
Remember me
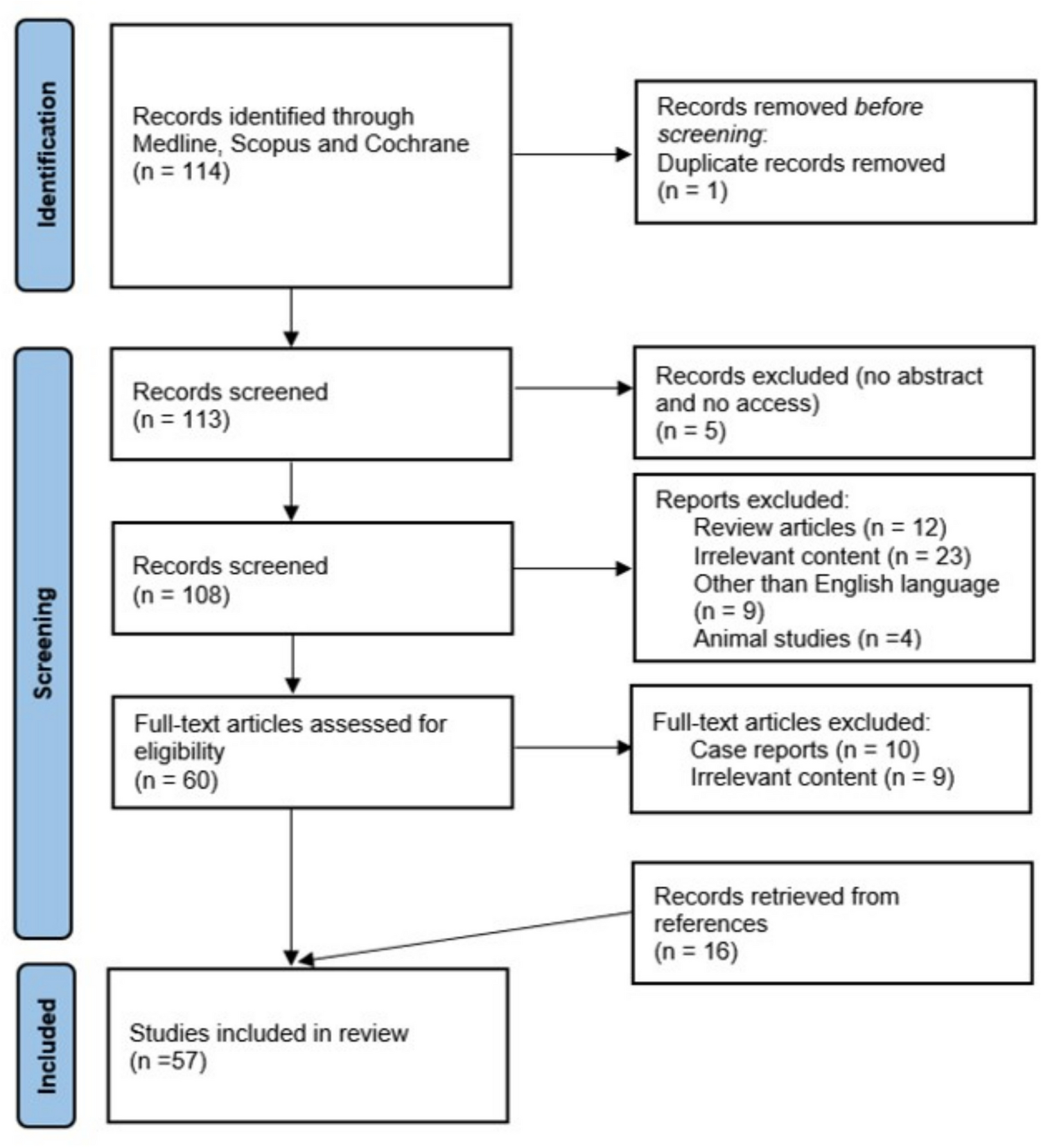

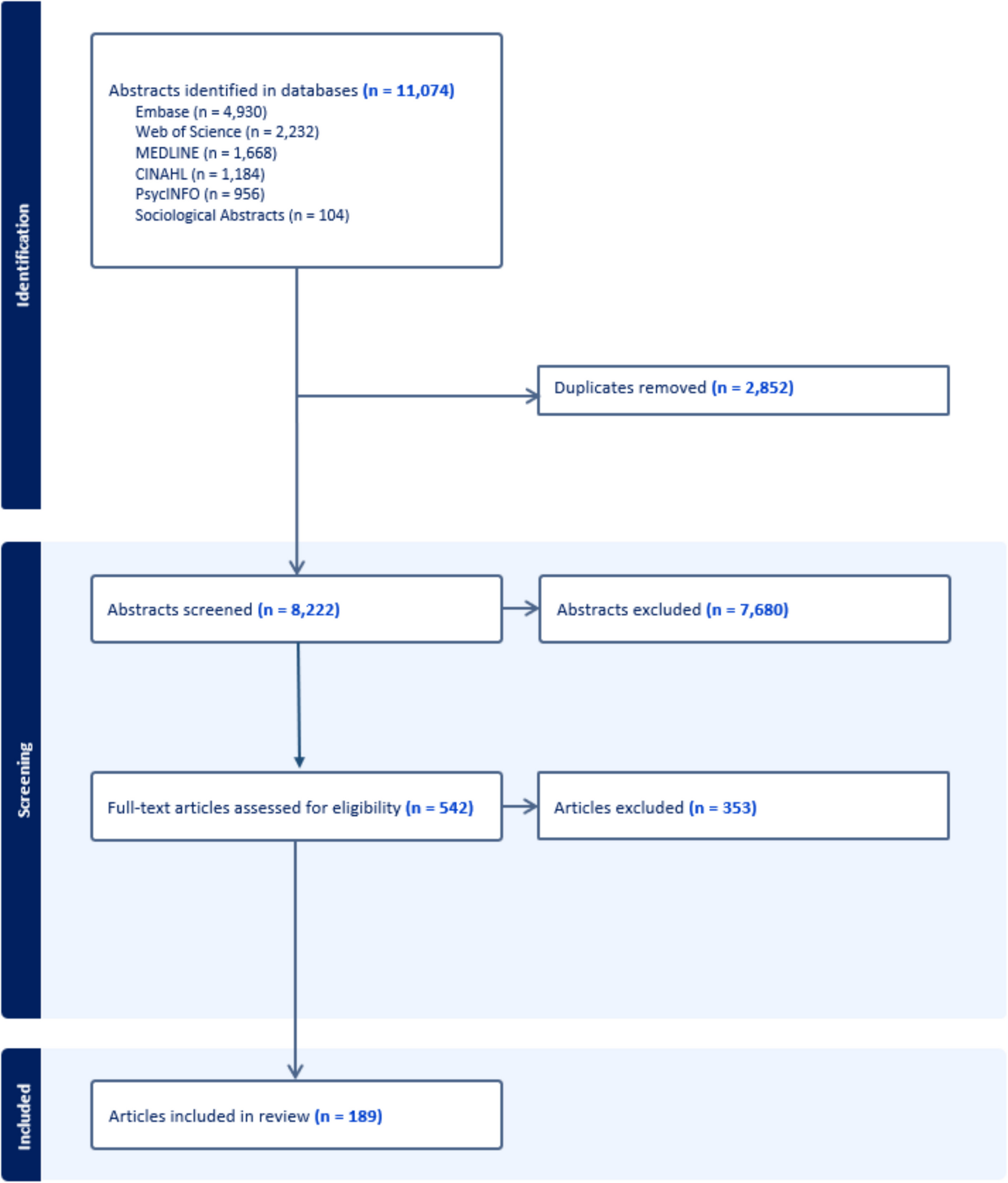
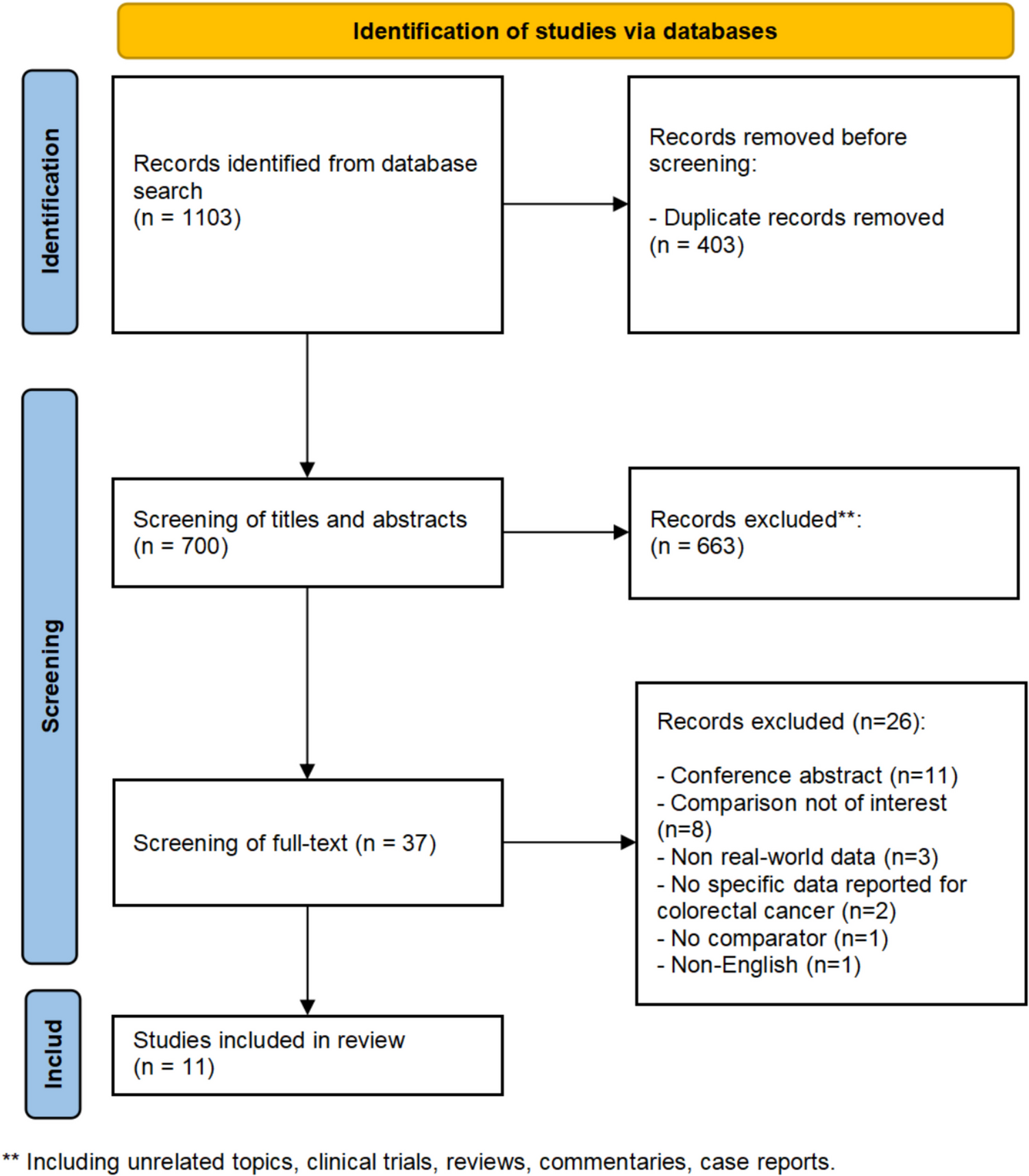
A total of 1,103 records were identified from the three databases. After removing the duplicates (n = 403), 663 records were excluded based on title and abstract screening. The full text of 37 records was then evaluated, and 11 observational studies that used real-world data (all based on electronic health records) were included in this review (Fig. 1) [26,27,28,29,30,31,32,33,34,35,36]. All 11 studies focused on mCRC patients. The majority of the studies were conducted in China (n = 10) [27,28,29,30,31,32,33,34,35,36], and one study was conducted in the United States [26]. Five studies did not report results stratified by MSI-H or MSS tumor type [27,28,29,30, 33], though MSS/pMMR comprised the majority of patient MSI status. Five studies were specifically conducted in the MSS mCRC setting [31, 32, 34,35,36]. One study included two cohorts: cohort one was specifically conducted in MSI-H mCRC setting, while cohort two included both MSI-H mCRC and MSS mCRC patients [26].
Fig. 1
PRISMA flow diagram of the study selection process [22]
Table 1 summarizes the characteristics of the included studies [26,27,28,29,30,31,32,33,34,35,36]. Of those that reported, the median duration of follow-up ranged from 10.8 to 28.4 months. A total of 2,049 patients were included across all studies, with sample sizes varying from 60 to 537 patients (median = 129) [26,27,28,29,30,31,32,33,34,35,36]. The ICIs used in the studies included camrelizumab, nivolumab, pembrolizumab, penpulimab, sintilimab, tislelizumab and toripalimab [26,27,28,29,30,31,32,33,34,35,36]. Comparators included conventional chemotherapy and other medications. Adverse reactions were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events [37].
Among studies involving patients with MSS mCRC, nine included liver metastasis as a prognostic factor in their analyses [27, 29,30,31,32,33,34,35,36]. Of these, three studies performed stratified analysis based on liver metastases within ICI-based treatment groups [31, 35, 36]. An et al. reported that OS was significantly prolonged in patients without liver metastases who received ICI plus fruquintinib treatment [31]. Similarly, Zhao et al. found that patients without liver metastases had significantly longer median PFS (6.7 months vs 3.5 months, p < 0.0001) and median OS (15.8 months vs 10.6 months, p = 0.045) [36]. Additionally, in a study of 38 patients without liver metastases, those receiving ICI combination therapy had significantly longer median PFS compared to those in the non-ICI group (7.1 months vs 5.6 months, p = 0.034) [35].
Table 1 Characteristics of included studies (n = 11)Immune Checkpoint Inhibitor MonotherapyOnly one study evaluated the efficacy of ICI monotherapy versus chemotherapy in mCRC [26]. The first cohort included 49 patients with MSI-H tumors who received first-line ICIs, including pembrolizumab or nivolumab monotherapy, or a combination of ipilimumab and nivolumab. This group was compared to 89 patients who received standard 5-fluorouracil (5-FU)-based chemotherapy [26]. Among patients with MSI-H tumors, ICIs demonstrated significantly improved outcomes compared to chemotherapy. The median PFS was 24.87 months in the ICI group, significantly surpassing the 5.65 months observed in the chemotherapy group (p < 0.001) with a hazard ratio (HR) of 0.31 (95% confidence interval [CI]: 0.18–0.52). Similarly, the median OS was not reached in the ICI group, indicating a sustained survival benefit, compared to 24.1 months in the chemotherapy group (p = 0.02), with a HR of 0.45 (95%CI: 0.23–0.88) [26]. Notably, the second cohort, consisting of 83 patients with MSI-H mCRC and 99 patients with MSS mCRC receiving ICI monotherapy at any line of therapy, showed more favorable outcomes for MSI-H compared to MSS tumors. The median PFS was 12.19 months in the MSI-H group versus 2.46 months in MSS group (p < 0.001). The median OS was not reached in the MSI-H group, compared to 6.57 months in the MSS group (p < 0.001) [26].
Immune Checkpoint Inhibitor and Antineoplastic Agent CombinationNie et al. assessed the efficacy of ICIs combined with trifluridine/tipiracil (TAS- 102) against TAS- 102 monotherapy and TAS- 102 with bevacizumab [27]. The combination of ICIs and TAS- 102 (n = 10) did not improve clinical outcomes compared to TAS- 102 alone (n = 6). The median PFS was identical in both groups at 3.0 months (ICI plus TAS- 102 combination: 95% CI: 1.5–4.5 and TAS- 102 monotherapy: 95% CI: 2.2–3.8; p = 0.041) [27]. Similarly, the median OS was 6.0 months for the ICI + TAS- 102 combination therapy (95% CI: 1.7–10.3) and 6.5 months for TAS- 102 monotherapy (95% CI: 0.1–12.9; p = 0.013). However, the DCR was lower in the ICI plus TAS- 102 combination group (40%) compared to 50% with TAS- 102 monotherapy (p = 0.047). The safety profile for ICI plus TAS- 102 combination therapy was comparable to TAS- 102 monotherapy, with no significant increase in TAS- 102-related adverse events [27].
Immune Checkpoint Inhibitor and Tyrosine Kinase Inhibitor CombinationsA total of eight studies examined the efficacy of combining ICIs with tyrosine kinase inhibitors (TKIs) as the main treatment group for CRC, particularly in patients who had progressed after standard chemotherapy [28,29,30,31,32,33,34,35]. Regorafenib was the most commonly investigated TKI, featured in seven studies [28,29,30,31,32,33, 35]. While results were mixed, the overall findings suggested better efficacy outcomes with ICI-TKI combinations.
In a retrospective study by Wang et al., which included 209 mCRC patients, those receiving PD- 1 inhibitors plus regorafenib (n = 53) had a significantly longer median OS compared to those receiving regorafenib alone (n = 156) (13.5 vs. 10.1 months; p = 0.014) [28]. In a larger cohort study of 537 patients, the combination of ICI-regorafenib (n = 161) also resulted in a significantly longer median OS compared to regorafenib monotherapy (n = 376) (13.5 vs. 10.0 months; p = 0.001) [29]. However, the median PFS was 5.4 months for the ICI-regorafenib group, compared to 3.8 months for regorafenib monotherapy, with the difference not reaching statistical significance (p = 0.170) [29]. Similarly, Deng et al. found that patients treated with PD- 1 inhibitors plus regorafenib (n = 27) had a more prolonged median OS compared to regorafenib monotherapy (n = 23) (14.8 vs. 10.0 months; p = 0.045) [
Comments (0)