In this study, we compared the diagnostic performance between target-μFR and vessel-μFR using the FFR ≤ 0.80 as reference standard. The primary study findings are summarized as follows: 1) the μFR, a novel physiological assessment methods, estimates the pressure drop due to coronary stenosis according to semiautomatic delineation of target vessels and FFR simulation from single-angle; 2) both target-μFR and vessel-μFR have demonstrated high correlations and great agreements with FFR; 3) the ability of target-μFR defining hemodynamic significant of coronary stenosis was similar to vessel-μFR; 4) the selection of the measurement location has less influence on the accuracy of μFR. Hence, it showed the potential in the coronary imagine and virtual physiological evaluation of CAD. The ability of μFR highlights that by integration of the imaging information in order to enable a comprehensive assessment of the CAD [11,12,13,14].
DEFER, FAME and FAME II establish FFR as the"gold standard"of coronary physiology for assessing coronary artery stenosis, treatment plan formulation and evaluation of treatment effect [4, 22, 23]. However, as an invasive method, the application of FFR requires expensive equipment and has potentially procedure-related complications, such as non-fatal myocardial infarction, cerebrovascular accident, and has been limited in clinical practice because of the invasive of the procedure, requirement of pressure wire, the administration of hyperemic agents and so on [3,4,5, 24]. To solve these limitations and reduce the complications, the QFR had been developed which is a virtual FFR technique derived from coronary angiography. Then μFR as a novel angiographic-based method could enable fast computation of FFR, which provides an avenue for determining the most appropriate therapy for the intermediate lesions.
A large number of clinical studies have confirmed the accuracy of QFR in assessing coronary artery function. In FAVOR Pilot Study, the fix-flow QFR (fQFR), contrast-flow QFR (cQFR) and adenosine-flow QFR (aQFR) was compared with the FFR to evaluate the capability in predicting coronary stenosis. The results confirm that fQFR, cQFR and aQFR had shown the great agreement and diagnostic performance (accuracy 80%, 86%, and 87%) for predicting ischemia myocardial [9]. Then, in the FAVOR II China, QFR demonstrated significantly higher sensitivity and specificity for indentifying hemodynamically significant stenosis compared to QCA (94.6% vs. 62.5%; 91.7% vs. 58.1%). The FAVOR II China also revealed that vessel-level QFR had a high diagnostic accuracy of 93.3% [10]. In a large study of FAVOR II E/J, the good diagnostic performance of QFR assessed the degree of coronary stenosis (accuracy 86.3%, specificity 86.9%, sensitivity 86.5%, AUC 0.92) and evaluated the calculation time of QFR and FFR. Furthermore, the time to complete QFR (5 min) was significantly shorter than the time to complete FFR (7 min) [11]. The FAVOR II China and FAVOR II E/J had proved that the diagnostic accuracy of QFR at both the patients and vessels level was better than QCA in the assessment of the relevance of functional stenoses. Subsequently, Wienemann etal further verified the good diagnostic performance of cQFR was maintained in different clinical subpopulations (including gender, aortic stenosis and atrial fibrillation, etc.) and different anatomical subpopulations (including focal and non-focal lesions, etc.) [25]. In a head-to-head study, QFR showed good agreement with FFR compared with SPECT and PET. Meanwhile, the accuracy of QFR was 88%, 82% for SPECT and 78% for PET [26]. Furthermore, the QFR is the only functional system that has been rigorously evaluated for its clinical value in a randomized clinical trial. In FAVOR III China, after 1-year of follow up, patients randomised to the QFR-guide strategies demonstrated better outcomes driven by fewer myocardial infractions and ischemia-driven revascularisations [27]. Recent findings from the FAVOR III Europe trial highlight the non-inferiority of angiography-derived QFR compared to FFR-guided strategies, supporting the clinical utility of virtual FFR methods likeμFR [28]. Based on those studies, QFR has demonstrated good diagnostic accuracy in detecting myocardial ischemia. Meanwhile, QFR could more conveniently calculate virtual FFR after CAG without any pressure-wire assessments, further providing clinical support for revascularization strategies.
However, the QFR investigations discussed above seldom exhibit target-specific QFR. In previous studies, they demonstrated that the choice of virtual-FFR measurement locations is particular importance when identifying ischemic lesions or guiding treatment strategies [15,16,17]. Series studies demonstrated that target-specific virtual-FFR, such as target-specific CT-FFR, can reclassify positive patients defined by the vessel-derived FFR value, and that target-specific FFR has higher diagnostic performance than vessel-derived FFR [29,30,31,32]. The possible causes of the above phenomenon were as follows: 1) the virtual FFR measurement at far distal segments may overestimate coronary ischemia, 2) these differences between vessel territories in pressure gradients for segments 1–2 cm distal to the stenosis versus far distal segments relate to the larger territory of perfused myocardium, 3) the virtual FFR were only assessed in the main coronary arteries, which may have disregarded the impact of collateral stenosis on myocardial ischemia [6, 16]. Then, Kołtowski Ł et al. analyzed the diagnostic performance of index QFR, vessel QFR (assessment for entire segmented vessel) and lesion QFR (assessment for the target lesion) to identify the best measurement location for optimal accuracy of QFR. The research demonstrated the index QFR value which obtained at the pressure transducer position was the best corresponding QFR model [33]. Although the μFR had been showed great agreement and correlation with standard three-dimensional QFR (R 0.996) [34], the diagnostic performance of target-μFR was similar with the vessel-μFR (P > 0.05).
In previous studies, the μFR demonstrated powerful and superior diagnostic performance for target-specific ischemia compared with angiography alone regardless of coronary calcification, and the μFR further reduced the assessment time (67 ± 22 s) [14]. Hence, this paper explores whether target-μFR could further improve the diagnostic ability of myocardial ischemic by comparing the diagnostic performance of target-μFR and vessel-μFR. The diagnostic performance (accuracy 87.67%,sensitivity 86.44%, specificity 88.51%) and AUC (0.936) of vessel-μFR were similar to those reported in previous studies. Then, those indexes of target-μFR (accuracy 91.78%,sensitivity 92.98%, specificity 91.01%), and AUC (0.937) were similar to vessel-μFR and previous research. At the same time, we found the calculation time of target-μFR (1–2 min) and vessel-μFR (1–2 min) was shorter than the QFR reported in previous papers (5 min) [11]. Because of that, the μFR could assess the degree of coronary stenosis which is a time-efficient and accurate method, the visualized anatomic geometry of the coronary artery can provide guidance for subsequent therapeutic regimens. What’s more, based on the U-Net architecture, Murray Law and artificial intelligence, μFR automatically outlines the lumen of the target vessels and their collaterals through artificial intelligence [14]. Hence we suggest the accuracy of μFR have almost less influence by the selection of the remote measurement locations. Based on the difference of the sensitivity, we suggest that the choice of measurement points during the calculation of μFR should be as close as 2–3 cm as possible to the distal end of the culprit vessel which may streamline decision-making by reducing reliance on distal vessel analysis. At the same time, μFR behaved similarly well in sexes and has great diagnostic performance, indicating its potential as a reliable wireless tool for identifying functional ischemia [35].
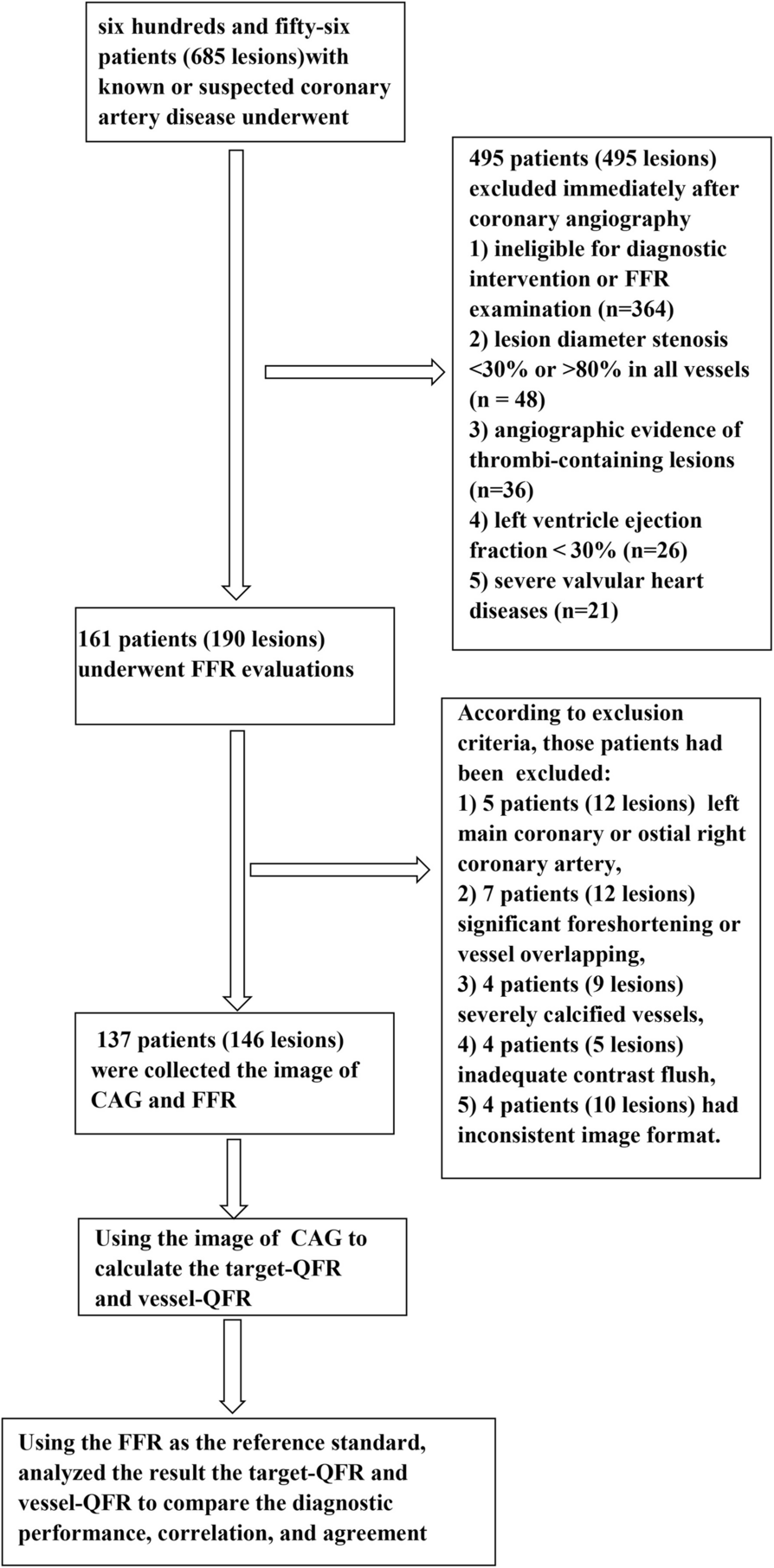
However, our study had several limitations. First, the study was conducted as a single-center, retrospective analysis with a limited sample size, potentially leading to selection bias despite the inclusion of consecutive patients. Furthermore, the statistical efficiency of the study was compromised by the small number of enrolled patients, which was attributed to the low adoption rate of FFR in clinical practice. Secondly, not all the vessels were interrogated for the enrolled patients. The vessels with diameter stenosis < 30% or > 80% were not assessed because performing physiological assessments in such lesions was unnecessary. Thirdly this is a retrospective analysis in which one-third of the data were excluded because the QFR assessment was not applicable, the study should more likely be viewed as a hypothesis-generating study, and further prospective studies would provide more evidence. The availability of QFR can be improved by requiring careful attention to the projection angle and location of the target lesions in coronary angiography; however, the extent to which this can be improved remains to be assessed. Forth, target-μFR and vessel-μFR computation require automatic reconstruction of 3D anatomical models of coronary vessels, and further studies should be consider that analyze the impact of anatomical features on diagnostic accuracy in target vascular lesions. Fifth, there may be inter-operator differences and previous PCI operation effect in the target-μFR and vessel-μFR calculation process, so further evidences from larger studies are needed. Sixth, the selection of the measurement location depends on the location recorded during the FFR evaluation procedure. Influenced by the real world, some of the measurement locations cannot be accurately positioned at the 2–3 cm distal to the target vessels. Hence, further large-sample, multicenter, prospective, and randomized sthudies are vital to further confirm the feasibility of target-μFR in clinical practice.



Comments (0)