
Therapeutic touch, which is often employed during PAT, involves a practitioner providing comforting touch such as hand holding during the psychedelic session and raises additional challenges for informed consent (Smith and Appelbaum 2021). Concern was expressed over whether informed consent for therapeutic touch could be gained during altered states (e.g., 9, 40, 45). One author described how participants may consent to one option then change their mind during therapy and how assessing whether a client had decision-making capacity during an altered state may be counter-therapeutic (44). Suggestions included a two-stage process for therapeutic touch where consent (or lack thereof) was determined before the session and then re-ascertained during the session (9), only providing therapeutic touch when it is requested (44) and thoroughly documenting consent (11).
Therapist AttributesTwenty-four articles discussed the values, morals, and competencies that PAT practitioners should possess. The importance of respect was discussed in terms of not discriminating against clients based on gender, religious beliefs, or other personal factors (e.g. 34, 36, 40). One article suggested that practitioners should cultivate spiritual intelligence (31) in order to increase empathy with participants who may have spiritual experiences during sessions. Another article suggested that therapists should not impose any spiritual beliefs on clients (21). Many articles highlighted the need to be empathetic, compassionate, and supportive as well as capable of building a therapeutic alliance and a trusting relationship with clients (e.g., 30, 31, 36).
The importance of self-awareness when practicing with vulnerable participants during altered states was highlighted and included being aware of increased transference and countertransference in the session (e.g., 8, 36, 40). Trust was suggested to be particularly important for BIPOC and other priority populations, including people who identify as LGBTQIA+ or with disabilities (e.g., 16, 27). The importance of supervision and self-care was commonly discussed (e.g., 2, 8, 9, 40). Self-care included practices such as being aware of one's intentions and needs entering a session and undergoing therapy to minimize the possibility of transference and boundary transgressions. Articles emphasized the importance of supervision in improving professional judgement and accountability.
Many articles discussed therapist use of psychedelics. Authors suggested that therapists should have experience using psychedelics because it enhanced client trust (9) and increased therapist understanding of the clients’ experience (31, 40). One article (36) suggested that if psychedelics were not available legally, therapists should try other methods such as holotropic breathwork. In contrast, another article discussed the possibility that psychedelic use may not be a necessary aspect for training practitioners and that it may affect clinical judgement and objectivity (22).
Boundary transgressions were discussed in fifteen articles. Unclear boundaries between the therapist and client during the psychedelic session were frequently discussed as a possible source of harm that could lead to exploitation of clients or the formation of dual relationships (e.g., 40, 45, 51). While boundary transgressions were usually seen as occurring due to increased vulnerability and intimacy between the client and practitioner (e.g., 1, 9, 11), one article suggested that in situations where participants presented a risk of harm to themselves or others, physical interventions may be necessary (40). Suggestions for maintaining professional boundaries included being self-aware of the risk of transgressions occurring, setting clear expectations prior to the session (8, 9), documenting consent, reporting transgressions, and upholding accountability (4, 36). It was suggested that the risk of dual relationships developing should be mediated by paying attention to confidentiality, trust, communication, and boundary setting (40). One article suggested that “energetic” boundary setting (9), which involved being conscious of nonphysical and nonverbal communication, was something practitioners should be aware of.
EquityEquity in this context refers to the fair and just treatment of all patients and research participants. Equity was discussed in thirty-five articles and was described in terms of 1) inclusivity in research (e.g., 14, 26, 48) and 2) equal access to PAT (e.g., 4, 10, 45).
Inclusivity in research was widely discussed (n = 21). Most articles described a need for greater inclusion of BIPOC (e.g., 14, 26, 28), with several articles also discussing the inclusion of LGBTQIA+ and disabled persons (e.g., 10, 16, 32). Authors also noted the importance of excluding certain individuals for safety reasons. Excluding high-risk individuals, such as those with a personal or family history of psychosis, was understood as a protective measure against possible adverse effects of PAT (32, 50). On the other hand, excluding these groups was seen as a barrier to access which would prevent them from benefiting from PAT (e.g., 1, 30, 50). In particular, excluding disabled individuals was seen as a potentially paternalistic view (32)
Access to PAT was widely discussed (n = 18). Articles described an “inverse-care law” in psychedelic research and practice, where those who need treatment the most may be least likely to be able to access that treatment (48). Financial burden on participants was a commonly discussed barrier to access (e.g., 30, 48, 50). Articles suggested that due to the high cost of treatment, as well as practical considerations such as transit costs and time taken off work, PAT may be unaffordable for many (e.g., 17, 38, 48). One article expressed concern that negative connotations around psychedelic drug use may create a barrier to access (5). For BIPOC specifically, barriers included social stigma and stereotypes around illicit drug use (16) and mistrust in the medical system due to previous exploitation and harm (45).
Lack of access and diversity in research is closely linked to concerns around fair distribution of benefits. Many articles expressed the need for research to directly benefit traditional-knowledge holders as well as ethnic minorities (e.g., 16, 28, 45). However, what “benefit” required was rarely discussed, with one notable exception (13). Celidwen et al (2023) suggested sharing benefits derived from the use of Indigenous medicines and practices with source communities as they deem appropriate.
Authors expressed concern that a lack of access may motivate individuals toward underground use (37). Suggestions for improving access included reducing the number and length of sessions, scheduling sessions outside of business hours, conducting assessment via telehealth, and compensating participants for their time and transit costs (30). One article suggested that the use of non-hallucinogenic psychedelics—i.e., altered psychedelic compounds with reduced hallucinogenic potential (Dunlap et al. 2020)—may increase accessibility because they can be administered at home over telehealth (38). Policy suggestions included the use of programmes such as coordinated registry networks and prescription drug monitoring systems to promote expanded access and to determine need (4). Authors also discussed destigmatizing PAT for all participants, but particularly for BIPOC who may view PAT as unsafe or stigmatizing (16, 42). Consideration of cultural variation in symptom presentation and targeted advertising and referrals from outpatient providers were suggested ways to increase BIPOC recruitment in research (16).
Many suggestions for improving access and inclusion highlighted the need for collaboration and increased diversity in research teams (e.g., 27, 39, 40). Articles discussed the need for collaboration with BIPOC and disabled communities (e.g., 26, 30, 36). Increased diversity in research teams was suggested to better understand the barriers to minority access, improve practitioner-client pairings, and reduce harm during sessions (26).
IntegrityIntegrity was discussed in thirty-one articles and revolved around two main topics: 1) conflicts of interest and 2) psychedelic exceptionalism and hype. Many authors expressed concern about financial conflicts of interest in psychedelic research (e.g., 17, 37, 40). Articles suggested that vested interests would not prioritize participant wellbeing, safety, and equitable access, would “crowd out” marginalized voices (36), cause distress, and undermine Indigenous participation (17). Vested interests could also overlook socio-political factors that lead to mental illness (37) and engender questionable research practices (35, 37). One author questioned whether it is the job of researchers to call out bad practice and what they should do if they find results that don’t align with desires of financial stakeholders (35). They highlighted the prevalence of vested interests, describing the common occurrence of receiving anonymous offers for money and illegally acquired or synthetic psychedelics (35) to “speed research along.”
A second and related concern was “psychedelic exceptionalism” (21), which was described as contributing to “blind devotion” to the research (11). Psychedelic exceptionalism is the belief that psychedelic drugs are uniquely transformative or beneficial, and as such should be exempt from the ethical, clinical, and legal requirements that other drugs are subject to (Johnson 2021). Authors expressed concern that exceptionalism was leading to questionable research practices, abuses of power, researchers not being transparent about the risks of psychedelics, and findings being overstated and embellished in the media (e.g., 11, 18, 37). One article discussed whether researchers having previous experience using psychedelics may impact objectivity and good science practices. It suggested that having researchers in the team who haven’t had personal experience with psychedelics may alleviate this risk (22).
Many suggestions for integrity in research recommended adherence to the principles of open science (UNESCO 2022). These included open data, pre-registration, peer-review, study replication, transparency, and providing a clear description of the generalizability of the study in research papers (e.g., 18, 21, 35). Authors also discussed the need to mediate public expectations by using transparent and objective public education and press releases (4, 37) and stated that psychedelic advocacy organizations should maintain high evidence-based standards and eschew media hype (32). Many articles suggested the need for ethical oversight, policy safeguards, supervision, and legal accountability for practitioners (e.g., 2, 4, 43).
Cultural Appropriation and SafetyCultural appropriation, which involves the extraction of Indigenous plants (25) and knowledge (19), was discussed in twenty-three articles. Concern was expressed about how the commercialization and appropriation of psychedelics would harm Indigenous people (e.g., 13, 15, 24). Authors also discussed the epistemic harms linked to appropriation (e.g., 24, 25); this theme will be expanded on in the next section.
Authors expressed concern over the patenting of psychedelic drugs and intellectual property regimes that extract Indigenous knowledge (e.g., 13, 17, 41). Appropriated knowledge has informed trial design, and this has often been done without any meaningful consultation, consent, or permission from Indigenous peoples (17, 19). Further, Indigenous people have not received adequate compensation or benefit from the use of their knowledge (10, 29). Appropriation may cause intergenerational distress that perpetuates mental health issues (17) and causes spiritual practices to lose their meaning (15). One article described concern that shamans would be forced to align with new safety regulations (24). Other authors expressed concern that the deforestation of rainforests was occurring due to the extraction of natural plant medicines (13). This practice may leave Indigenous users without access to traditional medicines (7, 25).
Many articles identified the need to “recognize” (7, 19) and “acknowledge” (13, 26, 28) the Indigenous origin of psychedelic practice and for “reciprocity” (15, 36) and “respect” (7, 15), without providing specific recommendations for how this should be done. One article (13) did provide ethical principles and guidelines for Western psychedelic practice, namely “Reverence, Respect, Responsibility, Relevance, Regulation, Reparation, Restoration, and Reconciliation.” These principles were developed through Indigenous-led collaboration with stakeholders. Suggestions included acknowledgement of Indigenous traditions; protecting Indigenous intellectual property; free, prior, and informed consent in research; increased accountability for harmful practices; restoring Indigenous authority; safeguarding self-determination; active inclusion of Indigenous knowledge holders and practitioners; formal efforts to include Indigenous-led intellectual foundations in Western practice; benefit sharing; and reparation (13). Other suggestions in the literature included incorporating Indigenous methods (7), investing in Indigenous-led research (7), increasing collaboration in research and practice (48), sustainable harvesting of psychedelic plants (25), and practicing restorative justice (43).
Epistemic JusticeEpistemic injustice is a form of harm that can include the silencing, distortion, or mistrust of certain ways of knowing (Fricker 2007). This theme was identified in fifteen articles. Authors expressed concern that psychedelics were becoming primarily framed by Western biomedical approaches to epistemology. Most discussion around epistemology was concerned with Western epistemologies delegitimizing Indigenous knowledge and practices. Some have argued that Western epistemologies tend to be reductionist and objective, whereas many Indigenous epistemologies tend to be subjective and holistic (Antoine et al. 2018; Mazzocchi 2006). Discussions around the delegitimization of Indigenous knowledge and practices included lack of compensation for Indigenous knowledge holders, the displacement and loss of Indigenous knowledge (25), and the othering of Indigenous people (16). Authors discussed related epistemic concerns such as bioreduction (39, 41). Bioreduction in this context refers to the perception of a concept only in terms of its biochemical components, at the expense of subjective knowledge (Yaden et al. 2022). Articles suggested that bioreduction, which discounts subjective Indigenous knowledge and practices, may reduce the effectiveness of PAT and hinder understanding of its therapeutic properties (41) and that Indigenous traditional psychedelic users have “epistemic expertise” that should be respected (39).
Not all discussion of epistemic justice was specific to Indigenous people. Injustice was described where psychedelic-using communities’ views were discounted and seen as untrustworthy (41, 50). One article suggested that psychedelic-using communities, including for example artists, healers, and festival-goers, had “epistemic expertise” and thus should be consulted in research (39). Discussions around medicalization suggested that globalized Western psychiatric concepts displace diverse expressions of distress (24) and ignore systematic and social issues (37). Another epistemological concern was that PAT may cause “epistemological harm” because it had the potential to alter participants’ perception, cognition, and beliefs (23).
Suggestions for epistemic justice largely involved the adoption and acceptance of Indigenous psychedelic knowledge and practices. Articles suggested giving equal privilege to Indigenous and Western knowledge (24), learning from Indigenous knowledge holders, and privileging Indigenous ethics, practitioner responsibility, training procedures, and land repatriation (15, 24). One author suggested that the limitations of Western scientific knowledge should be acknowledged and that Indigenous approaches to epistemology could combine with Western knowledge to enhance research (15). Another author suggested that a system of mental health care should be developed that considers different epistemologies (7). Articles noted that spirituality was a knowledge system often closely linked to Indigenous psychedelic practice (24, 31). Several articles suggested that spirituality should be accepted as an aspect of PAT and that practitioners should have spiritual experiences as part of training (24, 31, 49). Regarding psychedelic-using communities, one article suggested the need to legitimize lived experience knowledge (39).
ConsultationDiscussion in the consultation workshop expanded upon previously identified ethical issues around informed consent, integrity, and reporting standards, access, and competence. Participants agreed that the ethical issues identified in the literature were consistent with their own experiences. They further highlighted the importance of several issues that they found pertinent. These included issues with informed consent during altered states, lack of open science in psychedelic research, and belief changes during PAT. Workshop participants also raised several issues not frequently discussed within the literature. These were 1) lack of post-trial care, 2) lack of consensus on models of care and competencies, and 3) how current research and its associated ethical issues will be translated into practice (see Table 3).
Table 3 Additional Themes Identified through Consultation
Comments (0)