
Remember me



Rehabilitation medicine is a sub-specialty specifically focused on the consequences of medical conditions in terms of daily living. It aims at minimizing disability and optimizing functioning according to a biopsychosocial paradigm. From a theoretical point of view, and in accordance with modern medicine in general, it utilizes the ICD (International Classification of Diseases) for diagnosing the etiology of a condition, and the ICF (International Classification of Functioning, Disability and Health) for classification of the consequences of a condition. ICF is of primary importance in Rehabilitation medicine as well as in other medical branches dealing with rehabilitative efforts and is currently considered the taxonomy most pertinent for both classification and for clinical practice.
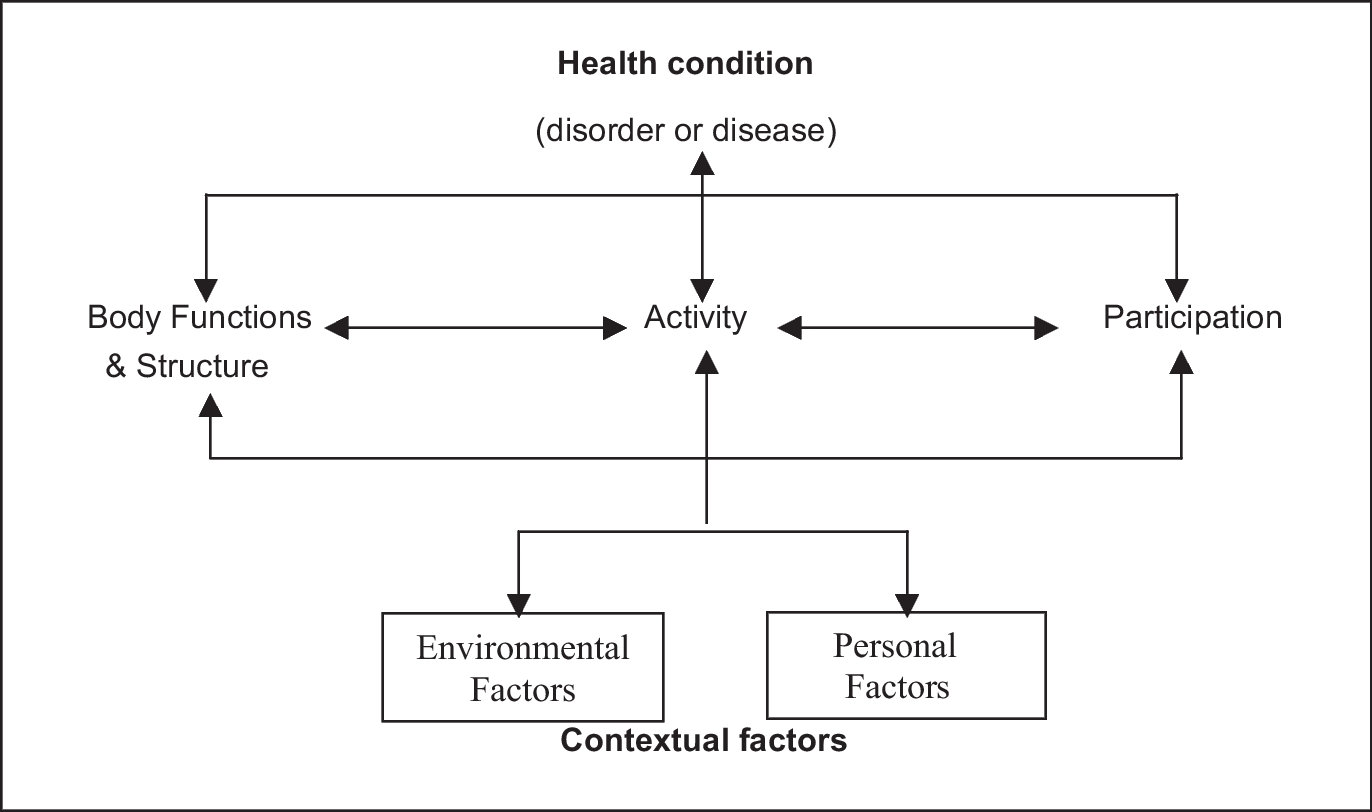
International Classification of Functioning comprises a classification of health and health-related domains. It is the WHO framework for measuring health and disability at both individual and population levels. International Classification of Functioning is well-developed for broadly assessing “functioning”, which according to its taxonomy is separated into “body structures and body functions,” “activities” and “participation.” In addition, it promotes (but does not explicitly structure) assessment of environmental as well as personal factors (Fig. 1) (WHO 2002).
Fig. 1
The ICF does not specifically include measures of well-being. However, both in clinical practice and in medical research, it is nowadays acknowledged as a matter of course that assessment of overall well-being also is required, typically in the guise of “quality of life” and/or “life satisfaction.” Therefore, ICF is sometimes complemented by instruments designed to specifically assess these issues, e.g. by the WHO-5 Well- Being Index or, more commonly, EQ-5D, the latter of which assesses health-related quality of life in terms of five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression.
However, the very concept of well-being is rarely discussed from a theoretical point of view in the medical context. In contrast, the assumption seems to be that attainment of maximal “functioning” (as measured by ICF) will also lead to the attainment of the maximally achievable well-being in light of the extant disorder or disability.
It may thus broadly be stated that rehabilitative medicine focuses on the direct pathophysiological consequences of a disease or injury as they translate into impairments of functioning. It tends to accept as well-being what EQ-5D or similar indices tacitly or explicitly comprise. However, in order to ensure that such instruments really measure what is taken to be important, it seems fundamental to first scrutinize how the concept of well-being is best understood. This seems to be a question for the philosophy of well-being. However, it seems unlikely that a person’s well-being is constituted in splendid isolation from contextual factors, e.g. cultural norms, socio-economic factors, etcetera. Thus, the situatedness of the individual in such terms also needs to be considered. But let us begin with the philosophy of well-being.
The Philosophy of Well-beingThere are many different, often conflicting, ideas about what makes a life go well. These different ideas may have quite different implications for how different kinds of medical disorders and treatments are being understood and handled in clinical practice as well as in healthcare policy. For example, they are crucial in assessments of how severe a given disease is considered to be and in predictions about the efficacy of healthcare interventions which, in turn, often constitute criteria for resource allocation in healthcare systems (see e.g. Barra et al. 2020). In some countries, it may also influence decisions on, for example, rights to sick leave and provision of rehabilitative measures at the expense of society (Carr et al. 2001).
In the following, we focus on accounts of well-being rather than theories about illness or health.Footnote 2 We proceed accordingly because we are interested in the evaluative aspects of people’s lives, and for theories about illness and health to account for such aspects, they would, in the end, have to refer to more fundamental views about what make people’s lives go well—views about well-being. The tradition of moral philosophy offers several ways in which theories on well-being can be divided (Fletcher 2013; Kagan 1992; Parfit 1984). The standard way of dividing among theories on well-being in this tradition stems from an appendix in Derek Parfit’s book Reasons and Persons published in 1984. In this tradition, well-being refers to “a life going well for the person whose life it is” (see e.g. Sumner 1996, 20),Footnote 3 or “what is ultimately good for a person” (Crisp 2021).
Parfit (1984, 493–502) distinguished between three kinds of theories: hedonistic theories, desire-fulfilment theories, and objective list theories. Hedonistic theories according to which a life goes well if it contains a balance of pleasure over pain. The hedonistic thesis is that experiences of pleasure and pain are the only relevant elements for a person’s well-being. Desire-fulfilment theories according to which a life goes well if one gets what one wants, prefers, or desires. A person’s well-being is thus constituted by a balance of desire-fulfilment over having one’s desires frustrated or having one’s aversions fulfilled. Objective list theories according to which certain things make a life go well, and these things are considered to do so whether a person wants to have these things or not. Things that usually appear on such lists are freedom, love, pleasure, and virtue.
Distinguishing between objective and subjective theories is one of the crucial manoeuvres here. While this distinction may seem quite straightforward, its importance for theories about well-being, and consequently for healthcare practices, calls for a closer examination. Although Parfit characterized objective list theories as being objective in the sense that”…certain things are good or bad for us, whether or not we want to have the good things, or to avoid the bad things” (Parfit 1984, 493), the standard interpretation of these theories is that the good things are objectively good in the sense that they are considered to be so, irrespective of the person’s attitude towards them. For example, it is good for you to be free irrespective of whether you want to be free or not. According to this interpretation it may be claimed that hedonism is objective in the same sense as objective list theories are (Crisp 2021; Fletcher 2013), given that one can experience pleasure that one does not want to experience. That is, one may experience pleasure meanwhile one does not have a favourable attitude towards that pleasure. This is the sense in which hedonism may be interpreted as an objective list theory (but with only one thing on its list). Perhaps guilty pleasures are such examples, you may experience pleasure while torturing cats but you wish you did not. Accordingly, the main idea is that these theories are subjective in the sense that they are dependent on the individual’s attitudes. For example, Lin (2017) states that “ … subjectivism says that something is basically good for you just if, and to the extent that, you have a certain favorable attitude, A, toward it under the right conditions, C” (354).Footnote 4 Accordingly, the defining characteristic for the subjective/objective distinction is attitude-dependence. This leaves us with desire-fulfilment theories as the only example of subjective theories about well-being.
Let us pause here and take a step back. These accounts about well-being may strike one as too abstract. Indeed, there is a general worry within analytic philosophy that the level of abstractness and idealization at which analytic philosophy is taking place make theories unable to account for the messiness of everyday life (Burman 2023). The more ideal a theory is, the more it disregards the complexities in everyday life. By abstracting aspects away (as is necessary in ideal theorizing) one risks make important aspects invisible.
The carpenter, the physician, and the shop-assistant are embedded in various kinds of relations. Consider, for example, a hedonistic evaluation of the physician’s well-being. According to such an evaluation, her relations to her children and husband are relevant to the extent they contribute to her experienced pleasure. Accordingly, her relations may well be instrumentally valuable but do not have any value for their own sake. Consider next, objective-list theories, here some relations may be characterized as objective goods. For example, Fletcher (2013) suggests that friendship is one such good. Accordingly, objective list-theories may account for the importance of relations as constituents of well-being.
How would this issue be understood by adherents of relational approaches? One may suggest that the correct answer here would be that they typically would adhere to objective list theories about well-being. However, relational approaches want to do something quite different. In the next section we spell out our interpretation of the relevance of their project for understanding the notion of well-being.
The Individual, the Collective, and the RelationalHitherto, we have discussed individualistic accounts of well-being. In “What is Group Well-being?,” Wiland (2022) discusses the difficulties and importance of thinking about the relationship between an individual’s well-being and the well-being of a group. He pedagogically shows how measuring this is much more complicated than understanding a group’s well-being in terms of the addition of the well-being of the individuals making up the group or an average of the same individuals’ level of well-being. Rather we must think about how the well-being of individuals and groups affects each other, in top-down and bottom-up ways and the external factors that may be simultaneously affecting them both. What his arguments point to, among other things, is that groups come in many different shapes, forms, and raisons d’etre. What the group looks like, how it works, and what it does, matters for the question of how an individual fares in it. If we are interested in a person’s well-being as related to the group’s well-being, we need to have tools to understand the relationship between the individual and the group as well as the relations between different members in the group.
Tools to figure out that relationship do, however, exist. In the literature on bioethics, there is an increase in approaches that refer to themselves as “relational.” However, relational approaches may be relational in several different ways. Gary (2023) spells out four kinds of difference in this respect. In her own words: “I emphasize four axes of difference rather than distinct types of relational approaches in order to more closely capture how they appear in the literature …” (Gary 2023, 734). Whereas the relational accounts referenced by Gary have primarily focused on questions about relational autonomy and care ethics as well as the relation between humans and non-human things, we are interested in how a relational angle on the notion of well-being may play out.
The first difference has to do with the scope of relations considered which is about which beings that can constitute a part of the relevant relation. For example, while some approaches ascribe responsibilities to certain relations between human beings, other would include relations to non-human animals as well as inanimate things.
The second difference concerns the nature of relations considered, more specifically, the kinds of relations that are considered primary for theorizing. Gary contrasts between, on the one hand, accounts that primarily focus on structural relations and, on the other hand, those that focus on more-than-human relations. The former kind of approach focuses on structural relations rather than interpersonal relations since these relations are crucial for understanding how people situate themselves. For example, in the words of Koggel “ … those who are oppressed are forced to situate themselves in relation to their oppressors” (Koggel 1997, 158). The latter approaches focus on more-than-human relations which may involve everything from human and non‐human animals to ecosystems and plant species to technological and social artifacts.
The third difference is about causal versus constitutive accounts of selfhood which is concerned with to what extent an account takes relations to be determinative of selfhood. According to causal accounts, relations are necessary for developing certain capacities (such as reflection and deliberation), whereas constitutive views say something more, namely that “ … relationships are ontologically prior to individuals …” (Gary 2023, 737, see also Mackenzie and Stoljar 2000, 22).
The fourth difference is about integrity of individual selfhood. This difference is related to the causal versus constitutive difference. That is, if one accepts that relations are prior to individuals, to what extent is there an individual self left to discuss?
Furthermore, sometimes there are relational aspects which become (in)visible because of the methodological approaches employed. While this is not the place for an extended discussion on theories of science, the interdisciplinary approach of this paper and the larger meta-epistemology project we are part of has brought together authors with three very different academic backgrounds working in radically different knowledge paradigms. One aspect of collaborating across disciplines and paradigms that we continuously are dealing with is trying to make sense of the “same” research object (in our case, PCC) when our research methods are producing very different understandings of that object. But even within the same disciplinary areas, methodological diversity creates ontological complexity. For example, some more traditional methods within sociology include ethnographic observations, surveys, group or individual interviews, but these have been complemented by more recent ones which rely on computer analysis of demographic data, data sometimes gathered by states, other times by private actors, and sometimes harvested out of the internet. Sometimes this methodological and ontological complexity is very frustrating. But it can also be useful. For example, qualitative methodological tools like observation and interviews can produce materials which help us see and articulate the group/individual relationship and its implications for health. Not only does this complement more traditional quantitative measures of health that form the basis of many PCC conversations, but such qualitative methodological work when connected to critical theory may shift a conversation about, for example, causal vs constitutive to a conversation about an individual’s relation to social expectations, power structures and the distribution of responsibility for oneself and others across multiple actors (individuals—partners, children, care providers and groups—families, work places, congregations, healthcare structures, etc.).
Back in the 1950’s, Parsons looked at this in his theorizing about the sick role and how a person’s health status was legitimated through different roles they had within a group and how this was related to the groups need for individuals to be healthy. In another mid-century American work, this time on mental health in rural areas, Eaton and Weil spoke about the individual and group by exploring different ways groups take care of (and sometimes repress) individuals (Eaton and Weil 1955). A bit later, and a bit more radically, Illich (1975) criticized the way modern medicine created a fissure between the individual from their group, leading to less well-being for both. Individuals which did not have the group to take care of them were isolated and less well-off. At the same time, groups with individuals who were not well integrated did not function as well. One of his many points was that as modern medicine took over the role of healthcare, “care” became less of a concern for the family, which isolated modern individuals and simultaneously destroyed much of what was good about the family group.
The field of women’s health has also often touched on the complex relationships between individuals and the expectations different groups (families, professions, social collectives of various sorts) make upon women. In this research, it becomes very clear that the well-being of a group can increase in an inverse relationship to the individual’s well-being if that individual is expected to provide work and care for others in the group in disproportionate and exploitative ways (see Davis 2002; Martin 1987; Rapp 1998; Thompson 2005; Cacchioni 2015).
Gender is not the only line along which power dynamics travel that has significance for health in the relationship between a group and individual. Theories about power and age, class, race, educational level, sexuality, gender identity, geographical location, legal regulations, etc., all show their analytical significance if we want to discuss the well-being of individuals and groups. There is a large body of work on this coming from fields like critical medical humanities (Whitehead and Woods 2016; Wailoo et al. 2010; Williams et al. 2011), exploring how power dynamics, group health and individual health are related to well-being. Tangential to this work is also the research that shows how material constraints and affordances of medical technologies play together to produce bodies, diseases, and health (Mol 2002; Löwy 2015). This work has fed into studies from within feminist technoscience and STS that is concerned with the messy entanglements producing material-discursive subjectivities in situated contexts. Other approaches, for example within feminist phenomenology, are more focused on the subject’s lived experiences that create an understanding of the self (Käll and Zeiler forthcoming). But all of these are interested in relational ways of being in and with the world and how this shapes, affords, impacts, or allows for the experience of the subject.
Similar methods and insights have also already been applied specifically to PCC. For example, in the afterword of Under the Skin, Villarosa uses her analysis of the construction of black health to examine how black Americans have been impacted by the COVID-19 pandemic. There are surely soon many more to come. In the framework of our discussion, we can take inspiration from these approaches to see how collectives and their responsibilities for and expectations on individuals may be impacting the three patients described below. This approach will then make relevant different potential causes or constituents of well-being, with a sensitivity to the contextual power structures within which they are living.
Comments (0)