
Remember me





Dematiaceous or black fungi are a heterogeneous group of fungi widely distributed in soil and decomposing plant material, mainly in tropical and subtropical regions [1]. They are characterised by the presence of melanin in their cell walls, leading to brown hyphae and conidia that form characteristic dark-coloured colonies [2]. Dematiaceous fungi can cause a variety of human infections, known as chromoblastomycosis and phaeohyphomycosis, and their ability to produce melanin is considered as an important virulence factor [3, 4]. Chromoblastomycosis, also called chromomycosis, is a chronic granulomatous infection of the skin and subcutis where, histopathologically, so-called Medlar bodies or sclerotic bodies are present in the affected tissue [5]. Phaeohyphomycosis can occur in both immunocompromised and immunocompetent individuals and lead to cutaneous, soft tissue, respiratory tract, and central nervous system (CNS) infections [4].
Most cases of ocular phaeohyphomycosis are exogenous and acquired through contaminated corneal or conjunctival injuries or following ocular surgery [6]. The most common dematiaceous fungal eye infection is keratitis, and its incidence appears to increase [7]. Endophthalmitis following disseminated fungaemia typically occurs in individuals with recent hospitalisation, major surgeries or underlying diabetes, malignancy or other systemic conditions affecting their immune system [8, 9]. Fungal endophthalmitis is usually endogenous in nature and often caused by Candida or Aspergillus species [9,10,11]. Only a few cases of endogenous endophthalmitis caused by dematiaceous fungi have been reported in the literature, and the prognosis is generally poor [12].
Cladophialophora (formerly known as Cladosporium) is a genus of dematiaceous hyphomycetes in the family Herpotrichiellaceae, which includes several pathogenic species [13, 14]. Herein, we present a challenging case of endogenous endophthalmitis caused by Cladophialophora devriesii and provide a brief review of the literature.
Case presentationA 73-year-old Caucasian female had noticed blurred vision and floaters in her left eye for about five months. One week prior to admission, she experienced increasing redness and pain in the same eye. There was no recent history of trauma or foreign travel. Her past medical history included tachycardia-bradycardia syndrome treated with pacemaker implantation 10 years earlier, and recurrent respiratory tract infections and chronic obstructive pulmonary disease (COPD) over the last 20 years. Treatment comprised of inhaled salmeterol/fluticasone propionate and short courses of prednisolone once or twice per year, typically administered over 4 weeks, starting at 20–30 mg/day and rapidly tapered to 5 mg/day.
At initial examination, the patient’s best corrected visual acuity (BCVA) was 6/7.5 in the right eye and 6/15 in the left eye. Intraocular pressure (IOP) was 10 mmHg and 5 mmHg, respectively. Anterior segment examination of the left eye revealed mixed conjunctival and ciliary injection, fine inferior keratic precipitates, anterior chamber cells and flare, fibrin formation with a small posterior synechia, and mild nuclear cataract (Fig. 1A, B). In the posterior segment, there was moderate vitritis with yellow-white condensations inferiorly. Fundoscopy through hazy media did not show any chorioretinal abnormalities. Examination of her right eye was unremarkable except for minimal nuclear cataract and a few macular drusen.
Fig. 1
Anterior segment photographs of the left eye at presentation. (A) Note the marked injection of the eye and the mild nuclear cataract. (B) Closer view of the anterior chamber shows some fibrin and posterior synechia
Complete blood count and biochemistry results were normal, apart from slightly elevated C-reactive protein level of 13 mg/L (reference < 5 mg/L). Urinalysis and culture performed shortly prior to admission were negative. Computed tomography (CT) of the head and brain showed normal sinuses and no evidence of fungal infection or malignancy. A comprehensive evaluation by an ear, nose and throat specialist, including rhinoscopy, revealed no evidence of sinusitis or upper respiratory tract infection. On chest CT and X-ray, bilateral infiltrates, basal condensations, and bronchiectasis consistent with pneumonia and COPD were observed. Whole-body positron emission tomography (PET)/CT showed a few pulmonary foci suggestive of active pneumonia. Transthoracic echocardiography demonstrated normal valves without vegetations. Repeated blood cultures were all negative. Bronchoalveolar lavage fluid showed growth of Haemophilus influenzae, but was negative by both microscopy and culture for fungi and mycobacteria.
Three days after admission, BCVA in her left eye was reduced to 6/30, and a core vitrectomy, followed by intravitreal injection of vancomycin 1 mg and amphotericin B 5 µg, was performed. No inflammatory lesions or thickening of the anterior choroid and ciliary body were observed during the vitrectomy. Microscopic examination of the vitreous showed inflammatory cells including macrophages and granulocytes, and the presence of fungal hyphae (Fig. 2A). Atypical lymphoid cells were not observed. Targeted amplification by polymerase chain reaction of the V2-V3 region of bacterial 16 S ribosomal deoxyribonucleic acid (16 S rDNA) was negative. Targeted amplification of fungal DNA targets, namely, internal transcribed spacers 1 and 2 (ITS1 and ITS2) and D1-D2 region of 28 S rDNA, were present. The sequence of D1-D2 region of 28 S rDNA could not differentiate between Fonsecaea and Cladophialophora species. However, sequences of ITS1 and ITS2 identified the microbe correctly to its species level as Cladophialophora devriesii. She was started on intravenous liposomal amphotericin B 150 mg (3 mg/kg) once daily and oral itraconazole 200 mg twice daily. She also received oral cotrimoxazole for a probable Haemophilus influenzae pulmonary infection. Culture of the vitreous sample demonstrated grey-black colonies after one week of incubation and their morphology and microscopic findings were consistent with Cladophialophora species (Fig. 3A, B). The ITS2 sequence obtained from the colonies was identical to that obtained from the sample. Then, the first intravitreal injection of 75 µg voriconazole was given. The eye gradually became less inflamed and BCVA improved to 6/12. A second intravitreal injection of voriconazole was given 10 days later. After two weeks on systemic amphotericin B and itraconazole treatment, her antifungal medication was changed to oral voriconazole 200 twice daily. During the following days, she complained of nausea, dizziness, and fatigue and appeared slightly confused. Brain CT was normal and transoesophageal echocardiography showed normal valves. Voriconazole-related side effects were suspected, and her medication was switched back to oral itraconazole 200 mg twice daily. At follow-up examination four weeks later, the eye showed no signs of inflammation, but progression of nuclear cataract was observed. The results of antifungal susceptibility testing by E-test were available from our reference laboratory about six weeks after the vitreous sampling and showed that posaconazole had the lowest minimum inhibitory concentration (MIC) value (0.008 mg/L) (Table 1). Her antifungal therapy was switched to oral posaconazole 300 mg daily. Despite troublesome side effects, such as myalgia, dry cough, and subjective hearing impairment, she continued this treatment for a total of 12 months. Whole-body PET/CT showed no signs of fungal infections, including pneumonia, at this stage. Examination of the left eye revealed nuclear cataract, otherwise both eyes were quiet without injection, anterior chamber cells, and vitritis (Fig. 4A, B).
Fig. 2
(A) Cytopathological examination of the vitreous specimen reveals fungal hyphae together with inflammatory and degenerated cells (Papanicolaou stain). (B) Histopathology of the enucleated eye reveals fungal hyphae located at the posterior lens capsule. The lens fibres are seen to the left of the vertically oriented posterior lens capsule (Periodic acid-Schiff stain). (C) Clusters of hyphae and conidia surrounded by inflammatory cells and cellular debris close to the ciliary processes, which are seen in the lower part of the image (Grocott methenamine silver stain). (D) At higher magnification, further details are revealed (Periodic acid-Schiff stain)
Fig. 3
(A) Culture on Sabouraud dextrose agar shows growth of small, grey-black colonies after one week of incubation. (B) Lactophenol cotton blue preparation of the colony material shows septate hyphae with solitary and short chains of ellipsoidal to fusiform conidia consistent with Cladophialophora species
Table 1 Minimum inhibitory concentration values of various antifungals against Cladophialophora devriesii isolates obtained from vitreous samples taken at admission (Isolate 1) and more than 3 years later (Isolate 2)Fig. 4
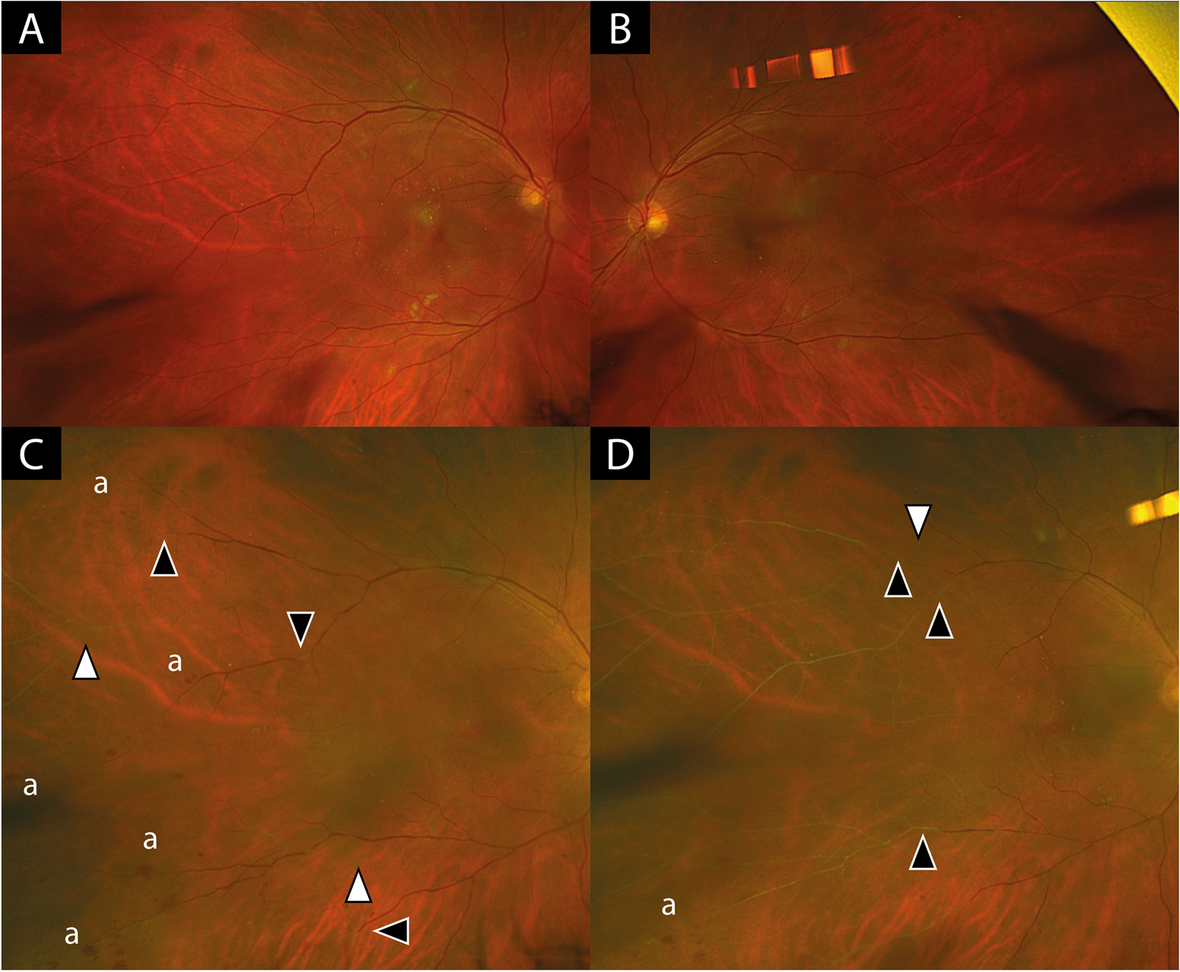
Fundus photographs of (A) the right eye and (B) the left eye taken during the course of treatment. Small drusen temporal to the macula are seen in both eyes. There are no inflammatory chorioretinal lesions or infiltrates in the left (endophthalmitis) eye
After three months without any antifungal medication, the patient noted increasing redness and pain in the left eye. Her BCVA was 6/38 and IOP was 4 mmHg. The eye was injected with keratic precipitates, anterior chamber cells and flare, extensive posterior synechiae, and marked nuclear cataract precluding clear fundus viewing. Repeated haematological, biochemical, and radiological investigations were all negative. She underwent a vitreous tap with intravitreal injection of 5 µg amphotericin B and was started on oral posaconazole 300 mg daily, as well as topical steroids and cyclopentolate. Intravitreal injection of amphotericin B was repeated after one week, followed by intravitreal injection of 100 µg voriconazole. Microscopy, cultures, and sequencing results of the vitreous sample were negative for fungi and bacteria. Redetermination of MIC by broth dilution method was then performed at the Statens Serum Institut in Denmark, using the fungal isolate cultured from the initial sample (taken 16 months earlier), and markedly different results were obtained (Table 1). Posaconazole was replaced by oral isavuconazole 200 mg daily, but after about six weeks, her medication had to be switched back to posaconazole 300 mg daily due to limited drug availability. After a further 18 months on oral posaconazole, the eye showed no signs of active inflammation, and once again an attempt to discontinue her antifungal medication was made. At follow-up examination three months later, the left eye was white, but a significant increase in anterior chamber cells and flare was observed. There was also a marked progression of the nuclear cataract and almost complete posterior synechiae (Fig. 5A, B). Visual acuity was reduced to finger counting at 2 m and IOP was 14 mmHg. Another vitreous sample, taken more than three years after the initial identification of Cladophialophora devriesii, revealed growth of the same fungus with identical ITS2 sequence. MIC values by E-test of this isolate, performed at our reference laboratory, were slightly different from the corresponding values of the initial isolate, but did not indicate development of resistance to triazole derivatives (Table 1). She was started on isavuconazole 200 mg daily in addition to topical steroids and cyclopentolate. During the following two weeks, the eye remained inflamed and she developed seclusio pupillae, which subsequently led to iris bombé and painful secondary glaucoma with an IOP of 45 mmHg. Due to the duration and severity of the infection, the eye was finally enucleated. Histopathologic examination of the enucleated eye revealed the presence of fungal hyphae and conidia close to the ciliary processes and the posterior lens surface (Fig. 2B–D). During three years of follow-up, the patient has been in good condition without any signs of systemic fungal disease.
Fig. 5
Anterior segment photographs of the left eye taken at recurrence more than three years after initial presentation. (A) Note the lack of injection, the secluded pupil, and the dense nuclear cataract. (B) Closer view of the anterior chamber shows extensive posterior synechiae and pigment deposits on the lens surface
Comments (0)