
Remember me
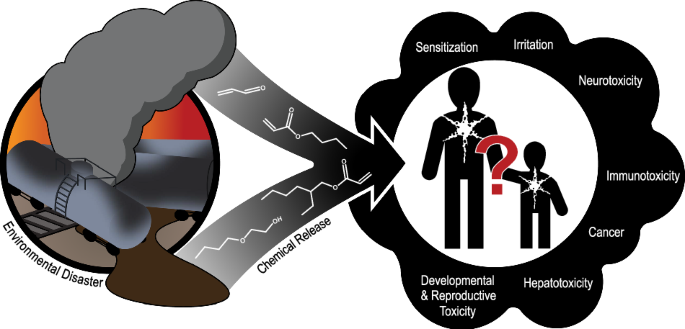

We reviewed and extracted a total of 134 resources (e.g., reviews, reports, databases) from authoritative sources across the 22 chemicals in Phase 1 (see Supplemental Excel File Table S1). Phase 1 results summarize and collate existing conclusions from authoritative sources on health outcomes associated with each chemical. We created an overview/map of the evidence (see Fig. 3) using the collated health outcome data from each authoritative source for the 22 chemicals (see Tables S4, S5, and S6 for supporting information; Table S5 [priority chemicals] and Table S6 [potentially related chemicals] summarize the health hazard conclusions and information across the authoritative sources). The maps provide information on whether, for each chemical, there was a health hazard conclusion and, if so, the confidence of the evidence or severity of the outcome (e.g., higher, moderate, lower) stratified by chemical priority (see Methods). If authoritative conclusions were not available, the maps indicate whether the studies in the reviewed sources suggested an association or if no/few studies were available. For some health outcomes (e.g., endocrine, immune, gastrointestinal, renal) there were few authoritative sources identified for chemicals. These health categories were combined as “Other Organs” for reporting purposes. We integrated determinations based on additional data from the targeted Causaly reviews with information from the authoritative reviews for select chemicals (acrolein; 2-butoxyethanol; diethylene glycol; dipropylene glycol; hydrogen chloride; and 1,2 propylene glycol).
Fig. 3: Summary of findings from authoritative sourcesa for 16 Primary East Palestine chemicals of interest and potentially related East Palestine Chemicals.
Summary of conclusions and other information from authoritative sources for 16 primary chemicals of interest and five PFAS chemicals and TCDD. See Fig. 2 and Tables S5 and S6 for more details. A list of authoritative sources is available in Fig. 2. For vinyl chloride and skin sensitization, one source reported Category 1 sensitization and another source reported that classification was not possible. “Conclusions available” relate to language used by authoritative sources as follows (see Fig. S2) : inadequate evidence (IE) = nonclassifiable (cancer); limited animal evidence (LA) = nonclassifiable (cancer); lower confidence or severity (LC) = possibly (cancer), suspected (noncancer), irritant category with other conflicting data, conflicting sensitizing data; moderate confidence or severity (MC) = probably (cancer), presumed (noncancer), animal data-derived risk estimate value, Category 3 (irritant), Category 1B (sensitizer); higher confidence or severity (HC) = known (cancer, noncancer), human data-derived risk estimate value, Category 1 and 2 (irritant), Category 1 A (sensitizer). 6:2 FTNO = 6:2 fluorotelomer sulfonamido amine oxide; 6:2 FTSHA = 6:2 fluorotelomer thiohydroxyammonium; 6:2 FTSAS = 6:2 fluorotelomermercap-toalkylamido sulfonate; 6:2 FTSA = 6:2 fluorotelomer sulfonic acid; 6:2 FTSA-PrB = 6:2 fluorotelomer sulfonamide alkylbetaine; PFAS = per- and polyfluoroalkyl substances; TCDD = 2,3,7,8-tetrachlorodibenzo-p-dioxin.
Irritation and sensitization Primary chemicalsTesting or health characterization of chemicals was the most complete for acute effects such as irritation or sensitization (see Fig. 4). Most chemicals were classified as causing skin (10 of 16 chemicals) or eye (11 of 16 chemicals) irritation, including all the higher-priority (i.e., highest and high-priority) chemicals, two moderate-priority chemicals (dipropylene glycol for both outcomes and polypropylene glycol for eye), and one low-priority chemical (petroleum lube oil for both outcomes). Among the higher-priority chemicals, risk assessment values were not found for skin irritation, and available values for eye irritation ranged from 0.0025 mg/m3 for acrolein to 180 mg/m3 for vinyl chloride (see Table S5). The reviews concluded that diethylene glycol was not associated with skin or eye irritation, and 1,2 propylene glycol was not associated with eye irritation. No other conclusions were identified for the other moderate- and low-priority chemicals. Half of the chemicals caused respiratory irritation, seven of which were higher-priority chemicals. Polypropylene glycol was not considered a respiratory irritant. Risk assessment values for high-priority chemicals and respiratory irritation ranged from 2 × 10−5 mg/m3 for acrolein to 180 mg/m3 for vinyl chloride (see Table S5). No definitive authoritative conclusions were found for benzene, three of the five moderate-priority chemicals, and all three low-priority chemicals. However, the reviews reported individual study findings for benzene, diethylene glycol, and 1,2-propylene glycol. Adverse respiratory effects or irritation from multiple chemicals are consistent with reported symptoms (e.g., running nose; congestion; coughing; burning nose, throat, or eyes; irritation) from the affected community and first responders in CDC’s ACE Survey [4].
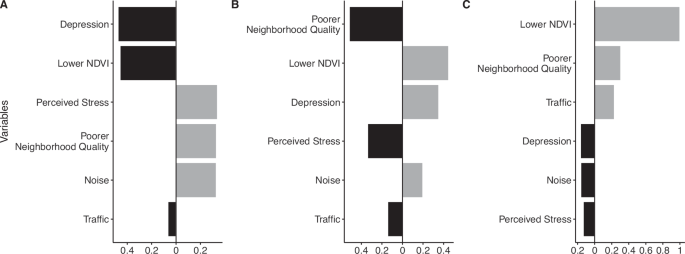
Fig. 4: Authoritative conclusions for 16 primary chemicals: A. irritation and sensitization, B. Noncancer outcomes, and C. Cancer outcomes.
Summary of irritant and sensitizer information, non-cancer and cancer outcomes from authoritative sources for 16 primary chemicals of interest. Detailed findings for each chemical × health outcome category are reported in Table S5 and Supplemental Excel Table S1. The “Other Organ” category includes double counts for two chemicals (acrolein and 2-butoxyethanol), wherein different conclusions were available for different organ systems NS = no or few studies, ES evidence suggestive, NL not likely to be irritating or sensitizing or risk for health outocme, LC lower confidence, MC moderate confidence or severity, HC higher confidence or severity. See Fig. S2 for more details.
While some authoritative sources discussed skin sensitization in the context of immune effects, skin sensitization was characterized as a separate outcome category in this review. Three higher-priority chemicals were categorized for skin sensitizing effects (butyl acrylate, 2-ethylhexyl acrylate, and vinyl chloride). The European Chemicals Bureau (ECB) [41] discussed sensitizing data for acrolein, another higher-priority chemical, but did not categorize it for sensitization. Little or no indication of skin sensitization was reported for seven chemicals (2-butoxyethanol, benzene, hydrogen chloride, diethylene glycol, dipropylene glycol, polypropylene glycol, and 1,2-propylene glycol). No conclusions were available for the remaining chemicals.
Potentially related chemicalsFor PFAS, one chemical (6:2 FTSA) was classified for corrosive effects to the skin, whereas three chemicals (6:2 FTSHA, 6:2 FTSA-PrB, and 6:2 FTNO) did not have irritating effects to the skin in studies reported in Phase 1 sources. Conclusions for eye irritation were available for two chemicals (6:2 FTSHA and 6:2 FTSA); some irritation was reported following exposure to 6:2 FTSA-PrB in rabbits, and no eye irritation was predicted for 6:2 FTNO. Data were not available for categorizing irritating effects to the respiratory system following PFAS exposures. Authoritative sources reported little or no concern for skin sensitization following exposure to three chemicals (6:2 FTSA, 6:2 FTSA-PrB, and 6:2 FTNO). Mixed results were reported from animal and in vitro studies for one chemical (6:2 FTSHA). Skin sensitization data were not available for the remaining PFAS (6:2 FTSAS). TCDD was classified as causing irritation to both the skin and eyes. Additionally, reviews emphasized that high-level exposures to TCDD can cause moderate to severe chloracne, an acne-like eruption of the skin, and other skin rashes and discoloration. There were no conclusions for TCDD and respiratory irritation, although one review reported upper respiratory irritation in humans following inhalation. Skin sensitization was not classified for TCDD because few data were available. No chemicals were forwarded to Phase 2 for these outcomes because there were no gaps for the highest priority chemicals.
Other noncancer outcomes Primary chemicalsAuthoritative conclusions for reproductive and developmental toxicities were available for approximately half of all chemicals (see Fig. 4 for noncancer outcome findings). Of the eight higher-priority chemicals (see Fig. 3 for chemical-specific determinations and priority categories), two chemicals (benzene and vinyl chloride) may be linked to developmental effects based on determinations. California Environmental Protection Agency (CalEPA) Proposition 65 [42] lists benzene as a chemical that can cause developmental and reproductive effects; other reviews agreed with the developmental effects conclusions (particularly for developmental hematotoxicity) but stated that the evidence for reproductive effects was limited. Available risk assessment values for developmental effects from inhalation exposure (mg/m3) are 0.027 for benzene (CalEPA Office of Environmental Health Hazard Assessment [OEHHA] REL for acute exposure) and 1.30 for vinyl chloride (ATSDR MRL) (see Table S5). Although positive associations have been observed for adverse reproductive (e.g., effects to reproductive organs or in pregnant animals) or developmental outcomes and exposure to several higher-priority—acrolein, 2-butoxyethanol, butyl acrylate (developmental only)—and moderate-priority chemicals—diethylene glycol—these effects occurred at high doses or at doses causing maternal toxicity. As a result, several authoritative sources (primairly ECHA) concluded that the chemicals are not significantly toxic to reproduction or the developing fetus. There was low concern for reproductive toxicity following exposure to butyl acrylate based on studies showing no adverse effects. There was also low concern for developmental and reproductive toxicity for 2-ethylhexyl acrylate and two moderate-priority chemicals, isobutylene and 1,2 propylene glycol. Unclear or no conclusions were available for both reproductive and developmental effects for the remaining higher-priority chemicals: hydrogen chloride and phosgene gas.
Health outcome conclusions were typically not available for neurotoxicity (14 of 16 chemicals) and immunotoxicity (14 of 16 chemicals). Vinyl chloride was deemed a presumed neurotoxicant and a suspected immunotoxicant, and benzene was associated with both neurotoxicity in workers exposed to high doses and adverse immune effects. Some authoritative sources noted that some immunotoxicity outcomes associated with benzene exposure may result from hematotoxicity or may occur at levels like those inducing hematotoxicity.
Exposures to higher-priority chemicals were also associated (higher or moderate confidence) with other adverse health outcomes. The most sensitive available risk estimates for these higher-priority chemicals (see Tables S5 and S6) are reported in Box 1.
Given identified research gaps for the higher-priority chemicals, we selected the following chemical × outcome pairs for Phase 2 activities (see Methods): neurotoxicity for acrolein, 2-ethylhexyl acrylate, butyl acrylate, and 2-butoxyethanol; immunotoxicity for butyl acrylate and 2-butoxyethanol; and hepatotoxicity for butyl acrylate. Although vinyl chloride is most likely the chemical of most concern, we did not select it for Phase 2 because a recent ATSDR review was available with conclusions about the selected health outcomes.
Potentially related chemicalsECHA classified 6:2 FTSHA as a presumed toxicant to fertility and development. Two PFAS (6:2 FTSA and 6:2 FTNO) were not associated with reproductive or developmental toxicity, and no conclusions were available for the remaining PFAS (6:2 FTSAS and 6:2 FTSA-PrB). Several agencies (e.g., OEHHA, EPA, ATSDR) have concluded that TCDD can cause adverse reproductive and/or developmental effects and have developed risk estimates based on these effects (EPA Integrated Risk Information System [IRIS] RfD: 7 × 10 − 10 mg/kg/day for oral exposure) (see Table S6). TCDD was also associated with both neurological and immune effects based on available human and animal evidence.
Cancer outcomes Primary chemicalsCancer conclusions were available for approximately two-thirds (12 of 16) of the chemicals (see Fig. 4). Of the eight higher-priority chemicals, five can cause cancer in humans or experimental animals: Benzene and vinyl chloride are IARC and NTP “known human carcinogens” [43,44,45,46], acrolein is “probably carcinogenic to humans” based on mechanistic and animal cancer data (IARC 2A), 2-ethylhexyl acrylate is “possibly carcinogenic to humans” (IARC 2B) based on sufficient evidence from studies in experimental animals, and 2-butoxyethanol induces tumors (hemangiosarcoma of the liver in male mice). IARC considered the evidence limited in experimental animals for 2-butoxyethanol and, thus, not classifiable as a carcinogen (Group 3). Butyl acrylate and hydrogen chloride are also classified as Group 3 by IARC based on inadequate evidence from experimental animal and human studies. No conclusions were available for phosgene gas. Among the moderate- and low-priority chemicals, exposure to isobutylene caused tumors in experimental animals. The others were either not likely to cause cancer or had no identifiable conclusions. Cancer types were available for the known human carcinogens: Benzene causes acute myeloid leukemia and other acute nonlymphocytic leukemia and may cause other lymphohematopoietic cancers (chronic myeloid leukemia, chronic lymphocytic leukemia, childhood leukemia, non-Hodgkin lymphoma, and multiple myeloma) and lung cancer; vinyl chloride causes angiosarcomas in the liver.
Taking into account these research gaps, we identified the following chemicals for Phase 2 searches for cancer outcomes: human cancer studies for acrolein, 2-ethylhexyl acrylate, and 2-butoxyethnanol; and human and animal cancer studies for butyl acrylate.
Potentially related chemicalsFor dioxins, most available cancer outcome data were for TCDD. Both IARC [47] and NTP’s Report on Carcinogens [48] classified TCDD as “carcinogenic to humans” based on sufficient evidence in humans (Group 1). OEHHA [49] provided slope factors for TCDD and a variety of individual chemicals in the class. Inhalation slope factors ranged from 3.9 × 101 mg/kg/day (for 1,2,3,4,6,7,8,9-Octachlorodibenzo-p-dioxin) to 1.3 × 105 mg/kg/day (for TCDD and 1,2,3,7,8-Pentachlorodibenzo-p-dioxin) [49]. Data on cancer effects were not available from authoritative sources for the five PFAS or other dioxins.
To increase the utility of our review and because of the limited health information on PFAS and dioxins other than TCDD, we selected 6:2 FTSA, 6:2 FTNO, and dioxins other than TCDD for unrestricted searches (i.e., searches for any health outcome data).
Box 1 Most sensitive available risk assessment values for higher priority chemicals and other noncancer outcomesChemical
Value
Source
Additional information
Hematotoxicity
Benzene
REL = 0.003 mg/m3
OEHHA
Inhalation exposure
MRL = 0.0003 mg/kg/day
ATSDR
Oral exposure; Based on hematotoxicity/immune effects
2-butoxyethanol
MRL = 0.97 mg/m3
ATSDR
Inhalation exposure
RfD = 0.1 mg/kg/day
EPA IRIS
Oral exposure
Hepatotoxicity
2-butoxyethanol
MRL = 0.07 mg/kg/day
ATSDR
Oral exposure
Vinyl chloride
RfD = 0.003 mg/kg/day
EPA IRIS
Oral exposure
Respiratory (non-irritating effects)
Phosgene gas
RfC = 0.0003 mg/m3
EPA
Inhalation exposure
Phase 2OverviewResults from the targeted searches and screenings conducted during Phase 2 are available in Table 1.
Table 1 Overview of literature search results for selected chemical-outcome pairs for primary chemicals. Primary chemicalsFor five searches (acrolein × cancer, 2-ethylhexyl acrylate × cancer, 2-ethylhexyl acrylate × nervous, butyl acrylate × hepatic, butyl acrylate × nervous), no relevant results were identified during title-abstract and/or full-text screening. At least one PECO-relevant reference was identified for each of the remaining six searches (acrolein × nervous [n = 8], 2-butoxyethanol × cancer [n = 1], 2-butoxyethanol × immune [n = 10], 2-butoxyethanol × nervous [n = 4], butyl acrylate × cancer [n = 1], butyl acrylate × immune [n = 5]). Although five PECO-relevant studies were identified for butyl acrylate × immune, all five reported on skin sensitization findings only. As skin sensitization data were considered separately from immune data during Phase 1, the five studies were not considered for further analysis during Phase 2.
For chemical × health outcome pairs with at least one new study that had not been included in authoritative reviews (acrolein × nervous, 2-butoxyethanol × cancer, 2-butoxyethanol × immune, and 2-butoxyethanol × nervous), we examined and summarized all studies identified during Phase 2, alongside some findings from authoritative source reports in Phase 1. Findings for each chemical × health outcome pair are summarized by endpoint in the text (acrolein × nervous and 2-butoxyethanol × cancer) and Table S7 (2-butoxyethanol × immune) and Table S8 (2-butoxyethanol × nervous) below. Figure S3 captures the literature identified and included at each step for these searches. An interactive version of this flow diagram is available on Tableau (see figure caption).
Potentially related chemicalsNo relevant results were identified during title-abstract and/or full-text screening for 6:2 FTNO × any health outcome. At least one PECO-relevant reference was identified for 6:2 FTSA × any health outcome (n = 2) and dioxins other than TCDD × any health outcome (n = 11). All studies identified during Phase 2 were summarized, alongside some findings from authoritative source reports in Phase 1. Information on the literature identified and included during these searches is also included in Fig. S1.
Selected chemical-outcome: Acrolein-nervous systemFour authoritative reviews—ATSDR [50] (12 studies), ECB [41] (1 study), EPA [51] (1 study), and OEHHA [52] (4 studies)—discussed findings from studies examining acrolein exposures and neurological effects, although none made hazard conclusions. Additionally, outputs from Causaly identified reviews and primary articles that discussed potential associations between acrolein levels and various neurological outcomes, including Alzheimer’s disease, Parkinson’s disease, and strokes.
Our literature scoping search to find published reviews on neurological outcomes identified eight reviews discussing effects and mechanisms associated with acrolein exposure in humans [53,54,55,56,57,58,59] and animals [53,54,55,56, 58,59,60], which are summarized below. One review was discussed in ATSDR, 2007 [60], but the remaining seven were not included in any authoritative sources. The four authoritative reports also included 14 primary studies in experimental animals—reporting effects related to neurotransmitter (neuropeptide) depletion, increased brain weight, inflammatory responses, loss of nerve tissue, and nonspecific histopathological effects (in inhalation studies)—and one primary study in humans that reported increased acrolein levels in the brains of Alzheimer’s patients compared to control subjects at autopsy. Most studies discussed in the ATSDR Toxicological Profile examined general toxicity in experimental animals and were not designed to measure neurotoxicity. Detailed results from the eight reviews identified in our literature scoping search are provided in the text below. As our search identified reviews only, a summary table is not provided. Importantly, exposure to acrolein can occur both exogenously and endogenously, as the chemical is a byproduct of lipid peroxidation initiated by oxidative stress [56]. In the eight identified reviews, acrolein is often used as a biomarker for oxidative stress and lipid peroxidation. Therefore, it was often unclear whether neurological effects are related specifically to acrolein or as a biomarker for oxidative stress. The review findings should be considered in this context.
Three other reviews identified during Phase 2 reported on the mechanistic effects of acrolein in nervous tissues [61,62,63], although mechanistic evidence was not the primary focus of our literature scoping activities. Acrolein was discussed as a highly toxic product of lipid peroxidation that can cross the blood-brain barrier [61]. In vitro and in vivo studies of neuroinflammation and neurodegeneration and acrolein’s role in the development of Alzheimer’s disease, Parkinson’s disease, and spinal cord injury were cited as evidence of its neurotoxic potential. Other reported mechanistic evidence suggests that acrolein induces demyelination of nerves—which impacts nerve conduction—neuronal apoptosis, neurotransmitter alterations, and protein adduct formation. Other reviews reported inhibition of glutamate and glucose uptake in acrolein-exposed neuronal cell cultures [62] and disruption of nerve terminals and subsequent potential for synaptic damage in in vitro studies [63]. These reviews suggest that acrolein, whether endogenous or exogenous, has the potential for neurotoxic effects.
Reviews of human and animal studies discussed the association between acrolein and strokes of varying severity [53, 55,56,57]; however, the discussion of acrolein’s role differed across reviews. Some reviews assessed acrolein’s role in the development of stroke or brain infarction, whereas others examined acrolein as a byproduct of the oxidative stress induced by stroke or brain infarction and its potential to cause additional neurological damage. Acrolein may be produced endogenously during ischemic stroke [53], and increased endogenous acrolein production has been reported in connection with both severe strokes and silent brain infarctions [57]. A mechanistic study summarized by Muguruma et al. [57] suggested that acrolein elicited a cycling of oxidative stress, resulting in stroke-related neuronal damage, and is a suspected driver of neuronal damage in stroke patients. Plasma levels of protein-conjugated acrolein (along with acrolein-producing enzymes) were shown to be appropriate biomarkers for human stroke [54,55,56, 58] and silent brain infarctions [55]. Multiple human studies have found dysregulated acrolein metabolism in stroke patients [53].
Findings from reviews of animal studies further support an association between acrolein and stroke, although it was unclear whether animals were dosed in studies cited in the reviews or whether effects were associated with endogenous acrolein. A review of animal studies reported an association between decreasing levels of acrolein and decreased infarction size [53]. A study in mice indicated that, during brain infarction, acrolein is “more strongly involved” in cell damage than reactive oxygen species [55]. Other reviews reported increased levels of acrolein at the site of brain infarction in mouse models [54, 58]. Neuronal damage was also reported in a review of animal studies, including acrolein-induced neuronal damage in pigs and rats, although some studies reported effects of endogenous acrolein only and should be considered accordingly [56]. In an in vitro study, acrolein induced mitochondrial dysfunction leading to neuronal death in HT22 mouse hippocampal cells [56].
Other neurological outcomes have also been considered for their association with acrolein exposure. In humans, significantly increased levels of acrolein were reported in the brains of patients with mild cognitive impairment [55,
Comments (0)