
Remember me
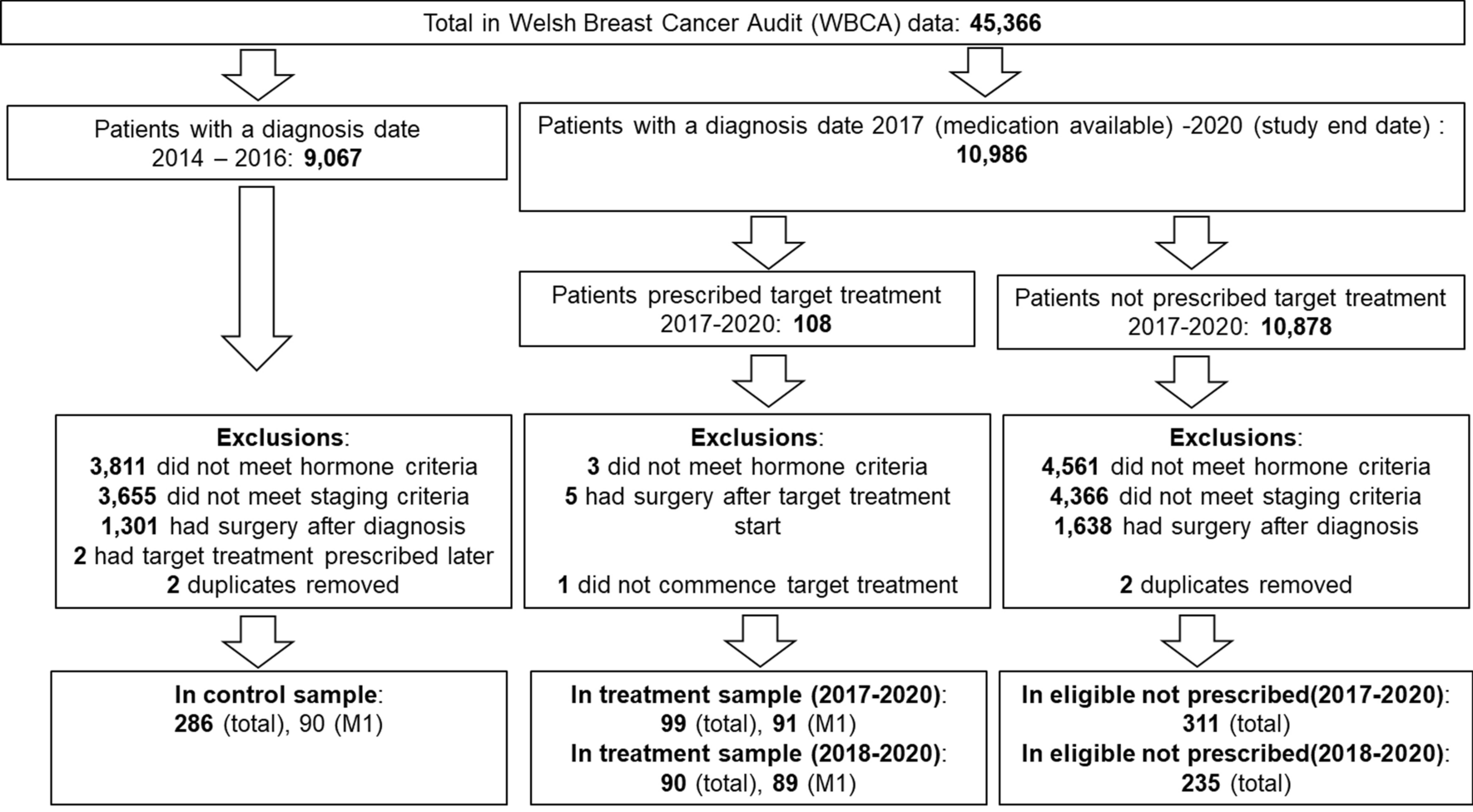
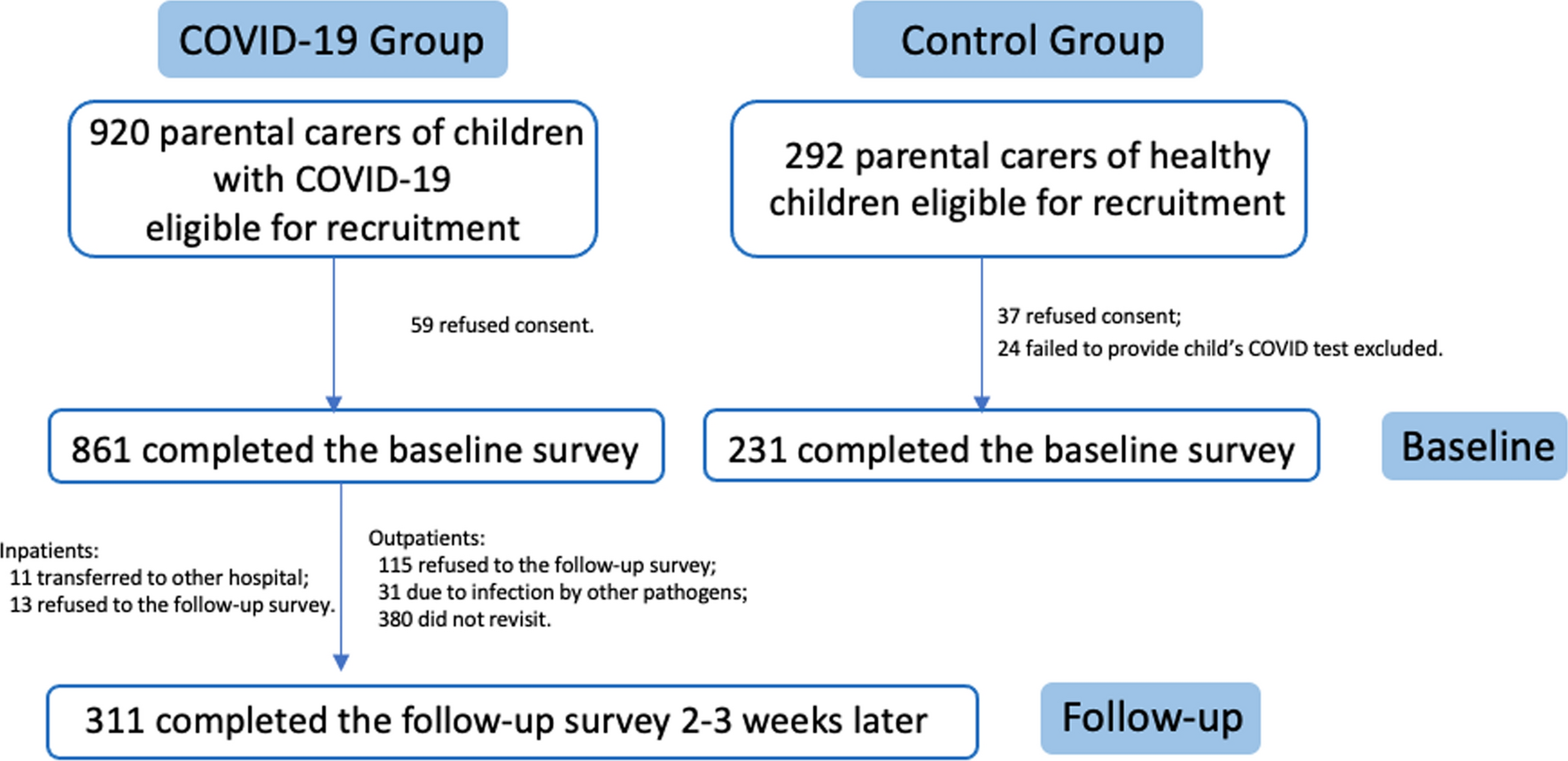




A total of 861 paediatric patients with COVID-19 and their parental carers were recruited from an academic hospital in Shanghai (May 2022 to January 2023). Recruitment involved approaching all eligible patients and their carers during hospital visits. Of the 920 eligible participants, 59 declined to participate. The control group included 231 parents of COVID-19-negative children, recruited via snowball sampling of patients’ siblings and friends.
Eligibility patients were aged 0–18 years, newly diagnosed with COVID-19 (7–10 days prior) via polymerase chain reaction or antigen testing, with no prior COVID-19 history, and hospitalised or receiving outpatient treatment. Exclusions included other respiratory infections (e.g. influenza, adenovirus, respiratory syncytial virus or Mycoplasma pneumoniae) within 3 months before the survey or other underlying illnesses.
The control group included children aged 0–18 years with no COVID-19 history, no symptoms or exposure in the past 3 months, and no recent known infections, confirmed by a recent negative polymerase chain reaction/antigen test. Exclusions were physical limitations or a lack of guardian consent.
Parental carers included primary carers present during the child’s outpatient visits or hospitalisation who were cognitively able to complete surveys. Parents with severe long-term conditions were excluded, but those with COVID-19 were included. Informed consent was obtained from all guardians.
2.2 ProceduresAll consenting patients and parents completed the survey separately, without mutual interaction: patients and carers in clinics or wards using tablets, and healthy controls at home via online platforms to ensure reliable communication. Standardised instructions ensured consistency, and one trained interviewer administered all surveys. Participants were required to respond to each item as fully as possible. Parents provided: (1) sociodemographic data; (2) the EQ-5D-Y-3L proxy version 1 for children aged over 4 years or the EQ-TIPS for children aged under 4 years, with the EQ VAS; (3) their own and their child’s Overall Health Assessment (OHA); (4) the EQ-5D-5L with the EQ VAS; and (5) the EQ-HWB-S.
For children aged over 6 years, the survey included the self-completed EQ-5D-Y-3L with the EQ VAS and OHA. At follow-up (2–3 weeks later), only 311 of 861 participants with COVID-19 completed the same questionnaire, with absences because of transfers, refusals, other infections and non-return (Fig. 1). Clinicians recorded symptoms, length of illness, compliance, severity and treatment per Chinese COVID-19 guidelines [23].
Fig. 1
Inclusion and follow-up of parent carers: study flow chart. COVID-19 coronavirus disease 2019
2.3 InstrumentsThe EQ-HWB-S comprises nine items addressing physical, cognitive and emotional well-being, measured on a 5-point Likert scale, with a 7-day recall period (see Fig. 2 for detailed dimension descriptions) [14]. The Chinese version was translated and culturally adapted per EuroQol Group guidelines [24, 25], showing good acceptability and construct validity [26]. The EQ-HWB-S index values were scored via the UK value set (−0.384 to 1), as no regional utility is available [27]. In this study, a comparative analysis focused on effect sizes (ESs) and regression models, emphasising intergroup differences over absolute index scores, which minimised potential bias from using different value sets [28].
Fig. 2
Distribution of dimension responses at baseline for the EQ-HWB-S (top) and EQ-5D-5L (bottom) for parental carers of children with coronavirus disease (COVID) 2019 and those non-infected. P-values represent differences between the distributions using the chi-square test, and Fisher’s exact test if any cell had an expected count less than 5. The nine items of the EQ-HWB-S and their corresponding response modes are: ‘mobility’ (D), ‘day-to-day activities’ (D), ‘exhaustion’ (F), ‘loneliness’ (F), ‘cognition’ (F), ‘anxiety’ (F), ‘sadness/depression’ (F), ‘control’ (F), and ‘physical pain’ (S). Each item is answered on a 5-point Likert scale assessing difficulty (D: no difficulty, slight, some, a lot of, unable), frequency (F: not at all, only occasionally, some of the time, often, most or all of the time), or severity (S: mild, slight, moderate, severe, very severe or not at all, a little bit, somewhat, quite a bit, very much). In the figure, the response levels of the EQ-HWB-S are defined as: Level 1: no difficulty/not at all/mild; Level 2: slight difficulty/only occasionally/slight; Level 3: some difficulty/some of the time/moderate; Level 4: a lot of difficulty/often/severe; Level 5: unable/most or all of the time/very severe or very much
The EQ-5D-5L measures five HRQoL dimensions (mobility, self-care, usual activities, pain/discomfort, anxiety/depression) on a 1–5 scale (no problems to unable/extreme problems) [29] and includes a 20-cm EQ VAS (0–100) for self-rated health, using a ‘today’ recall period [30]. Index values, scored via the Chinese value set (−0.391 to 1), reflect better health with higher scores [31].
The EQ-5D-Y-3L assesses children’s HRQoL in five dimensions (mobility, self-care, usual activities, pain/discomfort, feeling worried/sad/unhappy) with three response levels, using the Chinese value set (−0.088 to 1) [32]. The EQ-TIPS, a proxy tool for ages 0–3, covers six dimensions (movement, play, pain, social interaction, communication, eating) with three response levels. In this study, we used a level sum score that ranged from 6 (no problems) to 18 (most severe) [33].
The OHA is a validated measure of subjective health for both children and parents [34]. In this study, it was phrased as “How is your overall health today? Excellent, good, fair, poor, or very poor?” Its proxy version collected the carer’s impression of the child’s health.
Paediatric COVID-19 severity is categorised as: (1) mild: respiratory symptoms such as dry throat, cough and fever; (2) moderate: high fever (>3 days), cough, shortness of breath, respiratory rate <30/min, oxygen saturation >93% and pneumonia on imaging; and (3) severe: high fever over 3 days, tachypnoea, oxygen saturation ≤93%, nasal flaring, wheezing or stridor, altered consciousness, seizures and feeding difficulties with dehydration signs [23]. The Chinese criteria for COVID-19 recovery: (1) normal temperature >3 days; (2) significant symptom improvement; (3) a computed tomography scan showing lesion absorption (for pneumonia); and (4) two consecutive negative reverse transcription-polymerase chain reactions (Ct ≥35) or three consecutive negative antigen tests [23].
2.4 Data AnalysisWe conducted descriptive statistics to summarise demographic, socioeconomic and clinical characteristics, and assessed the distribution, construct validity, test–retest reliability and responsiveness of summary scores (EQ-HWB-S, EQ-5D-5L index scores, EQ VAS) and descriptive systems (dimensions). Response patterns were analysed by item-level frequencies and the proportion reporting ‘no problems’ across all items, indicating ‘full health’ (‘11111’ for the EQ-5D-5L and ‘111111111’ for the EQ-HWB-S).
Known-groups validity was assessed using a gamma distribution with a log-link generalised linear regression model to address the skewed EQ summary scores. Dependent variables were the parent’s EQ-HWB-S/EQ-5D-5L index scores and the EQ VAS, whereas the independent variables (the ‘known groups’) included child’s COVID-19 status, COVID-19 severity, parent’s daily caring time and work impact. The model was adjusted for confounders such as demographics, illness length, parental characteristics and household factors. To fit this model, scores were transformed to disutility as 1—utility for right skew, and the Modified Park test assessed model fit [35, 36].
We hypothesised that carers of children in better health (no COVID-19 or less severe disease) and with a lower caregiver burden (less caring time or work impact) would have higher EQ-HWB-S, EQ-5D-5L index scores and EQ VAS. Independent t-tests were used to compare mean scores; Cohen’s d ES (difference of mean/pooled standard deviation) indicated discrimination ability (0.20–0.49 modest, 0.5–0.79 moderate, >0.8 large). Dimension-level differences were test using the Chi-squared test and Fisher’s exact test, and odds ratios (ORs) assessed the likelihood of reporting ‘no problem’ versus ‘any problems’ in each dimension.
Test–retest reliability was assessed in parents with an unchanged OHA from baseline to follow-up [37], using an intraclass correlation coefficient for summary scores, with an intraclass correlation coefficient >0.7 indicating good reliability [38]. Dimension-level reliability was measured by Gwet’s agreement coefficient (Gwet’s AC1: <0.2 poor, 0.21–0.4 fair, 0.41–0.6 moderate, 0.61–0.8 good, >0.8 very good) [39].
Responsiveness was assessed by correlating a child’s health improvement with a parent’s HRQoL change in summary scores. Improvement, defined as COVID-19 recovery or better scores on a child’s EQ-TIPS, EQ-5D-Y-3L or OHA from baseline to follow-up, were compared using t-tests. Glass’ Δ ES (mean difference divided by baseline standard deviation) measured responsiveness (0.20–0.49 modest, 0.5–0.79 moderate, >0.8 large) [40]. Changes in ‘no problems’ responses by dimension were assessed with ORs. Responsiveness analysis focused on parents of improved children, as most patients were stable or improved at follow-up.
A p-value <0.05 was considered statistically significant. Analyses were conducted using SPSS 26.0 (IBM Corporation, Armonk, NY, USA).
Comments (0)