The incidence of POP is influenced by various factors, including the type of surgery, the patient’s baseline health status, and nosocomial infection control measures [14, 15]. Given the absence of a uniform diagnostic standard, reported incidences of POP significantly vary across hospitals, with overall incidences ranging from 0.9 to 1.6%. However, certain studies indicate incidences as high as 15.8%, with postoperative bacterial pneumonia incidence at 21.6%, trailing only behind postoperative incision and urinary tract infections. In China, postoperative bacterial pneumonia was 21.6%, second only to postoperative incisional infections and urinary tract infections. The incidence of surgical POP significantly varies by site; however, major thoracic and upper abdominal surgeries tend to impair respiratory muscles, leading to a notably higher incidence of POP compared to other sites [16]. Regarding cardiac surgery, the incidence of POP also demonstrates variability, with previous literature reporting a range from as low as 2.1% to as high as 24.2% [17, 18]. The incidence of POP after cardiac surgery at our institution remained around 5% for three consecutive years, exhibiting a significant downward trend in 2023 and presenting as comparatively low against other relevant reports. This outcome can be attributed to the medical team’s efficient collaboration, stringent medical procedures, and ongoing quality improvement initiatives.
Although the incidence of pneumonia post-cardiac surgery remains relatively low, it’s crucial to recognize that, despite its infrequency, the severe complications that can ensue from pneumonia significantly impact patient recovery and long-term prognosis. Figure 5 illustrates that patients with POP experienced substantially longer hospital stays, intensive care unit (ICU) stays, and antimicrobial usage than the non-infected group. To identify lung infections early and implement timely interventions, this study evaluated the postoperative dynamics of infectious markers like PCT and their clinical diagnostic utility for POP. As shown in Table 2, key factors potentially affecting the study outcomes, including smoking history, surgery type, and comorbidities, were excluded. Preoperative nutritional status is a significant, influential factor [19]. This study incorporated the CONUT score, a less frequently addressed indicator in previous research on risk factors for postoperative cardiac infections. Previous studies primarily utilized nutritional indices like BMI, ALB, TLC, etc. Compared to a single laboratory marker, a composite marker offers a more comprehensive assessment of patients’ nutritional status [9]. However, this study found no significant difference in preoperative dietary status between the two groups.
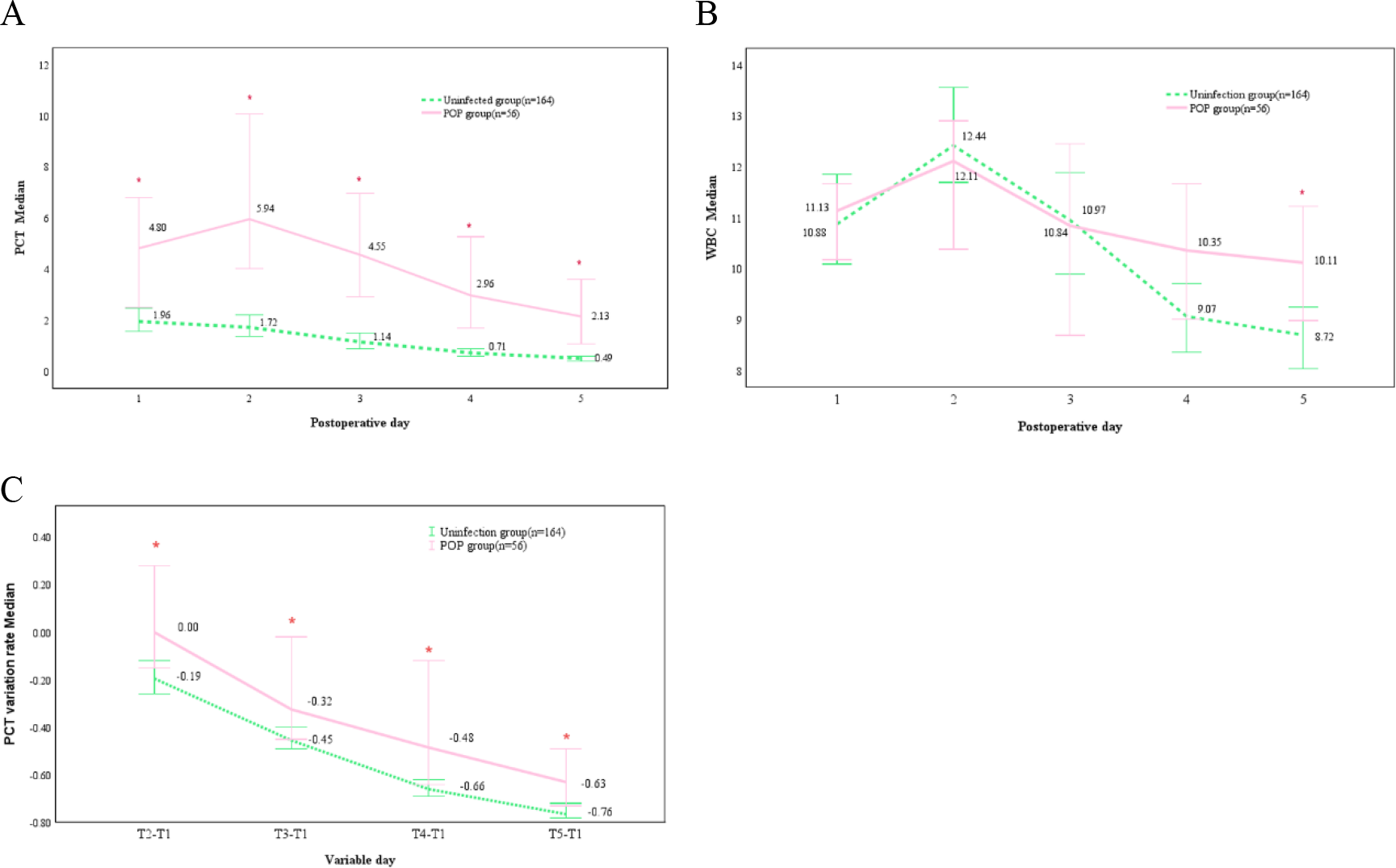
PCT, a peptide precursor synthesized by thyroid C-cells, is increasingly utilized to assess the risk of systemic infection or sepsis. Recently, its application in medicine has expanded, particularly in predicting post-surgical infections, gaining considerable attention. PCT’s utility in predicting postoperative infections across various surgical disciplines—including organ transplantation [20], orthopedic [21], abdominal [22], neuro [23], and gynecological surgery [24]—has been well-documented. Interpreting calcitonin levels alongside other clinical indicators and assessing the patient’s overall condition aids in identifying high-risk patients. This study systematically assessed the patterns of calcitonin gene changes following extracorporeal cardiac surgery in adults to evaluate its diagnostic value in early pneumonia detection. Results indicated significantly higher calcitoninogen levels in patients with early POP, underscoring its potential as a diagnostic biomarker for early pneumonia. ROC curve analysis revealed that PCT exhibited the highest diagnostic accuracy among the studied parameters, making it an optimal indicator for the early diagnosis of lung infection post-cardiac surgery. Our study offers more detailed insights into calcitoninogen dynamics compared to existing research. In-depth analysis revealed that PCT levels peaked on the second postoperative day, with concentrations in the infected group significantly surpassing those in the control group at all measured time points. Additionally, WBC counts peaked on the second day, yet notable differences were observed on the fifth day among infected patients. Crucially, the rate of PCT variation was markedly higher in the infected group, further illustrating the significant impact of infection on PCT fluctuations. These observations offer vital insights for refining postoperative management and infection control protocols. Furthermore, our study incorporated leukocyte and PCT variability rates to prevent the over-interpretation of fluctuations in individual biomarkers. A study encompassing 423 patients who underwent cardiac surgery with CPB assessed the predictive value of combining CRP, WBC, and PCT levels for postoperative infections. It confirmed that the combined assessment of PCT and leukocyte levels during the initial three postoperative days accurately predicted infections up to 30 days following cardiac surgery, providing a robust tool for early detection and management of potential post-surgical infections [25].
In the multivariate analysis, the PCT level on day 2 post-surgery, WBC count on day 5 post-surgery, PCT variability on day 4, and the duration of mechanical ventilation were included. Notably, the duration of mechanical ventilation has been identified as an independent risk factor for POP in a range of surgical procedures, extending beyond cardiac surgery. This underscores the significance of monitoring mechanical ventilation duration alongside PCT levels and WBC counts as part of a comprehensive approach to assessing the risk of POP [7, 26]; this study demonstrated that the PCT concentration in patients within the infection group peaked in the second postoperative day, subsequently decreasing but remaining elevated above the standard threshold (> 0.5 ng/ml) on the fifth postoperative day. In contrast, the PCT concentration in the non-infection group continued to decline, falling within the normal range (< 0.5 ng/ml) by the fifth day. A significant difference in PCT concentrations was observed between infected and non-infected patients throughout the postoperative period. These findings align with previous research on adults [7]; however, studies involving pediatric patients have indicated no statistically significant difference in PCT concentration between infected and non-infected groups within the first three days post-surgery. Furthermore, PCT concentrations in both patient groups continue to decrease from the second day after surgery [27]. Considering the kinetics of PCT response to bacterial infections, possible explanations include: (1) a delayed response to infection, where PCT levels typically rise in response to systemic bacterial infections, making postoperative day 2 a more predictive marker for POP. This implies that a postoperative infection might require time to trigger a systemic response significant enough to manifest in PCT levels. This delay can be attributed to the time needed for the infection to establish itself and for the body to mount a systemic inflammatory response. (2) Specificity of PCT for bacterial infections: PCT shows heightened sensitivity to bacterial infections over other types, such as viral infections. Given that POP is predominantly bacterial, an elevated PCT level on postoperative day 2 is a specific marker for bacterial pneumonia. This specificity renders PCT an invaluable biomarker for the early detection of bacterial infections. (3) Surgical stress response: Surgery initiates an inflammatory response influencing the levels of various biomarkers, PCT included. However, the initial increase in inflammatory markers post-surgery may more likely reflect surgical stress than infection. By day 2, distinguishing between surgical and infection-induced inflammation may become more apparent, rendering PCT a more reliable infection marker [28]. ROC curve analysis results indicated that the PCT threshold on the second postoperative day was 3.45 ng/ml, suggesting clinicians may need to perform early diagnostic assessments. This threshold is notably higher than those reported in previous studies. For instance, a meta-analysis published in The Lancet Infectious Diseases identified a median cutoff value of PCT as a marker for diagnosing sepsis at 1.1 ng/mL [29]. Furthermore, the expert consensus on the clinical application of PCT in emergency care, published in China in 2012, offers detailed recommendations for PCT monitoring in common infectious diseases. It specifies that the threshold level for PCT to diagnose sepsis is > 0.5 ng/ml, the optimal threshold for diagnosing endocarditis is 2–3 ng/mL, and the median PCT level for bacterial infection is 1.84 ng/mL. A PCT cutoff value of 0.25 ng/mL is a critical indicator for initiating and discontinuing antibiotic therapy for lower respiratory tract infections [30]. A meta-analysis conducted in 2024, focusing on diagnosing adult cardiac postoperative infections, included 2,984 patients. The findings indicated that PCT is effective in ruling out uncertain infections. The analysis established an optimal threshold of 3 ng/ml, with the relevant time point as the second postoperative day (POD2) [31]. In conclusion, the significant predictive value of PCT levels on postoperative day 2 for POP underscores the importance of understanding the body’s temporal response to surgery and infection, enabling timely and appropriate clinical interventions. Furthermore, the leukocyte count on postoperative day 5 emerged as an independent risk factor for POP, a discovery potentially linked to our study’s inclusion criteria. Specifically, our study’s case group comprised only patients who developed pneumonia within the first 7 days following surgery. Within this group, leukocyte counts peaked by postoperative day 5, leading to generally higher leukocyte counts in the infected versus noninfected groups. This contrasts with prior studies where leukocytes were seldom considered an independent predictor of postoperative infection [32].
Another key finding of this study is that the diagnostic value of the absolute PCT level surpasses that of PCT variability and WBC count, diverging from the conclusions of prior research.PCT variability reflects the dynamic infection process and condition changes, with studies indicating that patients with postoperative infections typically exhibit higher PCT variability, marking a significant distinction from non-infected patients. Thus, PCT variability emerges as a crucial diagnostic marker for postoperative infection, potentially surpassing the absolute PCT level in diagnostic efficacy [7]. However, there remains no definitive conclusion regarding the superior diagnostic value of either metric. Additionally, this study reveals that calculating the PCT variation rate is complex, necessitating continuous PCT level monitoring and change rate calculation, thereby somewhat limiting its clinical utility. Conversely, the absolute PCT level provides rapidity, simplicity, and ease of operation, facilitating widespread clinical application. Regarding clinical applicability, we also plan to collaborate with the information department to integrate this early warning model with hospital information systems. Before clinical deployment, we must conduct rigorous multi-stage verification. We will initially examine various patient populations by utilizing a multicenter dataset encompassing diverse demographics and surgical protocols to assess the model’s robustness. This will be succeeded by prospective clinical testing in a realistic environment, where we will quantify sensitivity and specific indicators while monitoring workflow integration parameters, including real-life scenario indicators such as alarm fatigue and decision time. Additionally, it is crucial to conduct focus group interviews to evaluate clinician acceptance. Optimization based on a people-centered iterative system can enhance clinical practicality while preserving clinician autonomy.
However, this study has several limitations. Firstly, as a single-center retrospective study, the results might be influenced by specific surgical techniques and management strategies, thereby somewhat limiting their generalizability and necessitating further validation in broader clinical settings. Secondly, the analysis excluded some risk factors potentially associated with developing POP, such as disease severity. Thirdly, the study’s observed outcome was the incidence of pneumonia within 7 days postoperatively, whereas the typical diagnostic window for POP extends to 30 days post-surgery. This lack of follow-up to 30 days could introduce bias in classifying some cases as non-infected. Finally, due to the impact of medical insurance cost control policies, the dynamic monitoring of C-reactive protein (CRP) and interleukin-6 is not routinely conducted in clinical practice. In the future, we plan to consider the inclusion of cost-effective indicators such as the neutrophil/lymphocyte ratio (NLR), platelet/lymphocyte ratio (PLR) [33], and mid-regional pro-adrenomedullin [34] from a cost-effectiveness perspective. We will investigate the value of utilizing multiple indicators for combined diagnosis to enhance the sensitivity and specificity of POP diagnosis. Furthermore, the differing kinetics of these biomarkers can be leveraged to monitor treatment efficacy, thereby providing a more refined approach to managing postoperative infections.



Comments (0)