
Remember me



Our data from institutional representatives represent a subset of data obtained from a larger set of regulator interviews across two periods—May to September 2022 for Western Australian regulators and September 2022 to July 2023 for Victorian regulators (White, Haining, and Willmott 2025). Overall, we conducted forty-seven regulator interviews with fifty-five individuals via Zoom or telephone, with one to three participants per interview. For this article, we draw on the data relating to local regulatory approaches of fifteen institutions (some with multiple sites) based on data from eighteen interviews with seventeen participants (see table 1). One participant took part in two interviews due to their involvement with two local responses. Interviews with institutional representatives ranged between 57 and 152 minutes. Each institution had representation from at least one participant who was intimately familiar with the institution’s approach to VAD, including having insight into its development, implementation, and/or operation. Each institutional case has been de-identified to protect the confidentiality of the participants and the institutions they work for.Footnote 5 However, to assist with result interpretation, some general characteristics have been provided in table 2. For the purposes of classification, we categorize institutions as having an IO if they elect not to offer the full suite of VAD activities to the extent to which their capability permits. We do not consider limiting VAD to particular individuals (e.g., own patients or catchment) to constitute an IO.
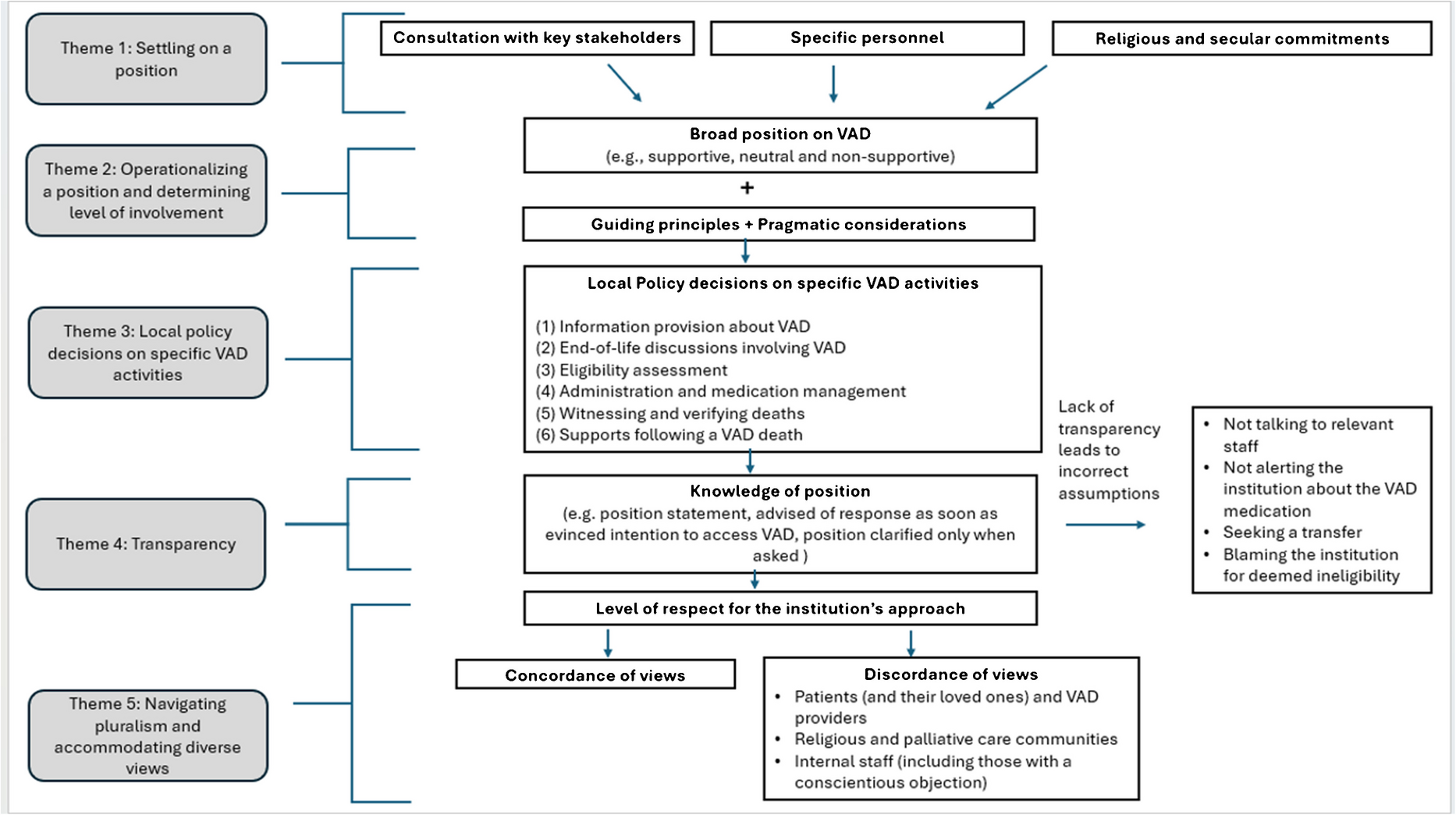
Table 1 Participant demographicsTable 2 Characteristics of institutionsAs a result of data analysis, we generated five main themes—settling on a position; operationalizing a position and determining level of involvement; local policy decisions on specific VAD activities; transparency; and navigating pluralism and accommodating diverse views—that will now be examined. The thematic schema in Fig. 1 shows the relationships between these themes.
Fig. 1 Settling on a Position
Settling on a PositionMost participants reported that considerable preparatory work informed the institution’s position on VAD, which determined whether it supported VAD in principle. Most institutions were proactive in formulating their position when VAD laws were being considered or during the implementation period after the law passed, reporting that their position derived from extensive consultation with key stakeholders (e.g., executive, church representatives, peak bodies, staff, and consumers). Some institutions used the consultation to develop (or interpret) broader frameworks (e.g., theological frameworks) that were then translated into a position on VAD. In one institution, consultation was not deemed necessary to determine the organization’s position on VAD.
Interviewer: Board engagement or not on that issue?
Respondent: No … [the decision to offer VAD] would be seen here as operational. [#9] [Non-IO, Private]
Views of certain personnel within the institution were sometimes thought to influence the institution’s position and/or approach to implementation.
What I didn’t appreciate necessarily is how much an individual leader’s views can translate into an [institution’s] processes … if leadership are agnostic or even ambivalent about the legislation, there is more likelihood that one gets a good enough balance between respecting patient[s’] decisions and autonomy, whilst ensuring a positive and safe institutional culture around a controversial issue. [#7] [Non-IO, Public]
Each institution acknowledged the lawfulness of VAD and the need to respect a person’s choices. However, some institutions that did not support VAD limited their participation. Opposition to VAD was stated to be on religious and secular grounds (e.g., inconsistent with palliative care philosophies).
We don’t want to participate in VAD because of the long-held [religious] position and ethic that prefers to journey with a person to the end of life rather than to hasten the death of a person. We would prefer quality palliative care. [#16] [IO, Private]
Conversely, institutions that supported VAD often framed their support in terms of an overarching commitment to respecting patients’ choices. For some institutions, this stemmed from their long-standing involvement in palliative care.
Where [Institution X’s] position has come from [is], particularly from the palliative care team … which is around supporting choice and control … [T]his is this client’s illness, this is their trajectory, this is their journey however you wish to describe. And we work with that person in the best way that they would like to be worked with and with the choices that they would like to be able to make. [#5] [Non-IO, Private]
Operationalizing a Position and Determining Level of InvolvementIn addition to an institution having a broad position on VAD (i.e., supportiveness or not of VAD), institutions needed to operationalize this and make decisions about the extent of their level of support for patients wishing to access VAD. Such an approach appeared to be informed by guiding principles and pragmatic considerations.
As was the case in relation to forming a broad position on VAD and determining whether the institution supported VAD in principle, participants identified several guiding principles that informed their degree of participation in the VAD process. Such principles have been broadly categorized in table 3; however, how these principles were framed varied across institutions. In cases of objecting institutions, values extended to palliative care and religious commitments that needed to be accounted for and balanced with the need to respect a person’s autonomy and the need to avoid obstruction. Different approaches were taken by objecting institutions to reconcile this, including by framing VAD as a “life choice” (and therefore something to respect) and/or ascertaining the level of complicity the institution was comfortable with.
Table 3 Guiding principles informing local policy decisionsPragmatic considerations, including the nature and size of the service, the institutional type (e.g., health service or aged care setting), the nature and capacity of the institution’s staff, reputational risk, and cost, also informed the nature of an institution’s approach (see table 4). Such considerations also influenced the limitations (if any) that the institution put on its delivery of VAD services. Such limitations included whether institutions would limit provision to business hours, limit access to individuals within the institution’s region, limit access to individuals who had an affiliation with the institution or its staff, or would only allow external personnel to participate in VAD provision (as opposed to its own staff).
Table 4 Pragmatic Considerations Influencing Degree of ParticipationLocal Policy Decisions on Specific VAD ActivitiesIn addition to decisions about the broad level of involvement (e.g. provision of VAD for all patients or only the institution’s patients), institutions also needed to make policy decisions about different aspects of the VAD process (see Supplementary Material 1), which were similarly informed by the institution’s position and the aforementioned guiding principles and pragmatic considerations.
1. Information Provision about VADWhile only a subset of institutions provided general information about VAD (or made it readily available), all institutions were prepared to provide at least some information about VAD upon request, albeit to varying extents. For many of these institutions, this included (and was sometimes limited to) details of the statewide care navigator service (typically in the form of a handout), which could be contacted for further information. Some institutions would facilitate contact with the care navigators on behalf of the person in all (or particular) circumstances. In most institutions (including some objecting institutions), the care navigators were permitted on-site and treated like private visitors. For institutions with a dedicated VAD liaison (i.e., an individual who was the point of contact for VAD in the organization), information about VAD was provided via that liaison (rather than the care navigators, albeit not exclusively). Sometimes, the VAD liaison was a designated VAD coordinator; in other cases, it was an organization’s manager or a designated clinical lead (e.g., a palliative care physician).
2. End-of-Life Discussions Involving VADMany institutions acknowledged the inevitability of people raising VAD with their staff and the need for internal processes to support such conversations. Staff were made aware of legal restrictions with respect to raising VAD.Footnote 6 Many participants observed that when a person raised VAD, it was a good opportunity to discuss the person’s values and preferences more broadly and explore their desire to hasten death. Such conversations were not unusual for many institutions’ staff, who were often considered well-placed to engage in such discussions.
For objecting institutions, while staff were generally permitted to have such conversations with patients, local policies typically required staff to be clear about the limits of their involvement in VAD. In doing so, many participants emphasized the need to respect a person’s choices and reinforced that they would not abandon someone seeking VAD. In some institutions (whether or not they had an IO), an escalation approach existed whereby people requesting VAD would be connected with dedicated VAD liaisons. Other institutions referred patients to the care navigators.
3. Eligibility AssessmentsInstitutions’ approaches to eligibility assessments varied. Institutions supporting VAD would assist patients in accessing VAD providers—for example, by facilitating contact with willing providers within the institution (or visiting specialists). Where the institution did not have medical staff (or VAD providers), care navigators would assist the patient in accessing a VAD provider, or patients would access willing providers on their own accord (e.g., via their general practitioner).
For objecting institutions, staff were not permitted to conduct VAD eligibility assessments in the course of their employment with the institution, even if qualified to do so. However, in such institutions, staff could provide clinical and prognostication information to other practitioners (including VAD providers) to help inform the VAD eligibility assessment. In the objecting aged care settings examined, institutions would permit external assessors on site to make assessments, but this was not allowed in other objecting settings.
4. Administration and Medication ManagementInstitutions varied regarding how much they would permit self or practitioner administration on their premises.
(a)Self-administration
In all but one of the institutions examined that had sites (i.e., not community nursing), the VAD medication could be brought on-site, and self-administration could occur on the premises. Most institutions also indicated that the statewide pharmacy service would be permitted to dispense the VAD medication on-site. Such permission was justified on the basis that the VAD medication was ultimately the person’s property and, therefore, should not be unnecessarily interfered with. Many institutions had strict protocols in place in relation to the VAD medication and, in some cases, the ability of their staff to handle the substance, which was prohibited in some institutions.
When self-administration took place in a health service or inside a palliative care unit, many participants observed that restrictions and controls were in place. These were often justified on safety grounds. Some participants reported that their institution encouraged patients to take the medication at home (where possible), with some institutions having processes in place to assist with discharge into the community, including offering to put the person in contact with community nursing services.
However, participants conceded that discharge was not always possible (or desirable), and consequently, the person would be permitted to take the medication on-site. Institutions varied with respect to their VAD medication storage requirements. Some institutions allowed patients to have their medication in a locked drawer close to their bed, whereas others required the medication to be locked elsewhere. Moreover, some institutions required patients to sign documentation and advise precisely when they would take the medication. In some cases, administration had to occur during set times or in the presence of specific staff members (who, in some institutions, were permitted to prepare the VAD substance). In other settings, stringency around time and personnel present did not exist. However, institutions encouraged people to notify them about their anticipated time of death so that they could assist with administrative and/or clinical arrangements.
(b)Practitioner-administration
Practitioner administration was not permitted at every institution. In all participating aged care facilities, practitioner administration was allowed on-site. This practice was also permitted at non-objecting health services and a stand-alone palliative care unit. Institutions that did not have VAD providers on staff (or did not have enough) needed to credential visiting doctors to facilitate administration, which was one reason (albeit not always exclusively) why practitioner administration was limited at certain institutions. In health services with VAD providers, practitioner administration was generally restricted to those staff members to the extent capacity permitted. At one institution, it was possible to credential a patient’s general practitioner to administer VAD to a patient if there was a long-standing relationship, despite having a pool of VAD providers available.
(c)Presence during administration
Some institutions required specific staff to be present during administration as a form of support. Participants also acknowledged that individuals may request that certain health professionals and/or carers be present during administration, and institutions varied in the extent to which this was permitted. In some cases, presence during administration was left to the discretion of individual staff members. In other cases, the institution would allow its staff to be present on a case-by-case basis.
5. Witnessing and Verifying DeathsInstitutions varied regarding the extent to which they would permit staff to witness and verify VAD deaths. Witnessing is required at multiple stages of the VAD process, including at the final request stage and/or during practitioner administration. In some institutions, staff were not permitted to witness. In other institutions, staff were allowed to witness and/or facilitate contact with an advocacy service that could provide volunteer witnesses. Some institutions also indicated they would verify deaths; however, it was unclear whether all institutions permitted this.
6. Supports Following a VAD DeathSupport for families following a VAD death was generally available from institutions regardless of whether they supported VAD. In some institutions, this would be the extension of bereavement support offered following any death. In other institutions, dedicated VAD bereavement procedures were in place. Support was also made available to staff following a VAD death, regardless of whether the staff were directly involved. One participant described a situation where pastoral care was extended to a VAD provider who visited the institution for administration.
TransparencyInstitutions varied regarding the extent to which details of their local response on VAD were publicly available. However, no institution had its local policies (where they existed) or detailed information about the extent to which they supported VAD (i.e., activities they took part in or permitted) readily available to the public. Some institutions published VAD position statements (or equivalent), although this was not uniform. Published position statements were often very high-level, articulating, in general terms, the institution’s supportiveness (or not) of VAD. Some participants attributed the failure to publish a position statement to oversight. However, in one institution, there was a deliberate decision not to do so to avoid drawing attention to VAD.
Interviewer: … [So, your approach is] not necessarily to advertise the fact that you won’t be providing VAD … [but] just clarify [your scope of participation] when [asked], rather than to signpost it.
Respondent: Yes, absolutely. [#15] [IO, Private]
Regardless of the approach, participants reported that if asked about the institution’s position, they would detail the extent of their participation to permit people to make informed decisions about attending (or remaining in) the institution. In some institutions, as soon as the patient evinced an intention to access VAD, they would be advised of the institution’s response.
[We provide] clarity for the customer on [Institution X’s] approach. So, they may have read the [position statement], but that’s words on a page, and they can interpret that how they choose to do so … the approach is that [the leader at the site] meets with the customer and/or their family if that’s what they want, and we have [a] clarifying conversation. [#12] [IO, Private]
The lack of transparency by institutions in some cases led to individuals seeking VAD and/or their loved ones making incorrect assumptions about the institution’s approach. In the case of objecting institutions, the starting assumption was often that the institution would attempt to obstruct access if it did not support VAD in principle. This manifested in several behaviours including not talking to relevant staff members out of fear they would coerce them out of VAD, not alerting the institution that the VAD medication was in their possession, requesting transfers to other facilities because of fear they would be blocked, and/or a person’s loved ones blaming the institution for their loved one’s ineligibility (table 5).
Table 5 Behaviours driven by assumptions about institutions’ positionsNavigating Pluralism and Accommodating Diverse ViewsSome participants indicated that just as institutions should respect a person’s right to VAD, the values of an institution, its position and its approach to VAD should be respected by others. However, it was reported that this was not always the case. One participant described a situation where a VAD provider made comments that devalued the institution’s position, even though the institution permitted VAD to take place.
[There was a case where there was an] inability to understand [our] position … [with the] doctor coming in and saying something like, “You’ve given this person the great gift of dying.” And we go, “No, that’s not what we would have wanted, if we had the choice, we would have preferred palliative care to the end.” But it was—you need to celebrate with champagne … that just left a rotten taste on the part of the staff... I can accept that a doctor needs to do his or her thing, but can we just have … a more sensitive approach to this? … [I]t might just be individuals involved … another doctor coming along might handle that differently. [#16] [IO, Private]
Some participants noted that some hostility (e.g., from patients, their loved ones, and VAD providers) was averted by working closely with the care navigators, who were aware of the institution’s limits and helped minimize any disruption to the person’s care.
We’re very clear to the navigators where our lines in the sand are. [#8] [IO, Public]
However, working relationships with care navigators were not uniformly reported. The absence of such a relationship was considered disadvantageous.
In my conversations with my counterparts and other service providers, we understand that some of them have … a working relationship with the navigators. That means that if someone has requested a doctor to come in, the navigators will liaise with the facility. We haven’t got that in place at the moment. I have requested it … at least it would give us the heads up. [#16] [IO, Private]
In a different vein, some participants representing institutions with an IO indicated that the way in which their institution was still able to support VAD (even if not involved in direct provision) was not uniformly accepted. On the one hand, participants reported that some people found it difficult to reconcile with the permissibility of the institution’s position. This was particularly the case among the broader religious community.
I brought two new chaplains in at one stage, and we were having another VAD discussion and the look on their faces it was like, “Oh yeah, you guys haven’t been through this journey, let me take you through it quickly.” [#13] [IO, Private]
Despite potential backlash, however, participants noted that the ability of institutions with an IO to still support patients seeking VAD (to some extent) was preferable to some more restrictive approaches taken by some other institutions with an IO, which participants described as obstructive and impractical.
It’s very enculturated at [Institution X] that you hold the patient at the centre. And that’s different to some of the other [institutions] who’ve struggled a bit and got themselves into a bit of argy-bargy. [#8] [IO, Public]
Diversity of views was also evident among staff members of the institution. Indeed, participants indicated that, notwithstanding the extent of involvement of their institution in VAD, some staff may not fully accept the institution’s position (due to its permissiveness or restrictiveness). In cases where an institution did not support VAD, some participants reported that their staff could still participate in VAD outside of their employment with that institution.
[Staff] may work in another private hospital, or they might work in another public hospital, then there’s a freedom to choose within that whether they participate or not. But … when they work under [Institution X’s] flag … that’s where the non-assessment, etcetera [applies]. [#8] [IO, Public]
Participants also noted that staff were permitted to seek employment elsewhere (and, in some cases, may be managed so they do so).
We’ve had one or two staff at each of the sites where we’ve had [someone] go through the process who have a strong faith themselves and found it particularly confronting … Broadly speaking, we don’t have extremes within our organization. I think people would likely have either been managed out of the organization in a wider context or would’ve self-selected that, “This probably isn’t a place I want to work,” if they’re of that particular mindset. [#12] [IO, Private]
In some cases, staff working in an institution that provided VAD would claim a conscientious objection. All institutions supported conscientious objectors and aimed to support them by various means, including adjusting rosters, providing debriefing opportunities, and making support services known and available either within the institution or externally.
We do have [staff] that have registered concerns … once they understand that there are some legal things that we’ve got to respect, and then our position and how we’ve tried to navigate that, that’s been a little better to deal with … there’s also the conscientious objection clause within the legislation, which we’ve made clear to the people in the training, and we’ve told them how that can be accessed. And that does not impact their job or their position … or anything like that. [#16] [IO, Public]
In most cases (but not exclusively), individual conscientious objectors were perceived not to frustrate the process and were viewed as sympathetic.
I’d like to change the word “conscientious objector” in the next legislation because I think it’s quite a negative word. When I say people are conscientious objectors, I’m cringing inside because they’re still sympathetic to the whole process. [#1] [Non- IO, Public]
While most participants did not report issues with conscientious objectors, multiple participants noted tensions arose when some sites and/or units did not adopt the institution-wide response. Some of these tensions resolved over time, while others did not.
[There were] implementation issues with a couple of sites that actually said, “Yeah, great system, wonderful thing, but we won’t be doing it here.” [#6] [Non-IO, Private]
One participant spoke of a particular unit within an otherwise non-objecting institution that refused to offer (and sometimes discouraged) VAD. In some cases, attempts were made to orchestrate transfers out of the unit when VAD was sought, which was considered distressing. Reflecting on a particular experience, the participant recalled:
[The objecting unit was proposing to move the] patient … [but they] did not have a permit [to access VAD]. [It was] felt that the permit would come through the next day. [The patient] felt [they were] being moved because [they] had to die. So [they were] extremely distressed by that. [The VAD coordinator] got a call from [the patient’s loved ones] [and then] rang the ward to say, “Why are you moving [X]? [They do not] even have a permit.” And the nurse in charge said, “Well, I’ve been told by [one of the] physician[s] that [X] has to move” … that was just so upsetting. [#18] [Non-IO, Public]
In other institutions, VAD was generally available on all wards/campuses (to the extent there were available doctors). Transfers only occurred due to ward capacity concerns and/or if patients wanted to move to a nicer ward.
In [Institution X] itself, you can access it wherever you are. [#1] [Non-IO, Public]
Comments (0)