The worldwide prevalence of XP is about 1:250,000 [2]. The disease usually develops at an early age, and the risk of developing melanoma and non-melanoma skin cancer increase by 2,000 and 10,000 times, respectively, compared with healthy individuals [3]. Basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) are the most common malignant tumor, others such as melanoma [4]. XP can be caused by nucleotide excision repair (NER) abnormalities caused by mutations in any of the eight genes (XPA-G and XPV). After continuous exposure to ultraviolet rays, XP patients may experience entropion or eversion of the eyelids, trichiasis and lower eyelid defects, conjunctival melanosis, corneal ulcers, cataract etc. [5]. Ocular malignancies can involved from the conjunctiva to the optic nerve, among which ocular surface squamous neoplasia (OSSN) is most common in the palpebral fissure area [2], such as conjunctiva squamous cell carcinoma [6]. We now present a case of XP with a progressive enlargement of the ocular surface neoplasm, genetic examination, and personalized treatment of the ocular surface mass.
The gene mutation site detected in this patient, XPC: c.1677 C > G has been included in the ClinVar database, but XPC: c.155 C > G has not been included in the ClinVar database, and no relevant literature reports have been found. The XPC gene is located in the 3p25 region of chromosome, contains a total of 16 exons, and encodes a protein consisting of 940 amino acids, accounting for about 25% of XP. The phenotypes of patients vary degrees of severity [7]. In addition to its role in NER, XPC is involved in several other DNA repair pathways or cellular mechanisms that also play a role in regulating cellular homeostasis. Therefore, the XPC gene plays an important role in tumorigenesis. In addition to the DNA damage phenotype induced by UVB, other tumorigenic pathways mediated by XPC also show a tendency to tumorigenesis in non-light-exposed areas [8].
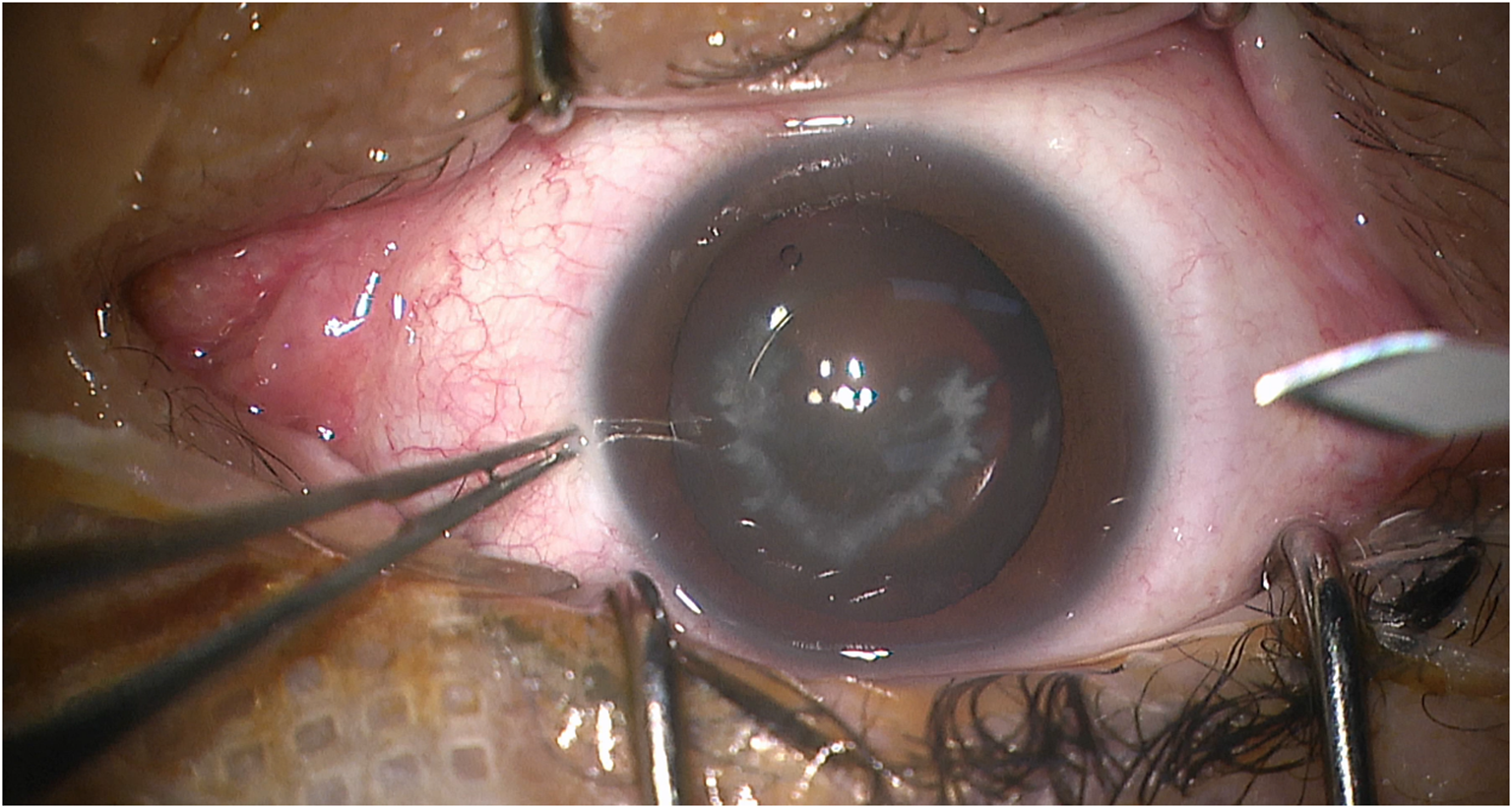
Ocular manifestations are one of the main early features of XP, which can occur in 40 ~ 80% of XP patients [9], and ocular surface cancer accounts for 2% of all XP cases with ocular manifestations [10]. The patient had ocular manifestations of XP, such as massive pigmentation foci on the eyelid skin and bulbar conjunctival pigmentation. The pathological result of corneoscleral hyperplasia in this patient was mixed hemangioma. XP combined with ocular surface hemangioma was rarely reported. Early skin lesions in XP patients include telangiectasia and atrophy, hyperpigmentation and hypopigmentation, so it is considered that the ocular surface mixed hemangioma in this patient is the manifestation of XP skin lesions on the ocular surface.
In this case, the intrastromal lenticule obtained from small-incision lenticule extraction was used as the donor graft for lamellar keratoplasty to repair the postoperative keratoscleral defect, which not only restored the integrity of the ocular surface, but also met the demand for corneal transplantation under the condition of donor scarcity [11]. Anti-VEGF drugs are a new option for the treatment of ocular surface neovascular diseases [12]. In order to reduce surgical bleeding and inhibit postoperative angiogenesis, anti-VEGF drugs (such as Compaplcept) are injected into the subconjunctiva before and after surgery, with the purpose of reducing intraoperative bleeding and inhibiting postoperative neovascularization of the sclera [13]. In this case, the graft healed well, the scleral blood vessels were slightly dilated after the operation, astigmatism did not increased significantly compared to preoperative levels, and postoperative visual acuity remained normal.







Comments (0)