
Remember me

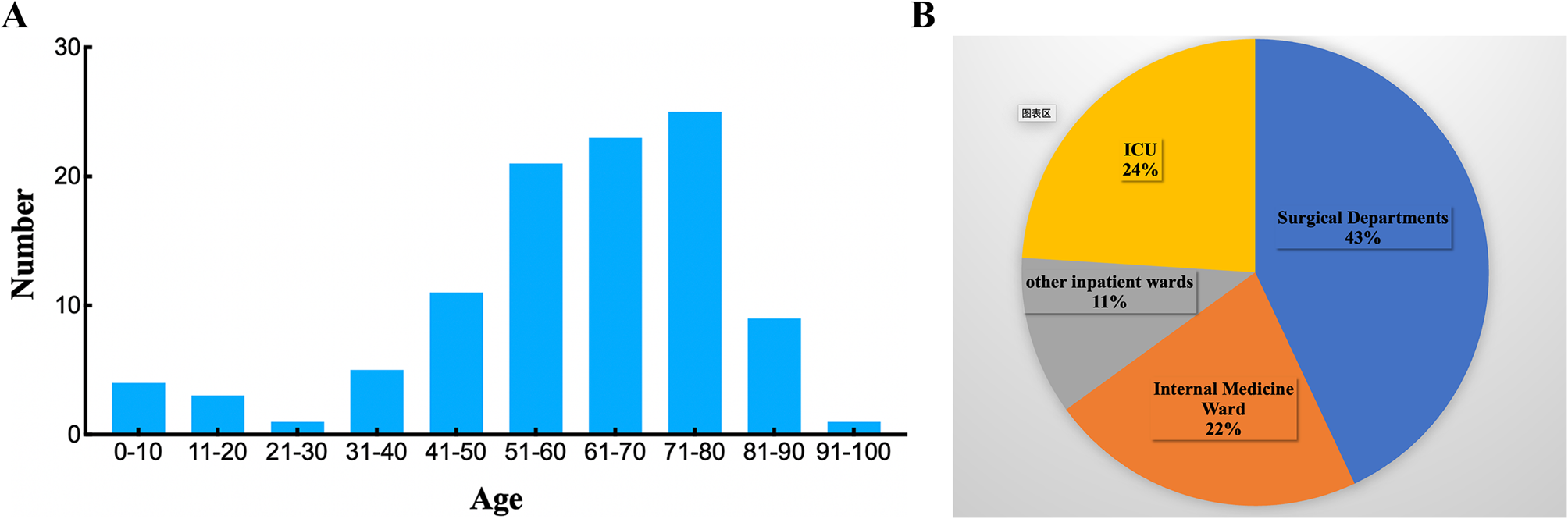




In this study, the detection rates of CREC from 2021 to 2023 were 3.0%, 2.8%, and 3.82%, respectively. 48 CREC isolates were collected from March 2021 to September 2023. With an age range of 3–98 years, the mean age of the patients was 46.14 years. 25 (52.08%) patients were diagnosed with hematological malignancies, 7 (18.6%) with urological malignancy, 4 (8.33%) with lung conditions, 3 (6.25%) with liver-related diseases, 3 (6.25%) with urinary-related diseases, 2 (4.16%) with acute pancreatitis, 2 (4.16%) with acute pancreatitis surgical wound infection, and 5 (10.42%) with other disease (cervical malignancy, osteoporosis and so on). Among the specimens, perianal swab (n = 12,25%), urine (n = 10, 20.83%), drainage fluid (n = 7, 14.58%), stool (n = 7, 14.558%), secretors (n = 5, 10.42%), blood (n = 4,8.33%), and sputum (n = 3, 6.25%) were procured. Of the 48 carbapenem-resistant cases, 81.25% (39/48) produced carbapenemase (carbapenemase-producing CREC, CP-CREC), while 18.75% (9/48) did not produce carbapenemase (non carbapenemase-producing CREC, non-CP-CREC). Furthermore, ESBL production was observed in 87.5% (42/48) of the isolates.
Resistance genes and virulence genes profileA further test was performed to determine whether the CREC strains carried genes for carbapenemase. It was observed that 64.58% (31/48) of isolates carried blaNDM−5 with the higher prevalence of blaNDM−1 (10.42%, 5/48), while blaNDM−4 and blaNDM−13 were detected in 3.8% (1/48) of strains, respectively. One of 48 isolates had two carbapenem-resistance genes (blaNDM−5 and blaOXA−48) present simultaneously. We screened all the CREC strains for the presence of mcr-1, mcr-2, mcr-3, mcr-8, and mcr-9 genes.Two strains carried mcr-1 but not the other mcr genes, which coexist with blaNDM.
Moreover, bacteria also possess genes encoding resistance to antibiotics such as beta-lactams, sulfonamides, streptomycin, aminoglycosides, quinolones, and tetracycline. Among the ESBL-resistance genes positive strains (39/48,81.25%), 25 carried the blaCTXM−10, 15 carried the blaCTXM−1, 12 carried the blaCTXM−9 gene, and 7 carried the blaCTXM−9. 33.3% (16/48) of isolates had blaCTX−M and TEM genes simultaneously, along with 2.08% (1/48) of isolates that had both blaCTX−M and SHV genes. In total, 40 aminoglycoside resistance gene-positive CREC isolates were PCR positive for ant3 (10 isolate), ant3 plus aac3-II (10 isolates), aac3-II (8 isolates), aac3-II plus aac6-IB (3 isolates), ant3 plus rmtB (2 isolates), ant3, aac3-II plus rmtB (2 isolates), ant3 plus aac6-IB (2 isolates), aac6-IB, aac3-II plus rmtB (2 isolates), ant3, aac3-II, rmtB plus aac6-IB (1 isolates), ant3, aac3-II, armA plus aac6-IB (1 isolates), aac6-IB and aac3-II (1 isolates), ant3, aac6-IB and aac3-II (1 isolates), aac6-IB (1 isolates), ant3 and aac3-II (1 isolates).
In total, 4 quinolone resistance genes were found, including 20 strains carrying gyrA (41.67%), 5 strains carrying qnrS (10.42%), 10 strains carrying both gyrA and qnrS (20.83%), 3 strains carrying both gyrA and qepA (6.25%), 1 strain carrying qnrS, gyrA, and qepA (2.08%), and 1 strain carrying qnrS, qnrB, and gyrA (2.08%). In addition, the tetA, sul1 and strA genes were detected in 38, 20, and 13 isolates, respectively (Table 1; Fig. 1).
It was found that the most prevalent virulence-associated gene was fimH (93.75%, 45/48), followed by ecpA (89.6%, 43/48), traT (60.4%,29/48), iucD (45.8%, 22/48), ompT (35.4%,17/48), afaC (4.2%,2/48), papC (2.1%,1/48) (Fig. 2).
CTX-M type ESBLs were found in all non-CP-CREC. Of the 9 non-CP-CREC isolates, 44.44% (n = 4) showed deletion in ompC and ompF porin-encoding genes (Table 2). The other five non-CP-CREC without pore-protein deletion had high expression of the efflux pumps genes acrA, acrB, and tolC (Fig. 3).
Fig. 1
Molecular characterization of resistance genes in CREC isolates as detected by PCR
Fig. 2
Molecular characterization of virulence genes in CREC isolates as detected by PCR
Fig. 3
mRNA level of AcrA/B-TolC expressed in 5 non-CP-CREC strain Values represent the relative mRNA level of AcrA/B-TolC normalized to CSEC. Datas shown are the average values from three independent experiments, and bars represent standard deviations. ****P < 0.001, ***P < 0.001, **P < 0.01, *P < 0.05
Table 1 Molecular characterization of 48 CREC strainsTable 2 Molecular characterization of 9 non-carbapenemase-producin CRECGenetic profiling and antimicrobial susceptibility analysisIn order to understand the genetic variability of the CREC, MLST was conducted. In total, 48 CREC belonged to 21 STs and five unknown STs (untypable). As shown in Table 1, the most common ST was ST410 (n = 9), followed by ST5229 (n = 4), ST38 (n = 3), ST405 (n = 3), ST648 (n = 3), ST617 (n = 2), ST10 (n = 2), ST155 (n = 2), ST69(n = 2), and ST617 (n = 2), and then by single ST isolates, including ST58, ST539, ST641, ST88, ST156, ST167, ST44, ST457, ST1730, ST297, ST361, and ST48 (Table 1).
All CREC isolates showed a high-level resistance to carbapenems, with 100% resistance to cephalosporins, including cefazolin, ceftazidime, ceftriaxone, and cefepime. Other antimicrobials showed irregular susceptibility and resistance, such as piperacillin-tazobactam (97.9%), ciprofloxacin (95.8%), levofloxacin (87.5%), sulfamethoxazole-trimethoprim (85.4%), gentamicin (76.2%), aztreonam (62.5%), and tobramycin (50%), whereas the highest susceptibility was recorded for polymyxin B (4.17%) (Fig. 4).
Fig. 4
Susceptibility of CREC isolates to different antimicrobial agents. Note: CFZ: cefazolin; PMB, polymyxin B; SXT, Trimethoprim-Sulfamethoxazole; CRO, Ceftriaxone; IPM, imipenem; TZP, piperacillin-tazobactam; CIP, ciprofloxacin; LEV, levofloxacin; GEN, gentamicin; ATM, aztreonam; TOB, tobramycin; AMK, amikacin
Results of transferability of plasmids carrying mcr-1 or bla NDMConjugation assays confirmed that blaNDM−1, blaNDM−13, and most blaNDM−5 (68.75%, 22/32) could be transferred between E. coli strains, with an observed transfer frequency ranging from 4.19 × 10^−1 to 1.80 × 10^−4. The antibiotic susceptibility testing results showed that the transconjugants, confirmed by PCR and sequencing, were resistant to imipenem (4 mg/L). It was found that the blaNDM−4 gene carried on the plasmid in strain CREC339 could not be transferred to EC600. The plasmid carrying the mcr-1 gene from strains CREC055 and CREC339, as well as the plasmid carrying the blaNDM−5 gene from 10 CREC strains, were unsuccessfully transferred to the recipient.
Risk factors for CREC infectionDue to incomplete case data, two patients detected by CREC infection were excluded. A comparison of the risk factors for acquiring CREC between CREC and CSEC groups is presented in Table 3, based on univariate and multivariate analyses. Using univariate conditional logistic regression analysis, it was demonstrated that hospital stay (> 30days), hospitalizations (> 3times), PICC, exposure to antibiotic agents (cephalosporin, aminoglycosides, fluoroquinolones, carbapenems, and antifungal agents), detection other pathogens (prior to CREC infection), surgical history, and respiratory disease were all risk factors for CREC infection. The multivariate conditional logistic regression analysis demonstrated that antibiotic usage (P = 0.004), antifungal use (P = 0.017), detection of other pathogens (prior to CREC infection) (P = 0.000), and respiratory disease (P = 0.016) were identified as independent risk factors for CREC infection (Table 3). After identifying these risk factors, we evaluated whether they could be used as scores to identify CREC infection. A point was assigned to each risk factor, resulting in a total score ranging from zero to four. For the purpose of determining the cutoff value for identifying cases with CREC infection, we performed receiver operating characteristic (ROC) curve analysis (Fig. 5). ROC analysis indicated high accuracy, with an area under the curve (AUC) of 0.937. Table 4 shows the sensitivity and specificity of each score. Youden’s index, with sensitivity and specificity values of 0.96 and 0.78, was maximal when 2 points were scored.
Table 3 Univariate and multivariate analyses of risk factors for CREC infectionTable 4 Accuracy of the proposed scoring system for the diagnosis of CREC infectionFig. 5
Receiver operator characteristic curve analysis for the scoring system
Comments (0)