
Remember me
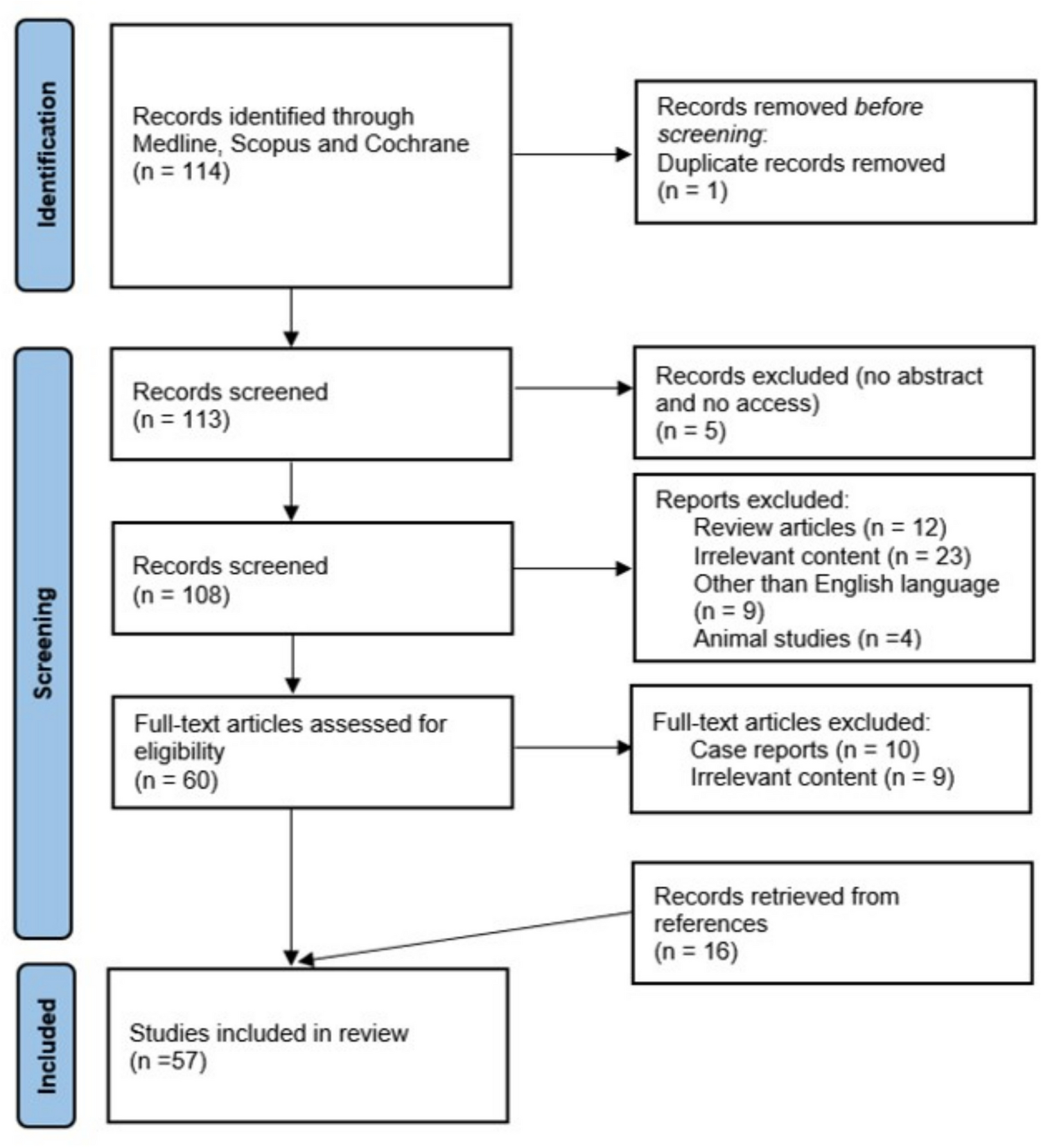

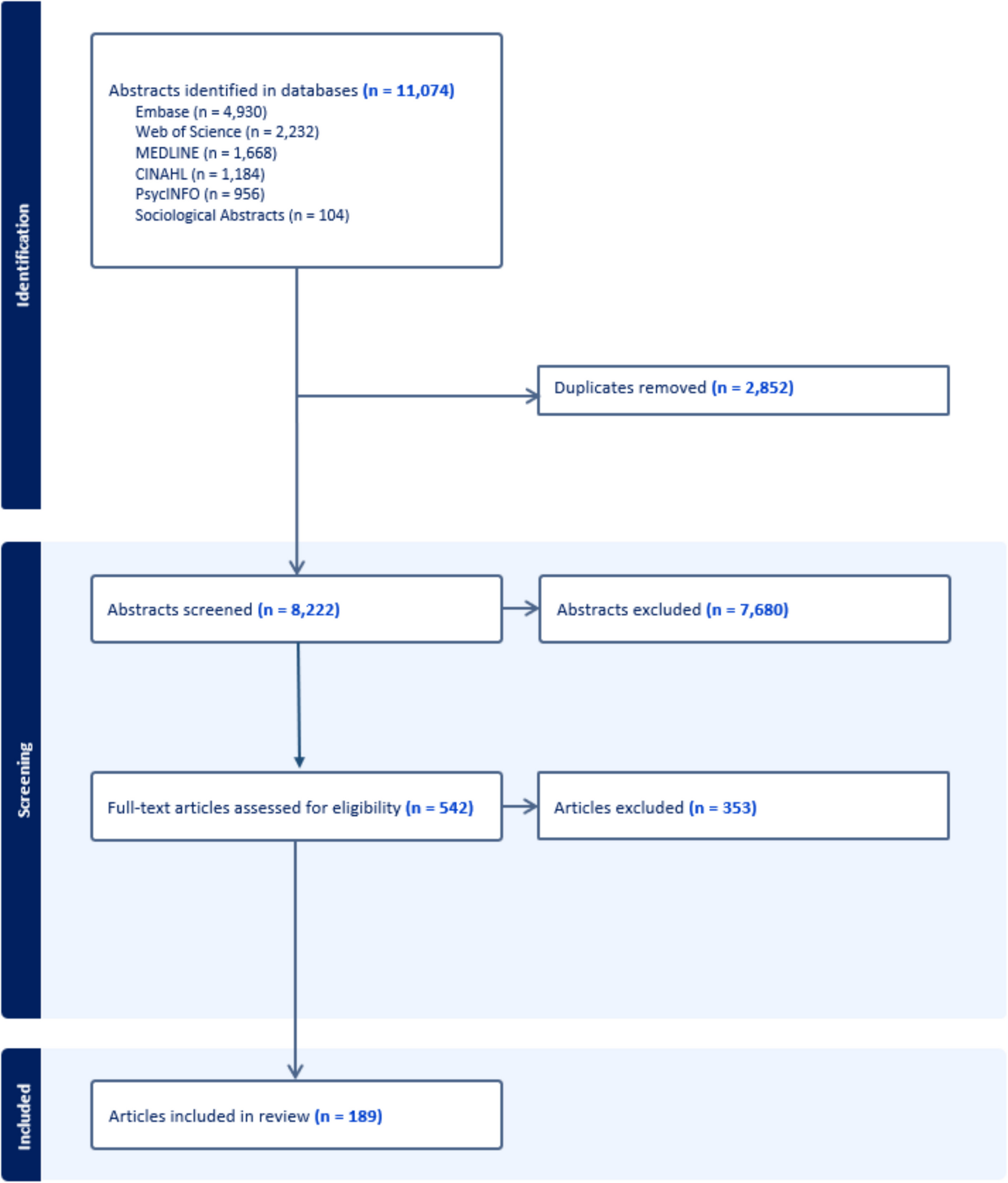
Figure 1 shows the selection flow chart of relevant studies. A total of 409 articles were retrieved, and 5 articles were finally selected for inclusion in the present review (study selection process is summarized in Fig. 1).
Summary of the Selected StudiesStudy and Population CharacteristicsThe systematic search included 5 studies (3 prospective non-randomized studies and 2 RCTs), with study selection flow chart in Fig. 1. The main characteristics of the studies included are summarized in Table 1. The study population only included MSM living with HIV.
Table 1 Summary of articles included in systematic reviewFig. 1
Systematic review flowchart
One randomized double-blind controlled trial [16] by Fox et al. compared imiquimod to placebo in treating intra-anal HSIL in 53 MSM living with HIV: 28 were assigned to active treatment and 25 to placebo. The imiquimod schedule consisted of 3 applications/week for 16 weeks and dosing was half a sachet intra-anally, to reduce potential systemic absorption and side effects. The CR rate was 14.3%; 29% had PR and in 57.1% the lesions persisted in the imiquimod arm, while the placebo arm showed only 4% CR and 96% of persistent lesions. After trial completion, partial responders, non-responders, and those in the placebo arm were offered an open-label treatment with imiquimod with the same schedule and dosing (21 patients in total, of whom 12 were originally from the placebo arm), resulting in a total of 23.8% CR and 19% PR rates. Thus, in total a sustained CR was observed in 61.7% (29/47 patients) over a mean duration of follow-up of 30 months. Two patients out of 53 developed ASCC (3.8%), one originally assigned to the placebo group after a few weeks into the treatment arm, which may be considered a prevalent case, in which the diagnosis was missed at study entry. The other one that progressed to ASCC was in the open label group, but no further information is available from the paper.
Wieland et al. published a prospective non randomized open-label pilot study that included 22 MSM living with HIV (18 perianal and 4 intra-anal AIN) compliant to therapy [17]. Out of the 22 patients, 64% (14) had histology-proven anal HSIL (11 perianal and 3 intra-anal). Imiquimod treatment consisted of self-applied 5% cream for perianal HSIL or suppositories for intra-anal HSIL 3 times a week for 16 weeks. After treatment, 78.6% (11/14) had a CR and 21.4% (3/14) had residual AIN- 1. After a mean 9.87 months of follow up after treatment, 10 maintained a CR, 1 recurred as HSIL, 2 recurred as LSIL, while 1 that had residual AIN at end of treatment had persistent LSIL. With respect to the 11 cases of only perianal HSIL, 81.8% (9/11) had a CR and 18.2% (2/11) had residual AIN 1 after treatment. After a mean of 11.1 months of follow up, 81.8% (9/11) maintained a CR, while 1 recurred as HSIL at 12 months and 1 as LSIL at 6 months.
An open-label RCT by Richel et al. compared imiquimod, topical 5-fluorouracil and electrocautery for the treatment of AIN in 156 MSM HIV + [18]. Anal HSIL was present in 57% of patients, while 43% had LSIL. 54 patients were randomly assigned to imiquimod, 48 to topical fluorouracil, and 46 to electrocautery. Imiquimod was administered three times weekly for 16 weeks (6.25 mg). For perianal HSIL, half a sachet was the standard dose, while in intra-anal HSIL the volume was increased by an indifferent cream and applied with a standard applicator. Regarding only anal HSIL, a CR was recorded in 21% (5/24 patients, per protocol analysis), a PR in 25% (6/24) and no response in 54% (13/24). Furthermore, response rates were higher for perianal HSIL than for intra-anal ones, and imiquimod showed superior outcomes compared to other treatments: a CR of 100% (9/9) for perianal HSIL and a 22% CR (9/41), 15% PR (6/41) and no response 63% (26/41) for intra-anal HSIL.
Van der Snoek et al. [19] included 44 anal HSIL in HIV + MSM, 15.9% with perianal HSIL in and 84.1% with intra-anal HSIL. Patients were instructed to apply imiquimod during five consecutive nights per week for 16 weeks (6.25 mg). For perianal HSIL, half a sachet was the standard dose, while in intra-anal HSIL the volume was increased by an indifferent cream and applied with a standard applicator. After 16 weeks of treatment, a CR of 20% and PR of 25% were recorded, with an overall response rate of 45%. Perianal lesions showed an overall response rate (RR) of 100% (71% CR and 29% PR), while intra-anal HSIL an overall RR of 35% (11% CR and 24% PR). An additional 16-weeks course of treatment was offered to another 20 partial responders and non-responders, which resulted in more responders (45%; 15% CR and 30% PR). Thus, after 32 weeks, an overall response rate of 66% was reported, 59% in intra-anal HSIL and 100% in perianal HSIL. After 12 months of follow-up, 3 patients (8%) experienced HSIL recurrence.
A prospective non-randomized open-label pilot trial enrolled 9 HIV + MSM with anal HSIL treated with imiquimod 3 times a week for 9 weeks. A CR of 33% was achieved and 7 out of 20 lesions in 9 participants (35%) downgraded from HSIL to LSIL [20]. No effects were observed in cytokine gene expression, HIV 1 DNA/RNA levels, or HPV load or types.
Type of RegimenThe frequency of application was 3 times weekly in almost all studies, following a schedule similar to that for condyloma [16, 17, 21, 22]. One study increased frequency of application to 5 times weekly, but apparently this did not lead to superior outcomes in terms of responses [19]. The treatment duration was 16 weeks [16, 17, 19, 21] in all but one study, in which it was of 9 weeks [22].
An additional 16-weeks treatment was offered to partial responders or non -responders in two studies, with an increase in the response rate [16, 19].
Type of TreatmentImiquimod was mainly self-applied in cream form for both intra-anal and perianal disease in most studies [16, 19, 21, 22].
In two studies, Wieland et al. and Van der Snoek et al. suppositories for intra-anal disease were used [17, 19].
The dosage of imiquimod was typically 6.25 mg per application (half-sachet) [16, 17, 19, 21] while one study [22] allowed the use of a whole sachet, but with a shorter treatment duration.
Side EffectsFox et al. reported that only one patient discontinued the treatment due to side effects (out of 28 in the imiquimod arm), but the specific type of side effect was not detailed [16].
In the RCT by Richel et al. side effects were reported by 91% of patients treated with imiquimod, with 9% of patients discontinuing treatment due to its severity [21]. Grade 1–2 side effects were reported by 47% of the patients and grade 3–4 by 43% (mainly pain, bleeding, itching, flu-like symptoms, and fatigue).
Cranston et al. documented 7 adverse events in 5 out of 9 participants: 4 cases of anal irritation, 1 of chills, 1 of fatigue, and 1 hemorrhoid flare [22].
Reported adverse events were erythema in all patients and further events in 11/22 compliant patients in Wieland’s paper [17]. Of these, 7 patients (32%) experienced mild erosions and 1 severe erosion (due to overdosage). Four patients (18%) had influenza-like symptoms within the 2 first weeks of therapy.
In the Van der Snoek et al. study adverse effects were present in 95.5% [19], with the most frequently reported being pain during defecation, burning sensations, mood swings, and fatigue, while flu-like symptoms were rarely observed (< 5%). Side effects did not differ between 3-days and 5-days schedules [19]
Comments (0)