
Remember me



The present study is a pre-postintervention study utilizing an interrupted time series analysis of observational data. This study received an exemption from ethical approval by the ethics review board of Leiden University Medical Center (nWMODIV2_2024009).
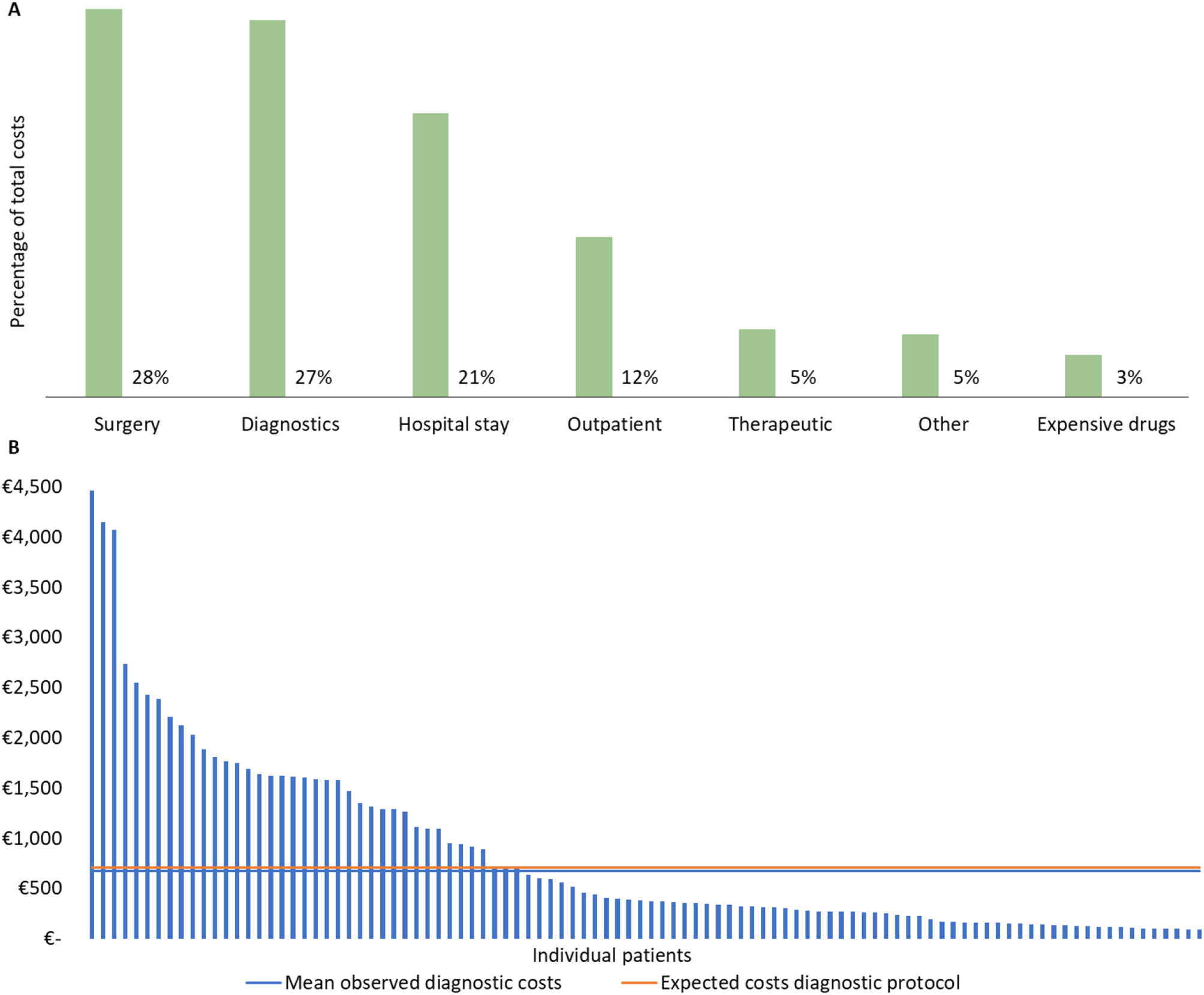
ContextThe VBHC care pathway for thyroid cancer is multidisciplinary and provides preoperative analysis, surgery, postoperative treatment, radioactive iodine treatment, and follow-up care. Since 2017, the pathway has been part of a VBHC implementation program, working with a core VBHC team of medical specialists, improvement coaches, financial advisors, researchers, and IT specialists. This team developed a dashboard displaying outcomes and costs to guide continuous improvement of care delivery in plan-do-check-act cycles. Cost data revealed diagnostics was one of the major cost drivers within the care pathway (Fig. 1A). A benchmark of the costs of the expected diagnostic costs (according to the care pathway’s diagnostic workup) and the observed costs showed a high variation of diagnostic use among individual patients (Fig. 1B). A significant proportion of patients underwent one or more repeat FNA due to non-diagnostic results (classification Bethesda I) and there was a high utilization of molecular diagnostics. These findings resulted in the consequent improvement project targeting needle selection in FNA.
Fig. 1
(A) Share of total costs for major cost categories, and (B) benchmark of observed versus expected diagnostic costs and variation of costs across individual patients
InterventionIn the preintervention period, sonographers used a conventional syringe needle (21G) to perform FNA per standard practice. This was changed to a Modified Menghini-type needle (Biomol, 20G) needle containing a mandrel in the postintervention period. Using a Modified Menghini-type needle needle, a thyroid nodule is punctured when the mandrel is inside the nodule. The mandrel is then retracted, creating a vacuum and allowing the sonographer to move the needle through the entire nodule with an ‘apple coring’ motion before withdrawing. The advantage of this needle to a conventional syringe needle is that it prevents contamination of the derived material by blood and tissue that is in between the skin and thyroid nodule and more cells can be sampled. Before implementation, sonographers received training in the use of the Modified Menghini-type needle needle from an expert radiologist. After completing the training and practicing on a phantom, the Modified Menghini-type needle needle was adopted by the sonographers in October 2021. The only change in the entire diagnostic workup was the needle; smear technique and other methods remained unchanged. The samples obtained both pre- and postintervention were considered cytological material and fixed by buffered formalin and embedding in paraffin.
Participants and data sourcesPatients were included if they presented with a thyroid nodule at the care pathway between July 2020 and May 2022, were 18 years or older, and underwent FNA performed by a specialized sonographer. Patients were excluded if FNA was performed on thyroid tissue with no discernable nodule or if FNA was performed by a radiologist (in training). Data was retrospectively collected from radiology and pathology reports and financial administration of the institue. The financial administration registers health care utilization at the individual patient level by coupling care activities, including their date, to costs. These costs are derived using activity-based costing (ABC). ABC allocates direct and indirect costs based on distinguishable care activities [12].
FNA characteristics and outcomesOutcomes collected for each FNA included TI-RADS classification [13], composition and maximum size of the nodus (in mm), number of attempts, number of nodules, sonographer performing the FNA from radiology reports, and Bethesda I-VI classification from pathology reports according to the 2017 Bethesda System for Reporting Thyroid Cytopathology [11]. The TI-RADS categories were: (1) normal thyroid tissue, (2) benign lesion, 3), probably benign lesion; 4) suspicious potential malignant lesion, 5), probable malignant lesion. The Bethesda classifications were: (I) nondiagnostic; (II) benign; (III) atypia of undetermined significance; (IV) follicular neoplasm; (V) suspicious for malignancy; and (VI) malignant.
Health care utilizationHealth care utilization data in the first patient year following FNA was collected, including diagnostics, treatment, and follow-up within the care pathway. Diagnostics were divided into an initial diagnostic workup– which included simultaneous FNA, lab tests, ultrasound of the neck, and potentially needle biopsy and histology– and follow-up diagnostics in case of cancer or a nondiagnostic outcome (Bethesda 1). Follow-up diagnostics consisted of additional diagnostic workup, pathology, and/or imaging. Costs were updated to 2024€ with the health care sector-specific consumer price index provided by the Dutch Bureau for Statistics [14]. Health care utilization data was coupled to radiology reports on the patient level. A random sample of 15% of financial data was reviewed to crosscheck whether FNA was registered as a care activity and on the same date as FNA was registered in the radiology reports. Patients with no FNA registered in the financial data were excluded from the analysis of health care utilization. In the healthcare utilization analysis, patients who underwent FNA in both the preintervention and postintervention period were only included in the preintervention group.
The unit cost of FNA in the preintervention period was derived from the ABC model of the hospital. The postintervention unit cost of FNA was estimated under the assumption that FNA costs consist of the costs for the needle(s), plus other costs proportional to the duration of the procedure: first, the cost of a syringe needle (€0.99) was subtracted from the total preintervention FNA unit cost, which was then divided by the duration of an FNA appointment (30 min.) to estimate the FNA unit cost per minute. This FNA unit cost per minute was multiplied by the duration of an FNA appointment postintervention. This duration was estimated as the duration of one FNA appointment (30 min.) minus the difference in the number of puncture attempts pre-postintervention*2.5 min (the estimated average duration of an additional puncture attempt). Then, the current cost of a Modified Menghini-type needle needle (€22) was added to the unit cost.
Statistical analysisFNA characteristics and Bethesda classifications were analyzed at the level of FNA, and health care utilization was analyzed at the patient level. We first used descriptive statistics and univariate analyses to describe preintervention and postintervention differences. Continuous variables were described as means with standard deviations and analyzed by the independent sample’s t-test for (un)equal variance. Categorical variables were described as proportions and analyzed by Fisher’s exact test due to the small expected cell count for some variables. The primary outcomes of Bethesda I classification (nondiagnostic) and health care utilization were assessed over time using interrupted time series (ITS) analysis. All ITS models consisted of three model terms: (1) a linear trend over time (in months), (2) a change in level between the preintervention and postintervention period, and (3) a change in linear trend over time (in months) between the preintervention and postintervention period. We used generalized linear models of a binomial family with a logit link function for Bethesda I classification as binary outcome, and a Gaussian family with identity link function for health care utilization in 2024€ as continuous outcome. The analysis of Bethesda I classification was additionally adjusted for sonographer ID using four dummy variables. For all statistical analyses, a p-value below 0.05 was considered statistically significant. Statistical analyses were performed with R studio (version 4.3.1).
Comments (0)