
Remember me

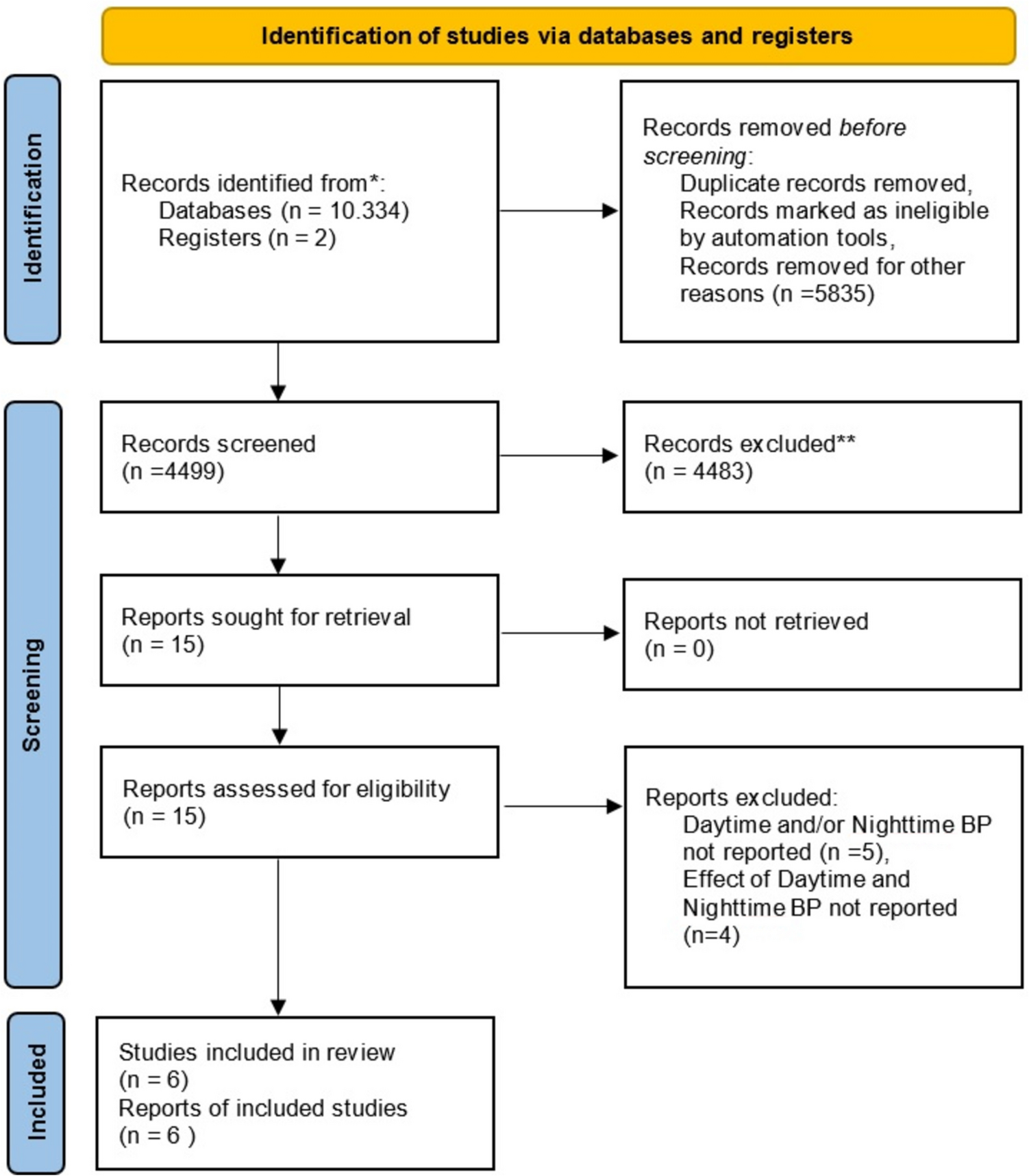



A flow diagram of the selection process is depicted in Fig. 1. A total of 1186 potentially relevant articles were identified from PubMed, Scopus, and EBSCOhost databases. After removal of duplicates (n = 360) using Rayyan software, 826 articles were available for title and abstract screening, after which 779 articles were excluded for reasons including: i) outcomes and publication types outside the scope of this review; ii) studies with biomarkers measured in serum, plasma or other bodily fluids; iii) animal, genetic and intra-uterine studies; and iv) studies focusing on pre-eclampsia or maternal hypertension. Among the 47 articles selected for full-text screening, 25 were excluded as they did not report outcomes of interest for this review (n = 14), did not measure kidney function biomarkers in urine (n = 4), focused on genetics (n = 2), were publication types outside the scope of this review (n = 2), had no full-text articles available (n = 2) or the article was retracted (n = 1).
Fig. 1
Preferred Reporting Items for Systematic Reviews and Meta-analyses flow chart of the study selection
Study CharacteristicsThe main characteristics of the studies reviewed are summarised in Table 1 and Table 2.
Table 1 Main characteristics of studies reporting associations between kidney biomarkers and blood pressureTable 2 Main characteristics of studies reporting associations between kidney biomarkers and markers of target organ damageThe majority of studies identified had an observational design, including 12 cross-sectional [35, 36, 38, 42, 45,46,47,48, 50,51,52, 55], nine prospective [37, 39,40,41, 43, 49, 53, 54, 56] and one case control study [44]. Additionally, almost half of the studies (n = 9) were conducted in North America [36, 37, 43, 45, 48,49,50, 54, 55], followed by studies done in South Africa (n = 3) [35, 44, 47], China (n = 2) [40, 42], Japan (n = 2) [39, 51], while the remainder of the studies were conducted in Italy (n = 1) [41], Croatia (n = 1) [46], Czech Republic (n = 1) [38], Switzerland (n = 1) [52], Germany (n = 1) [53] and Serbia (n = 1) [56] (Fig. 2). Furthermore, the studies encompassed a wide range of age groups (Fig. 3), including seven studies in children and adolescents (aged ≤ 19 years) [35, 38, 43, 49, 50, 52, 54], two studies in young adults (aged between 20–44 years) [46, 47], seven studies in middle-aged adults (aged between 45–64 years) [37, 40, 41, 44, 48, 53, 55] and six studies in elderly individuals (aged ≥ 65 years) [36, 39, 42, 45, 51, 56].
Fig. 2
Percentage of studies done in different countries
Fig. 3
Number of studies in different age groups per kidney function biomarker. A darker shade of colour indicates studies focusing on blood pressure, while a lighter shade of colour indicates studies focusing on markers of target organ damage. Abbreviations: uA1M, urinary alpha-1 microglobulin; uNGAL, urinary neutrophil gelatinase-associated lipocalin; uUMOD, urinary uromodulin
The original and standardised quality scores of all the included studies are indicated in Supplementary Tables 2–4, Online Resource 1. The overall study quality was high, with a median quality score of 9 (range: 6–10). No low-quality studies were included.
Associations Between Biomarkers of Kidney Function and Blood PressureAmong the 19 studies that focused on associations with blood pressure, most included uA1M (n = 9) and uUMOD (n = 8) as biomarkers of kidney function, followed by uNGAL (n = 6), while CKD273 was the least investigated biomarker (n = 2).
uA1M: In an analysis performed in 957 children (Black; n = 526 and White; n = 431) from the Exercise, Arterial Modulation and Nutrition in Youth South Africa (ExAMIN Youth SA) study, Craig et al. [35] reported a positive association between urinary alpha-1 microglobulin-to-creatinine ratio (uA1M/Cr) and office systolic blood pressure (SBP; β = 0.15; 95% CI, 0.06 to 0.19; p < 0.001), diastolic blood pressure (DBP; β = 0.18; 95% CI, 0.09 to 0.24; p < 0.001) and mean arterial pressure (MAP; β = 0.11; 95% CI, 0.02 to 0.17; p = 0.018) in the Black group, as well as a positive association between uA1M/Cr and DBP (β = 0.10; 95% CI, 0.01 to 0.25; p = 0.038) in the White group. In the same study, it was found that the likelihood of elevated BP increased with 28% (Odds ratio = 1.28; 95% CI, 1.10 to 1.50) with each standard deviation increase in uA1M/Cr in the Black group (p = 0.002) [35]. In a large-scale study of 2436 participants in the Systolic Blood Pressure Intervention Trial (SPRINT) [36], it was found that each standard deviation increase in SBP at baseline (16 mmHg) was associated with higher levels of uA1M (10%) and lower levels of uUMOD (−2%) (all p < 0.05), while no association was observed with uNGAL. On the other hand, in a recent study by Khan et al. [37] with a median follow-up period of 9.9 years in 1170 adults in the Coronary Artery Risk Development in Young Adults (CARDIA) study, no statistically significant association of uA1M and uUMOD with incident hypertension or with a 10-year change in SBP or DBP was evident. Similarly, in a small-scale study on 37 children with Autosomal Dominant Polycystic Kidney Disease (ADPKD), Seeman et al. [38] found no significant correlation between uA1M/Cr and office blood pressure index.
In a study conducted by Ishiwata et al. [39] with a median follow-up period of 488 days and involving 623 adults with acute heart failure, it was observed that individuals in the higher quartiles of uA1M/Cr were more likely to have higher SBP (138 ± 27 mmHg vs 131 ± 27 mmHg; p = 0.013) and a history of hypertension (64.3% vs 44.4%; p = 0.002). In an analysis of 1451 participants enrolled in the Incidence, Development, and Prognosis of Diabetic Kidney Disease (INDEED) study with a 10-year follow-up, Sun et al. [40] observed a positive association between office SBP and uA1M levels (p < 0.01) and similarly, in logistic regression analyses, they found significant associations between the high stable SBP group and uA1M levels > 29.75 mg/L (Odds ratio = 2.91; 95%CI, 1.43 to 5.94; p < 0.05). Additionally, in a study with a 6-month follow-up (after the end of antiviral therapy), focusing on 135 Child–Pugh A cirrhotic patients receiving direct acting antiviral treatment for chronic hepatitis C, Bilioti et al. [41] indicated that the presence of hypertension with diabetes was associated with tubular dysfunction (Odds ratio = 4.23; 95%CI, 1.10 to 16.27; p < 0.05), indicated by uA1M/Cr levels > 14 µg/mg. Furthermore, in a study that involved 691 elderly community participants, Wang et al. [42] found that hypertension increased the likelihood of having elevated uA1M/Cr levels (> 15 mg/g) by 38% (Odds ratio = 1.38; 95% CI, 1.02 to 1.93; p = 0.011). These findings were further supported by the fact that 39.9% of individuals with hypertension and 47.2% of individuals with both hypertension and diabetes had increased uA1M/Cr levels in the same study [42].
uUMOD: In a study by Bakhoum et al. [43] with a median follow-up period of seven months that included 436 Chronic Kidney Disease in Children (CKiD) participants, univariate analyses showed that each two-fold higher urinary uromodulin-to-creatinine ratio (uUMOD/Cr) at baseline was associated with 1.66 mmHg (95% CI, −2.31 to −1.00) lower 24-h SBP (p < 0.001), 0.49 mmHg (95% CI, −0.97 to −0.01) lower 24-h DBP (p = 0.05), 1.71 mmHg (95% CI, −2.45 to −0.97) lower clinic SBP (p < 0.001) and 0.90 (95% CI, −1.59 to −0.22) lower clinic DBP (p = 0.01). However, these associations were attenuated with the inclusion of age in the multivariable models [43]. In a study population of 129 Black South Africans, including 71 individuals with clinically diagnosed hypertension-attributed chronic kidney disease (CKD), Nqebelele et al. [44] observed a negative correlation between uUMOD and office SBP (r = −0.23; p = 0.004). In this study, higher levels of uUMOD were also associated with 38% lower odds of having hypertension-attributed CKD (Odds ratio = 0.62; 95% CI, 0.48 to 0.81; p < 0.001) [44].
Additionally, in a study involving 933 participants from the Cardiovascular Health Study, Steubl et al. [45] found that the presence of hypertension was associated with lower uUMOD levels in univariate and multivariate (β = −4.30; 95% CI, −7.50 to −1.10; p < 0.05) analyses. In a recent study focusing on 326 young, middle-aged apparently healthy adults [46], uUMOD/Cr correlated negatively with several ambulatory blood pressure monitoring parameters in both prehypertensive and hypertensive groups. This included a negative correlation with 24-h and nighttime pulse pressure (PP) (Rho = −0.28; p = 0.04 and Rho = −0.31; p = 0.02, respectively) in the prehypertensive group as well as negative correlations with 24-h DBP (Rho = −0.29; p = 0.04), daytime DBP (Rho = −0.27; p = 0.04) and nighttime SBP (Rho = −0.29; p = 0.04) p = 0.03) in the hypertensive group [46]. While an analysis in 956 young apparently healthy adults from the African-Prospective study on the Early Detection and Identification of Cardiovascular Disease and Hypertension (African-PREDICT) study showed no significant associations of uUMOD/Cr and CKD273 classifier with office SBP [47]. In another study done by Muiru et al. [48] involving 198 human immunodeficiency virus (HIV)-positive individuals enrolled in the Multicenter AIDS Cohort Study (MACS) and the Women’s Interagency HIV Study (WIHS), no associations between uA1M, uNGAL or uUMOD and hypertension were observed.
uNGAL: In a study 5-year follow-up study involving 110 children with congenital heart disease enrolled in the Translational Research Investigating Biomarker End Points in AKI (TRIBE-AKI) study [49], no significant differences were found in 5-year median uNGAL concentrations or in the absolute change in uNGAL concentrations from baseline to five years in patients with hypertension compared to those without hypertension. However, in this study, hypertension was associated with a higher proportion of patients with 5-year uNGAL concentrations above normal for their specific age (10% vs 1%; p = 0.03) [49]. In addition, a study involving 31 participants, including 21 type-1 diabetes mellitus patients, Mamilly et al. [50] observed a negative correlation between urinary neutrophil gelatinase-associated lipocalin-to-creatinine ratio (uNGAL/Cr) and nocturnal SBP dipping (r = −0.47; 95% CI, −0.76 to −0.03; p < 0.05). On the other hand, a study that included 147 hypertensive patients, stratified according to eGFR values [51], found no significant correlation between uNGAL/Cr and BP. Similarly, in a small-scale study conducted on 30 children, including 15 children with ambulatory ADPKD [52], no association between uNGAL and MAP was present.
CKD273: In a small-scale study of 32 patients with resistant hypertension undergoing baroreflex activation therapy for six months, Wallbach et al. [53] found no correlation between changes in 24-h SBP values and changes in the urinary CKD273 score. In this study, the data was also stratified according to ambulatory blood pressure response and subsequently, there was a statistically significant (p = 0.011) reduction in the CKD273 score from a mean of 0.16 (95% CI, −0.16 to 0.56) to − 0.44 (95% CI, −0.63 to 0.05) after baroreflex activation therapy in patients with an ambulatory SBP decrease of ≥ 5 mm Hg [53].
Associations Between Biomarkers of Kidney Function and Target Organ DamageAmong the four studies that focused on associations with markers of target organ damage, most studies included uA1M (n = 3), while the other studies focused on uUMOD (n = 1) and uNGAL (n = 1). No studies investigated CKD273 in this regard.
uA1M: Apart from observing an association between uA1M/Cr and blood pressure, Ishiwata et al. [39] also indicated that, when individuals with acute heart failure are stratified according to quartiles of uA1M/Cr, individuals in the higher uA1M/Cr group were more likely to have higher LVEF (55.5% vs 47%; p = 0.002). Another study involving 504 children enrolled in the CKiD study with a 1-year follow-up [54] found that a two-fold increase in uA1M levels was associated with a lower prevalence of left ventricular hypertrophy (LVH) (Prevalence ratio = 0.90; 95% CI, 0.82 to 0.99; p = 0.026). In 393 participants of the Multi-Ethnic Study of Atherosclerosis (MESA) without diabetes, CVD or CKD [55], each two-fold greater concentration of uA1M/Cr was associated with a 1.2% (95% CI, −2.20 to −0.20) lower LVEF (p < 0.05). The latter is further supported by the fact that, when stratified according to uA1M/Cr levels, individuals in the highest tertile of uA1M/Cr had lower LVEF (p < 0.05) [55].
uUMOD: In the MESA study [55], uUMOD/Cr also correlated negatively with left ventricular mass to volume ratio (r = −0.13; p < 0.01). However, these results were no longer significant in multivariable linear regression analyses after adjusting for age, gender, race, education site, blood pressure medications, SBP total cholesterol, lipid-lowering medication, body mass index, eGFR, urine albumin and 1/urine creatinine.
uNGAL: In a small-scale study by Stopic et al. [56] with a follow-up of 18 months in 51 individuals over 18 years of age with CKD, no significant differences were observed in uNGAL levels regarding the presence or absence of cardiovascular events or LVH.
Taking the above into account, it is evident that urinary kidney function biomarkers such as uA1M and uUMOD were more frequently studied in relation to cardiovascular health than
Comments (0)