
Remember me







BOX. KEY EVENTS IN CALIFORNIA STATE CANNABIS HISTORY
Medical cannabis legalization (1996): Medical cannabis was legalized on 5 November 1996, with the passage of Proposition 215, the Compassionate Use Act. The law permitted the use, possession, and cultivation of cannabis by patients with a physician’s recommendation for the treatment of a qualifying medical condition. Dispensaries selling medical cannabis were subsequently introduced. Many medical cannabis dispensaries, both licensed and unlicensed, were operating at the time that recreational cannabis was legalized.
Recreational cannabis legalization (“Legalization”) (2016): Recreational cannabis was legalized on 8 November 2016, with the passage of Proposition 64, the Adult Use of Marijuana Act. The law legalized the possession, use, and personal cultivation of recreational cannabis in California for adults aged 21 years and older. Licenses to cultivate, transport, manufacture, test, or sell recreational cannabis did not become active until 2018.
Initiation of recreational cannabis retail sales (“Commercialization”) (2018): Legal sales of recreational cannabis to adults aged 21 years and older through retail outlets began on 1 January 2018. Cities and counties reserved the option to ban recreational retail cannabis business from siting within their borders, but receipt of home delivery of retail cannabis was permitted statewide beginning in November 2018. Thus, in cities and counties that did not ban retail cannabis businesses, legal retail sales of recreational cannabis became available through storefronts in January 2018 and home delivery in November 2018, whereas in cities and counties that did ban retail cannabis businesses, legal retail sales of recreational cannabis became available only through home delivery in November 2018. Sales occurred through retail outlets that were formerly or concurrently licensed for medical cannabis or through newly opened recreational retail outlets.
A growing number of US states have adopted policies permitting the possession, use, production, and sale of cannabis for recreational purposes. Regulatory changes may have both positive and negative impacts on public health.1,2 One concern raised by public health experts is that cannabis producers (such as tobacco and alcohol) are incentivized to increase potency3,4 and diversify products.3,5,6 Higher potency products may increase risks for cannabis use disorder, psychosis, and other problems.1,7,8 Capacity to enforce product safety standards may also be limited in newly legalized areas.9–12 Consequently, the Food and Drug Administration has called for public health monitoring to identify and respond to cannabis product safety concerns.13
A key source of surveillance data recommended by public health experts are Poison Control centers.2,9 Several types of cannabis-related safety concerns may be captured in Poison Control records. Adults who intentionally consume a recommended dose of a cannabis product may experience adverse effects such as vomiting or psychotic symptoms.9,14 Consumers may also intentionally overdose, defined by poison centers as purposeful exposure to nonstandard doses of tetrahydrocannabinol-containing products with the intent to gain a high, euphoria, or some other psychotropic effect.15 Unintentional overdoses may arise from unfamiliarity with new product types (e.g., concentrates), confusion about dosing, or lack of guidance on safe consumption.16 Acute cannabis overdoses may manifest as vomiting, ataxia, disorientation, psychotic symptoms, or psychological distress.9,14,17,18 Cannabis can be mistaken for other products and consumed unintentionally, particularly by children.19–27 Finally, like most products, cannabis can be spoiled or contaminated with other drugs or chemicals.
Research has documented increases in cannabis-related calls to Poison Control centers following cannabis legalization and commercialization.19–22 In California, cannabis-related calls to Poison Control centers increased by 64% following recreational legalization (November 2016) and an additional 29% following the initiation of recreational retail sales (“commercialization,” January 2018) (Box), particularly among children aged 12 years and under and for edible products.20 Existing studies have focused on state-level patterns, but states can devolve regulatory powers over cannabis to the local level.28–32 In California, cities and counties can determine retail tax rates, limit outlet densities or locations, regulate the types and potency of products sold, establish packaging and labeling requirements beyond state requirements, and mandate whether salespeople need to be trained to advise customers on dosing (e.g., “budtender training”), among others. This local policy variation provides a unique opportunity to compare alternative regulatory strategies and potentially identify effective prevention approaches.
We evaluated whether local cannabis control policies adopted following statewide recreational cannabis commercialization may help prevent increases in harmful cannabis exposures reported to Poison Control. We focus on California, which has the largest legal cannabis market worldwide ($6 billion in annual sales)33,34 and a comparatively high degree of local autonomy in regulating cannabis. We hypothesized that localities that adopted more restrictive regulatory approaches would experience smaller increases in harmful cannabis exposures following commercialization.
METHODS Policy Data Collection and MeasuresThe cannabis policy data collection and coding are described in detail elsewhere.31,35,36 The complete protocol and data collection instrument are provided in eAppendices 1–2; https://links.lww.com/EDE/C129. Briefly, we measured local cannabis control policies for California’s 58 counties and all 482 incorporated cities within them. Incorporated city policies apply within city borders, and county policies apply to areas outside of incorporated cities (“unincorporated county areas”). The combined set of 539 incorporated cities and unincorporated county areas were the mutually exclusive and collectively exhaustive jurisdictions (“localities”) to which distinct policies applied.
Following established legal epidemiology procedures,37,38 we systematically collected and coded characteristics of local cannabis control policies. We used a structured data collection instrument to capture the presence or absence and content of prespecified provisions. Localities were coded independently by two analysts until achieving >95% agreement with interpretations confirmed by a legal expert. Policy data collection was conducted from November 2020 to August 2021.
The local policies we measured were based on an existing taxonomy of all possible cannabis policies developed through literature review and expert discussion.39 We coded all major categories of policies that (1) could be adopted by city or county governments according to state law, (2) were more restrictive than state law, (3) varied across localities, and (4) were plausibly related to public health, based on existing evidence, public health best practices, and expert opinion.28,29,39
In this study, we evaluated three categories of local cannabis control policy measures (Table 1). First, we examined bans on storefront retail businesses selling recreational cannabis (hereafter, “retail bans”). Second, we generated a policy score capturing the overall restrictiveness of a locality’s cannabis control policies by summing the 18 binary policy variables relevant to the operations of retailers and the availability of recreational retail cannabis. Third, we considered specific provisions recommended as potential solutions to harmful cannabis exposures identified by Poison Control:9 limits on product types and potency, packaging and labeling requirements, and server training requirements.9 While some other policies are more common (e.g., retail taxes), these three policies address explicit mechanisms leading to overdoses (e.g., consumer confusion about dosing). We examined the restrictiveness score and specific provisions for the subset of localities without retail bans. For all three categories, the exposures were cross-sectional measures of the policies applicable at the time of data collection. Because statewide commercialization preceded data collection, we interpret our estimates as patterns in harmful cannabis exposures in localities that did versus did not adopt the given policy by 2021. To assess whether the measured policies were effective throughout the postcommercialization period 2018–2021, we retrospectively evaluated a random sample of 20 localities. We found that 50% had unchanged policies throughout 2018–2021, 15% made minor changes (e.g., clarifying a definition), and 35% made major changes. See eAppendix 3; https://links.lww.com/EDE/C129 for details.
TABLE 1. - California Local Cannabis Control Policy Measures Adopted by 2021 Policy Measure Description Summary Statistic(s) Bans on storefront recreational retail cannabis businesses The state permits commercial businesses for the retail sale of recreational cannabis with a state-issued license. However, localities can ban retail cannabis businesses from siting within the locality’s borders. We focused on local bans on businesses selling recreational cannabis instead of medical cannabis because our study covers the postrecreational legalization period.a We focused on storefront (brick-and-mortar) businesses as opposed to home delivery retailers, because receipt of home delivery was legal statewide, versus physical proximity to outlets offering in-person purchases.40 Localities banning storefront recreational retail businesses by 2021: 69% Overall restrictiveness of cannabis control policies We created a policy score capturing overall restrictiveness by summing the 18 binary policy variables relevant to the operations of retail outlets and availability of retail recreational cannabis: bans on on-site consumption, outlet density limits, outlet location limits, bans on outlet overconcentration in vulnerable communities, restrictions on outlet locations in relation to alcohol outlets, limits on hours or days of sale, outlet buffers around sensitive locations such as schools, buffers between outlets, requirements for outlet upkeep, requirements for outlet safety (e.g., night lighting), limits on advertising and marketing, liability for hosting underage consumption (social host), restrictions on special outdoor events involving cannabis, limits on product types or potency, restrictions on packaging and labeling, server training requirements, taxes on retail purchases, and other price controls. This list includes all cannabis control policy measures we collected except those pertaining to bans on cannabis cultivation, manufacture, distribution, or testing businesses. Median (minimum, maximum): 7 (1, 13)b Specific provisions Limits on product types and potency Applicable local policies include bans on specific product types such as cannabis-infused beverages or flavored combustibles, or maximum allowable tetrahydrocannabinol potency levels of products. Localities adopting any limits by 2021: 7%b Requirements for product packaging or labeling Applicable local policies include supplemental warning labels (beyond those required by state law) and requirements of plain packaging (e.g., no depictions of persons, characters, or animals). State law mandates that cannabis products cannot be attractive to children and should not be easily confused with non–cannabis-containing commercially available foods. Local policies in this category also include heightened standards for what qualifies as attractive to children or appearing like a non–cannabis-containing product. Localities adopting any requirements by 2021: 13%b Server training requirements Applicable local policies include mandatory or voluntary “budtender” training requirements for retail licensees, managers, servers, or other employees of retail businesses. The content of the training may include advising customers on recommended dosing or procedures for preventing sale to intoxicated persons or minors. Training may be provided by the local government, the permittee, or a third party. Localities adopting any requirements by 2021: 3%baReceipt of cannabis home delivery is legal statewide, but localities can ban businesses offering delivery from siting within their borders.
bValues are reported for the subset of localities that permit recreational retail cannabis businesses.
We used data collected by California Poison Control System (CPCS), a network of four call-answering sites. CPCS maintains a free 24/7 hotline providing expert advice on exposure management to the lay public and medical practitioners. We analyzed all CPCS calls from 1 January 2011 to 31 December 2020 originating from California and involving human exposure to “marijuana” (ingested, inhaled, absorbed, or applied to the body), based on product codes used by all accredited US Poison Control centers to identify cannabis-containing products. Call records included patient demographics, caller location, substance, route of exposure, symptoms, treatment, and medical outcomes. The Institutional Review Board of the University of California, San Francisco approved this study.
Medical outcomes (hereafter, “severity”) were categorized following Poison Control standards into no effect, minor, moderate, and severe.15 Examples of minor effects included self-limited gastrointestinal illness; moderate effects included pronounced or systemic symptoms typically requiring treatment (e.g., psychosis); severe effects were life-threatening (e.g., respiratory compromise requiring intubation) or death. In the primary analysis, we excluded cases with no effect (e.g., informational calls), instead focusing on harmful cannabis exposures, defined as those involving minor, moderate, or severe medical outcomes. We aggregated individual call record data to the locality–quarter level. The primary outcome was the rate of harmful cannabis exposures reported to CPCS using census-based denominators. Additional detail on outcome classification and data cleaning procedures is provided in eAppendix 3; https://links.lww.com/EDE/C129.
Statistical AnalysisWe merged the local cannabis policy data to CPCS outcomes by locality. Of the original 539 localities, we excluded four for which no legal text could be identified and four that did not specify whether recreational retail cannabis businesses were permitted. The final analytic dataset included a balanced panel of 531 localities over 40 quarters.
To estimate the associations of the local cannabis control policies adopted by 2021 with harmful cannabis exposures before and after commercialization, we applied a two-way fixed effects design,41 a generalization of differences-in-differences for the setting with multiple treated units. Our modeling approach was based on a simulation study that compared the performance (bias, precision) of common approaches for estimating policy effects in panel data.42 The authors found that the optimal method was a negative binomial model that included an autoregressive effect.42 However, some locality–quarters had no harmful cannabis exposures, so incorporating autoregressive terms would have involved log(0). We, therefore, employed the next-best approach identified by the study and used negative binomial regression to model the rate of harmful cannabis exposures as a function of the policy variables, locality fixed effects, and quarter fixed effects with standard errors clustered at the locality level (see eAppendix 3; https://links.lww.com/EDE/C129 for statistical model). The locality fixed effects controlled for time-invariant characteristics of localities (e.g., political orientation, population density, and wealth) and the quarter fixed effects controlled for temporal patterns that were universal across localities (e.g., statewide legalization and trends in cannabis product potency) that would otherwise confound the results. Remaining potential confounders are time-varying, locality-specific factors that relate to (1) which local cannabis policies were adopted and (2) rates of reported harmful cannabis exposures. Additionally, our approach relies on the assumption of parallel trends on the multiplicative scale.43 That is, we assume that the trends in the log-transformed outcome rates in the localities that did not adopt the given policy are parallel to the trends in the outcomes in the localities that did adopt the policy, had these localities (counter-to-fact) not adopted the policy (see eAppendix 3; https://links.lww.com/EDE/C129 for detail). We are not aware of any concurrent changes that affected harmful cannabis exposures, supporting the plausibility of this assumption, but we cannot rule out uncontrolled confounding. Under the assumptions of parallel trends and no anticipation, the exponentiated coefficient on the policy exposure variable is the standard differences-in-differences estimate of the average treatment effect on the treated (in this case, an associational rate ratio [RR]).41
All analyses were stratified by age group (under 13 years vs. 13 years and older), because prior research indicated differential impacts of statewide recreational cannabis commercialization between these two age groups20 and because exposures for the younger age group were frequently unintentional consumption of edibles whereas exposures among older age group were more often intentional and varied in product type.20 We fit separate models for each category of policy measures: first, retail bans, among all localities; second, overall restrictiveness, among localities without retail bans; and third, the three specific provisions plus a new restrictiveness score made up of the remaining 15 cannabis control policies (without the three specific provisions), among localities without retail bans. For analyses involving overall policy restrictiveness, we standardized the policy score so that estimates correspond to the change in the rate of harmful cannabis exposures associated with a 1-standard deviation increase in the policy restrictiveness score, a substantial increase in restrictiveness (see eFigure 1; https://links.lww.com/EDE/C129).
In subgroup analyses, we stratified the outcome by patient gender (men, women), mode of cannabis product consumption (ingested, inhaled), medical outcome severity (minor, moderate, major/death), and caller site (community, health care facility). To test the robustness of our results to our specification choices, we conducted sensitivity analyses in which we (1) restricted to exposures involving cannabis but no other substances and (2) included cases of unknown severity (see eAppendix 3; https://links.lww.com/EDE/C129). Consistent with increasing concerns about the value of null hypothesis significance testing, we do not adjust for multiple comparisons.44,45 All analyses were performed in R version 4.3.0, The R Foundation for Statistical Computing, Vienna, Austria (see eAppendix 4; https://links.lww.com/EDE/C129 for code).
RESULTSOf 539 localities, we obtained the cannabis control policy text for 535 (99%). Of these, 69% had retail bans (Table 1). Among the 167 localities without retail bans, the median cannabis policy restrictiveness score was 7 (range: 1–13). Only 7% of localities placed any type of limit on product types or potency, 13% adopted any requirements for product packaging and labeling beyond state laws, and 3% placed some form of server training requirement.
There were 7906 harmful cannabis exposures reported to CPCS over the study period, and we linked 7,668 (97%) to their originating locality (Table 2). Among the cases, 55% were men, 76% were people aged 13 years or older, 59% involved cannabis only (vs. cannabis and other substances), 80% involved ingestion (vs. inhalation or another route of exposure), 71% were minor severity, and 66% were calls made from health care facilities. Reported exposures increased over time from 565 in 2011 to 1,343 in 2020.
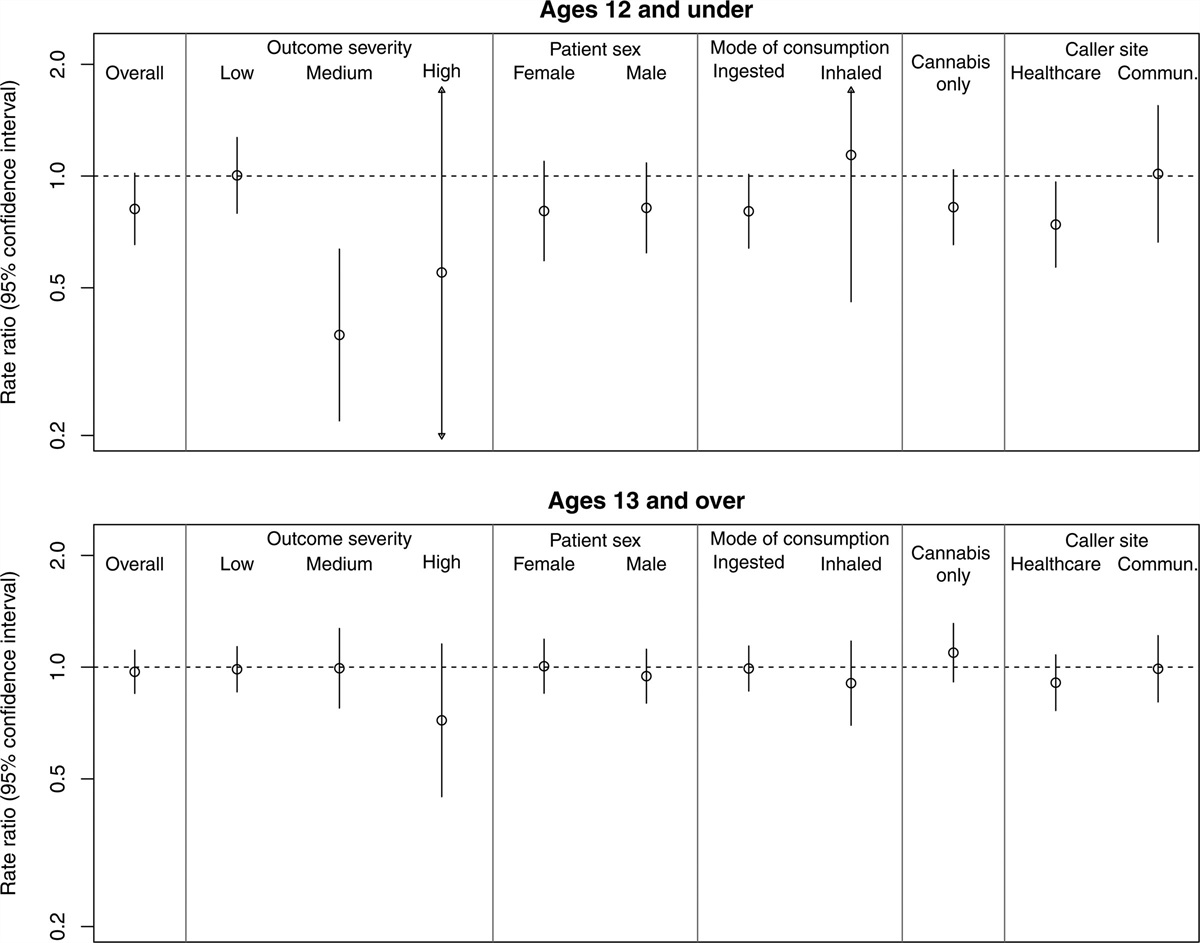
TABLE 2. - Characteristics of Harmful Cannabis Exposures Reported to the California Poison Control System, 2011–2020, Overall and by Locality Stance on Storefront Recreational Retail Cannabis Businesses in 2021 Characteristic Overall Localities Banning Storefront Recreational Retail Cannabis by 2021In adjusted analyses (Figure 1), localities that adopted bans on storefront recreational retail cannabis businesses by 2021 had 18% fewer harmful cannabis exposures for people aged 12 years and under compared to localities not adopting such bans by 2021 (RR = 0.82; 95% confidence interval [CI] = 0.65, 1.02). However, we observed no association for people aged 13 years and older (RR = 0.97; 95% CI = 0.85, 1.11). For people aged 12 years and under, this RR corresponds to approximately 10 cases averted annually (2018–2020) among all localities adopting retail bans by 2021 combined. Subgroup analyses revealed that the reduction in harmful cannabis exposures for those <13 years applied primarily to moderate severity cases (RR = 0.37; 95% CI = 0.22, 0.64), ingested products (RR = 0.80; 95% CI = 0.64, 1.01), and calls originating from health care facilities (RR = 0.74; 95% CI = 0.57, 0.96). In subgroup analyses for ages 13 and older, associations with retail bans were generally null. One exception was that retail bans were associated with lower rates of high-severity cannabis exposures, but this estimate was imprecise (RR = 0.72; 95% CI = 0.45, 1.15).
 FIGURE 1.:
FIGURE 1.: Estimated associations of local bans on storefront recreational retail cannabis businesses with rates of harmful cannabis exposures reported to the California Poison Control System, 2011–2020.
In adjusted regression analyses restricted to the 167 localities without retail bans by 2021 (Figure 2), the overall restrictiveness of a locality’s cannabis control policies in 2021 was not associated with changes in harmful cannabis exposures among children aged 12 years and under, overall or for any subgroup. For people aged 13 years and older, localities with a 1-standard deviation higher level of overall restrictiveness experienced 7% fewer harmful cannabis exposures for people aged 13 years and older compared with less restrictive localities (RR = 0.93; 95% CI = 0.86, 1.01), corresponding to approximately 11 cases averted annually among all localities adopting more restrictive approaches to cannabis control by 2021. This finding was driven by medium-severity cases (RR = 0.82; 95% CI = 0.71, 0.94) and calls originating from health care facilities (RR = 0.89; 95% CI = 0.80, 0.98).
 FIGURE 2.:
FIGURE 2.: Estimated associations of overall restrictiveness of locality cannabis control policies with rates of harmful cannabis exposures reported to the California Poison Control System, 2011–2020. Estimates correspond to the change in the rate of harmful cannabis exposures associated with a 1-standard deviation (SD) increase in the policy restrictiveness score.
For limits on product types or potency, packaging and labeling requirements, and server training requirements, we generally did not detect differences in rates of harmful cannabis exposures between localities with and without these policies by 2021 (eFigures 2–4; https://links.lww.com/EDE/C129). Fewer than 15% of localities adopted these policies (Table 1) and we restricted analyses to the 167 localities without retail bans by 2021. Thus, estimates were imprecise. There was some indication that localities adopting packaging and labeling requirements by 2021 experienced fewer harmful cannabis exposures among people aged 13 years and older, specifically for male patients (RR = 0.76; 95% CI = 0.60, 0.97) and calls originating from the community (RR = 0.70; 95% CI = 0.58, 0.83). Server training requirements were also unexpectedly associated with more harmful cannabis exposures among people aged 13 years and older (RR = 1.23; 95% CI = 1.01, 1.51).
Results from sensitivity analyses including cases of unknown severity were consistent with the main results (eFigures 5-9; https://links.lww.com/EDE/C129).
DISCUSSIONIn this statewide retrospective study of all 539 California localities (cities and counties), the restrictiveness of local cannabis control policies adopted by 2021 was associated with differential rates of harmful cannabis exposures reported to the CPCS following before versus after statewide cannabis commercialization in 2018. Local bans on storefront recreational retail cannabis businesses by 2021 were associated with 18% fewer harmful cannabis exposures among children under 13 years, but no difference in harmful cannabis exposures among people aged 13 years and older. Among the 167 localities without retail bans, more restrictive local approaches to cannabis control by 2021 were associated with fewer harmful cannabis exposures for people aged 13 years and older, specifically for medium-severity cases and calls originating from health care facilities. We also examined specific cannabis control provisions proposed as solutions to harmful cannabis exposures: limits on product types and potency, packaging and labeling requirements, and server training requirements.9 However, we found that these policies were rarely adopted by 2021 and corresponding estimates were generally too imprecise to determine their effectiveness. Overall, these findings are important for informing local governments’ approaches to prevent harmful cannabis exposures, because they suggest that taking more restrictive approaches to local cannabis control may help mitigate some increases in harmful cannabis exposures following statewide recreational cannabis commercialization.
Increases in harmful cannabis exposures reported after commercialization may reflect a greater willingness to call Poison Control after penalties for possession and use were lifted for adults aged 21 and older.19,20 This may have been especially true in localities that permitted local retail, whereas calls may have increased less in places with retail bans. However, this reporting bias cannot explain all the findings because we observed increases in harmful cannabis exposures after commercialization when recreational cannabis use had already been decriminalized for several years. Additionally, the changes we observed occurred primarily for calls originating from health care providers, whose propensity to call Poison Control is unlikely to be affected by cannabis laws.
Local cannabis control policies designed to reduce the availability and demand for recreational cannabis, including retail bans, may contribute to lower levels of cannabis use and corresponding problems. In particular, changes in rates of harmful cannabis exposures may reflect differential availability, purchasing, and use of cannabis products, particularly high-potency and edible products that may be less familiar to users. In most states legalizing recreational cannabis, cannabis use increased among adults,46 and edibles increased in popularity.47 Potency of cannabis products also increased.5,6 In California, the proportion of cannabis-related CPCS calls attributable to chocolates, candies, gummies, and other edibles increased dramatically following statewide legalization.20 When recreational cannabis sales began in 2018, many localities introduced recreational cannabis retail outlets by converting existing medical cannabis dispensaries; these outlets were therefore poised to distribute diverse high-potency cannabis products.48,49 Lower availability of these products, in places with retail bans and in places that permitted businesses but regulated them, may have resulted in fewer harmful cannabis exposures relative to localities with less restrictive policies.
We cannot rule out the possibility of uncontrolled confounding or reverse causation. Localities adopting more cannabis control policies may be those with larger cannabis markets. Restrictive policies may also be adopted in response to more frequent problems (i.e., reverse causation), consistent with prior work showing that restrictions on outlet overconcentration in historically disinvested neighborhoods were more common in California localities with such problems.35 In future studies, longitudinal policy measures would help rule out reverse causation. Additionally, not all localities have the capacity or expertise to develop nuanced cannabis control regulations; more restrictive or complex policies may reflect the greater capacity of larger localities, which are also more likely to experience a harmful cannabis exposure because the population is larger. The ongoing presence of a widespread illegal cannabis market50 and misalignment between the frequency of cannabis use and cannabis use problems may also contribute to variation in our findings.
Lower rates of harmful cannabis exposures associated with more restrictive cannabis control policies were driven primarily by medium-severity cases (defined as non–life-threatening cases needing medical attention). The policies we studied may therefore be more relevant for cannabis exposures serious enough to require medical attention. While minor cases are a nuisance, they are unlikely to be a major threat to population health. In contrast, preventing serious cannabis-related harm is a public policy imperative. Our findings suggest that retail bans and more restrictive overall approaches to local cannabis control may help prevent some of these cases (medium severity).
Consistent with prior research,20 our findings differed for children aged 12 and under compared with people aged 13 and older. Local retail bans were associated with fewer harmful cannabis exposures for children aged 12 and under, whereas more restrictive overall approaches to local cannabis control among localities permitting retail were associated with fewer harmful cannabis exposures for people aged 13 years and older. If these associations are causal, they suggest that banning recreational cannabis retail altogether is more likely to be effective in preventing harmful cannabis exposures among children, whereas for the older age group, permitting but constraining recreational cannabis retail may be sufficient. Harmful cannabis exposures among children typically involve unintentional ingestion of edibles, whereas harmful cannabis exposures among adults more often involve intentional consumption of various products.20 Prevention strategies may need to be tailored to the type of product (e.g., ingested versus inhaled) and the nature of the exposure (i.e., intentional versus unintentional). For example, prevention of child exposures may be centered around child supervision or safe sto
Comments (0)