Based on clinical evidence, multifocal IOLs (MIOLs) should be used cautiously in patients with prior corneal refractive surgery (e.g., PRK). However, in this case, the patient demonstrated favorable ocular characteristics for MIOL implantation, including regular central 4 mm corneal morphology, minimal astigmatism (< 1.00D), and low HOAs. These parameters fell within acceptable thresholds for MIOL use, prompting selection of the Tecnis Symfony ZXR00 IOL (Johnson & Johnson, USA).
The ZXR00 incorporates a proprietary echelette diffractive grating and chromatic aberration correction technology, providing extended depth of focus while neutralizing corneal spherical aberration. Clinical studies report reduced incidence of photic phenomena (glare/halos) compared to conventional MIOLs [13,14,15]. Notably, ZXR00 demonstrates superior contrast sensitivity, particularly at low spatial frequencies, versus the AT LISA tri 839MP (Carl Zeiss) in myopic patients [16]. Its optimized optical profile delivers excellent distance and intermediate vision with a smooth defocus curve. Similar to cataract patients without a history of refractive surgery, patients with a history of such surgeries, including PRK, can achieve ≥ 20/25 UDVA postoperatively, and similar subjective visual function scores [17]. Given this patient’s occupational requirement for prolonged digital device use, we targeted a myopic residual refraction (-0.50D to -0.75D) to optimize intermediate/near vision while maintaining satisfactory distance acuity, achieving personalized visual rehabilitation.
The Barrett True-K formula represents an advancement over the Barrett Universal II formula, specifically designed to address corneal power estimation in post-refractive surgery eyes while providing reliable IOL power predictions across varying axial lengths [13, 17,18,19,20,21,22,23]. Nevertheless, cataract surgery in post-refractive patients remains significantly more complex than in virgin eyes, with greater variability in postoperative outcomes [24,25,26,27]. In patients with a history of refractive surgery, the altered corneal curvature—particularly significant changes in the central corneal curvature—may lead to inaccuracies in biometry even with advanced biometric measurement devices. Moreover, applying the standardized corneal refractive index of 1.3375 to calculate IOL power in these patients may result in erroneous estimation of the effective lens position (ELP), leading to IOL power calculation errors [25]. In our clinical context, postoperative residual refractive error (defined as > ± 0.5D deviation from target spherical equivalent) most frequently manifests as compound myopic astigmatism (35.5%) or simple myopia (33.3%) [28, 29]. Despite this refractive discrepancy, the patient in this case achieved excellent functional vision at intermediate and near distances, fulfilling their primary visual demands and resulting in high satisfaction. This outcome emphasizes that while precise refractive targeting remains challenging in post-refractive cases, optimal visual quality can still be attained through careful IOL selection and management of patient expectations.
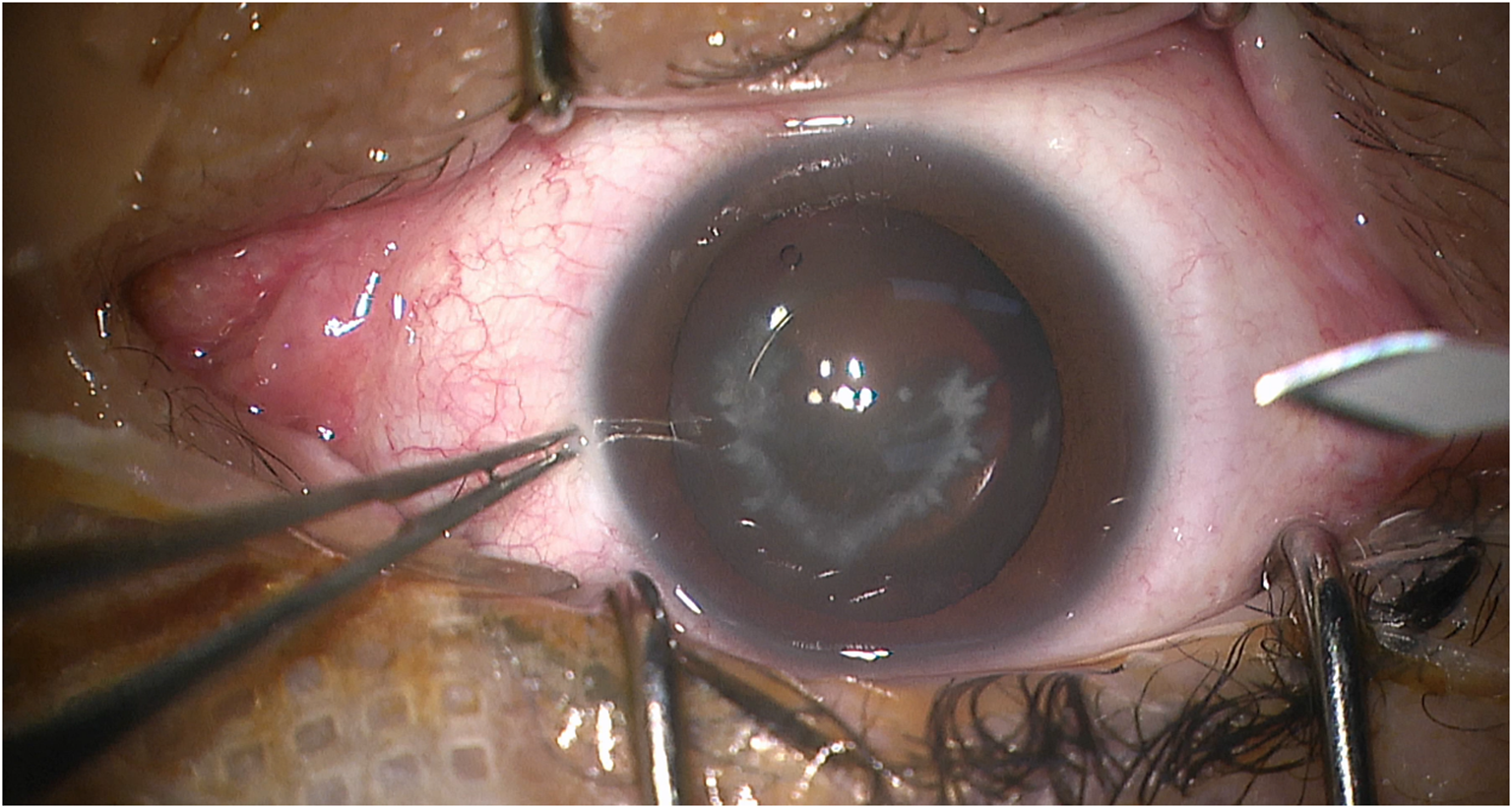
Regarding the surgical procedure itself, the surgeon should strive to be extremely gentle during the process of removing the ICL to avoid damaging the corneal endothelium, zonules, and lens. From the perspective of our past experiences, for cataract patients with high myopia similar to the case, the size of the capsulorhexis is crucial because of fragile zonules. When implanting the IOL, it is vital to ensure that IOL is correctly placed in the capsular bag, minimizing the risk of IOL decentration or tilt. During postoperative follow-ups, the surgeon should closely monitor the position of the IOL and promptly identify and address any abnormalities, as this is important for the long-term success of the surgery. Additionally, one easily overlooked point is that surgeons should thoroughly understand the indications and suitable candidates for multifocal intraocular lenses. Meanwhile, delving into patient’s personality, occupation, and visual expectations is also important. During preoperative discussions, surgeons should inform patients comprehensively about the characteristics of multifocal IOLs, potential postoperative outcomes, and possible complications, helping patients realize the potential gap between actual results and their ideal expectations.
Although the visual outcomes in this case were largely positive, long-term potential risks—such as intraocular lens (IOL) decentration and tilt—still require further follow-up observation. Additionally, individual variations inherent in single-case studies may introduce bias, further studies are warranted to validate these findings in larger cohorts.
In conclusion, we cautiously recommend that, for patients express a strong desire for spectacle independence or have specific occupational needs, and their preoperative biometric measurements meet the indications for MIOLs, the use of TECNIS Symfony ZXR00 IOL, along with adjustments to the residual refractive power, may result in excellent visual outcomes, ensuring good visual quality and satisfaction.







Comments (0)