Our study aimed to investigate the correlation between WWI and FH among the US population. In this cross-sectional study involving 3698 adults, we found a nonlinear positive correlation between WWI and FH incidence rates, indicating that individuals with higher levels of WWI are more likely to have FH, and this relationship remained stable in fully adjusted models. In subgroup analyses and interaction tests, consistency in the relationship between WWI and FH was observed across gender, race, hypertension, and diabetes statuses. However, there was a significant association between WWI and FH among populations with a personal history of early ASCVD and a family history of early ASCVD.
BMI is associated with the prevalence of FH
Some studies indicate a certain correlation between BMI and FH incidence rates. A Greek study [16] on 1655 FH adults found that 68.4% of patients had BMI levels exceeding normal values, and the occurrence rate of ASCVD risk factors gradually increased with increasing BMI. Additionally, another study [17] on FH children showed that BMI was a promoting factor for changes in lipid parameters in FH children, and a significant increase in LDL-C levels was a hallmark of FH.
WWI more accurately predicts FH than BMI
Although these pieces of evidence suggest an association between traditional obesity indicators and FH, the obesity paradox still exists [18]. The potential reasons for the debate may partly be attributed to the limitations of traditional indicators, which cannot differentiate between fat mass and muscle mass. WWI is a new obesity indicator that combines the benefits of WC while attenuating the association with BMI, accurately indicating central obesity and can be used to assess fat and muscle mass [9]. Therefore, WWI can serve as a more comprehensive and accurate obesity measurement method, which may more accurately demonstrate the correlation between obesity and FH. In recent studies [7], WWI has been found to be the strongest predictor of cardiovascular disease mortality, surpassing BMI and WC. This is similar to our research findings, where we also believe WWI may be an effective predictor of FH. Unlike BMI, which only focuses on weight and height relationships, WWI also considers waist circumference, aiding in capturing the risk of central obesity. With its simple calculation and powerful predictive ability for disease development, WWI holds great promise as a potential anthropometry measurement indicator.
Correlation between WWI and cardiovascular disease
To our knowledge, with previous research mainly focusing on the correlation between WWI and cardiovascular disease. Ding [19] et al. conducted a prospective study on 12,447 Chinese individuals and found a significant correlation between higher levels of WWI and increased risk of all-cause mortality and cardiovascular mortality. Zhang [20] et al. found that WWI may be an independent predictor of heart failure in a cross-sectional study of 25,509 individuals. Fang’s research [21] showed a positive linear correlation between WWI and CVD, with greater significance in the under-50 age group. Previous domestic research has shown that 44.2% of FH patients suffer from cardiovascular disease, with early-onset ASCVD being one of the main clinical manifestations of FH, and male FH patients experiencing ASCVD before the age of 50, while female onset age is slightly later than males [22].
Correlation between WWI and FH
Similarly, our study is the first to investigate the correlation between WWI and probable prevalence of FH, found a nonlinear positive correlation between WWI and FH, consistent with the adverse consequences of WWI on cardiovascular health described in previous studies. This indicates that WWI may be an intervention indicator for reducing the risk of cardiovascular disease in the general adult population and a potentially effective factor screening for FH, emphasizing the importance of WWI in FH diagnosis and treatment.
Potential mechanisms between WWI and FH
Some potential mechanisms may explain the correlation between WWI and FH. FH is a genetically related hereditary disease, typically resulting from mutations or deletions in the LDLR gene, leading to defective synthesis, assembly, transport, and recycling of LDLR [23]. LDLR is a transmembrane glycoprotein widely distributed in various tissues of the body, with the highest expression in the liver, primarily involved in the metabolism of LDL [24]. The most common molecular alterations in the LDLR gene are small nucleotide variations present throughout the gene, mainly divided into spontaneous and induced mutations, with causes of induced mutations including radiation, chemicals, chronic inflammation, and oxidative stress. Firstly, the marker of abdominal obesity (WWI) has a greater impact on inflammatory markers than the marker of overall obesity (BMI) [25]. Caloric overload induces dysfunction of adipose tissue, promoting the production and release of various pro-inflammatory cytokines. The chronic inflammatory state resulting from the sustained presence of these cytokines may lead to many secondary consequences associated with increased risk of diseases, including an increased mutation rate in genes [26]. Secondly, central obesity can increase the oxidative stress response of individuals, and the adipose tissue will release more reactive oxygen species (ROS), an important deoxyribonucleic acid (DNA) damaging agent [27]. When ROS production exceeds the ability of cells to metabolize them, it leads to an excessive accumulation of ROS, which in turn disrupts cellular defenses, a process that regulates the genetic and epigenetic cascades of altered gene expression in humans [28]. In addition, while the oxidative stress response leads to DNA damage, DNA damage will induce the occurrence of inflammatory response, which then exacerbates the range of DNA damage, forming a vicious circle [29], and the oxidative stress and lipid peroxidation (LPO) accompanying infection and chronic inflammation may induce a variety of genetic diseases [30]. Finally, other coexisting disease states associated with obesity are also promoting factors for FH.
Superiority of the study
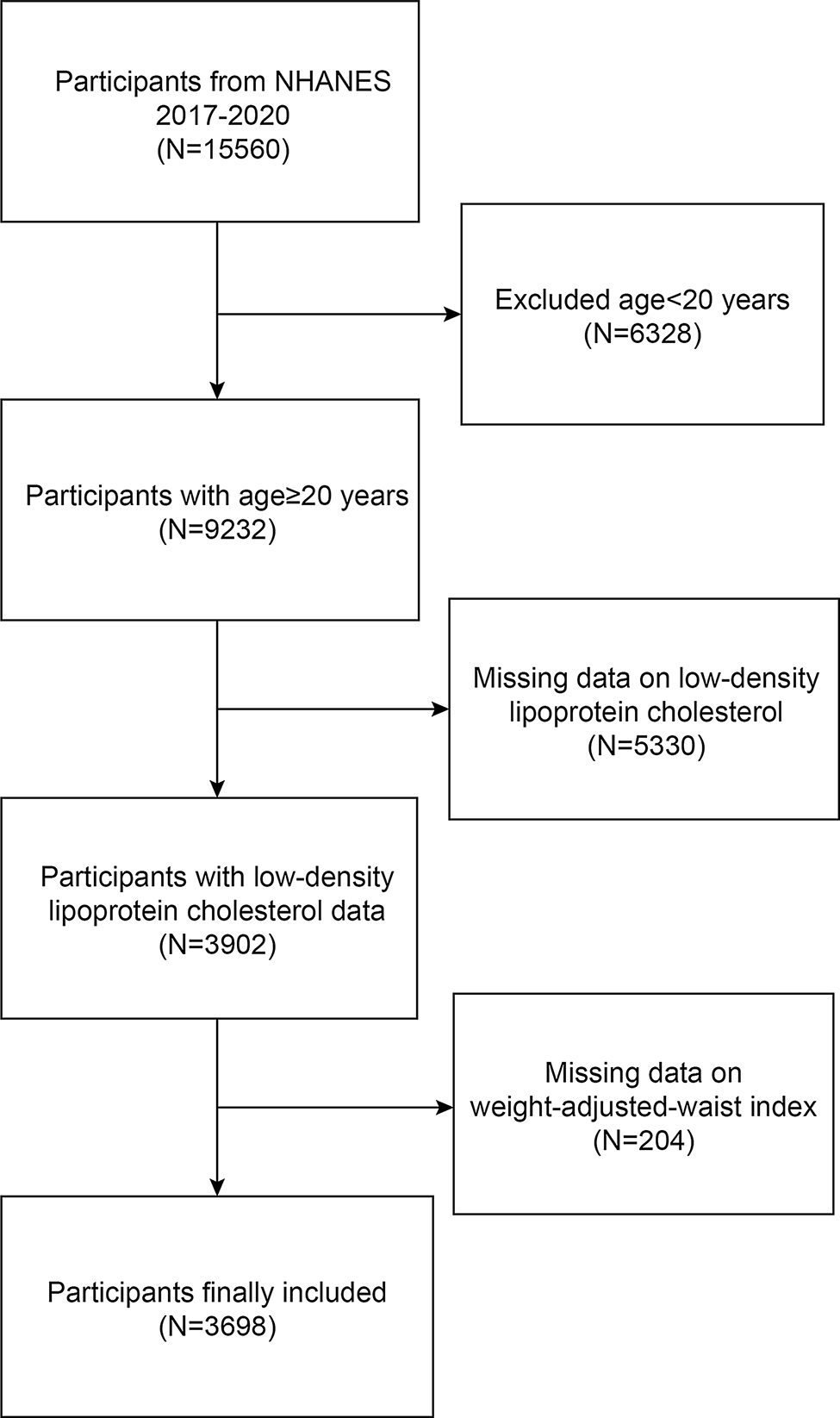
Compared with previous studies in this field, for example, studies in Europe [31], Japan [32], China [33] and other regions, there are some differences in the conclusions we may obtain. However, the strength of this study is that it was first collected using a stratified multistage probability sampling strategy based on NHANES data, thus improving the reliability and representability of our findings. Second, we used new data from 2017 to 2020, and the novelty of the data can be guaranteed. In addition, we used a new approach to obesity assessment that allowed us to make more accurate predictions of obesity-related risks. Finally, in our analysis method, we used a multivariate logistic regression model (logistic) adjusting for a range of relevant covariates to assess the impact of WWI on FH.
Limitations of the study
Nevertheless, this study has limitations, due to the relatively small number of FH patients, the results should be considered preliminary, and future research may benefit from increased sample sizes. Additionally, the study population primarily focused on adults, and whether similar conclusions can be drawn for adolescents remains uncertain. Despite adjusting our statistical models for most confounding factors, residual bias cannot be entirely ruled out. We acknowledge that our selection of patients did not involve explicit genetic diagnosis, potentially leading to the inclusion of individuals with other forms of hyperlipidemia, thus necessitating further investigation into genetically defined patients. Lastly, given the nature of the NHANES database, the scope of our study results fundamentally applies only to the U.S. population, and whether our conclusions are applicable to different ethnicities or countries outside the United States requires further exploration.



Comments (0)