
Remember me


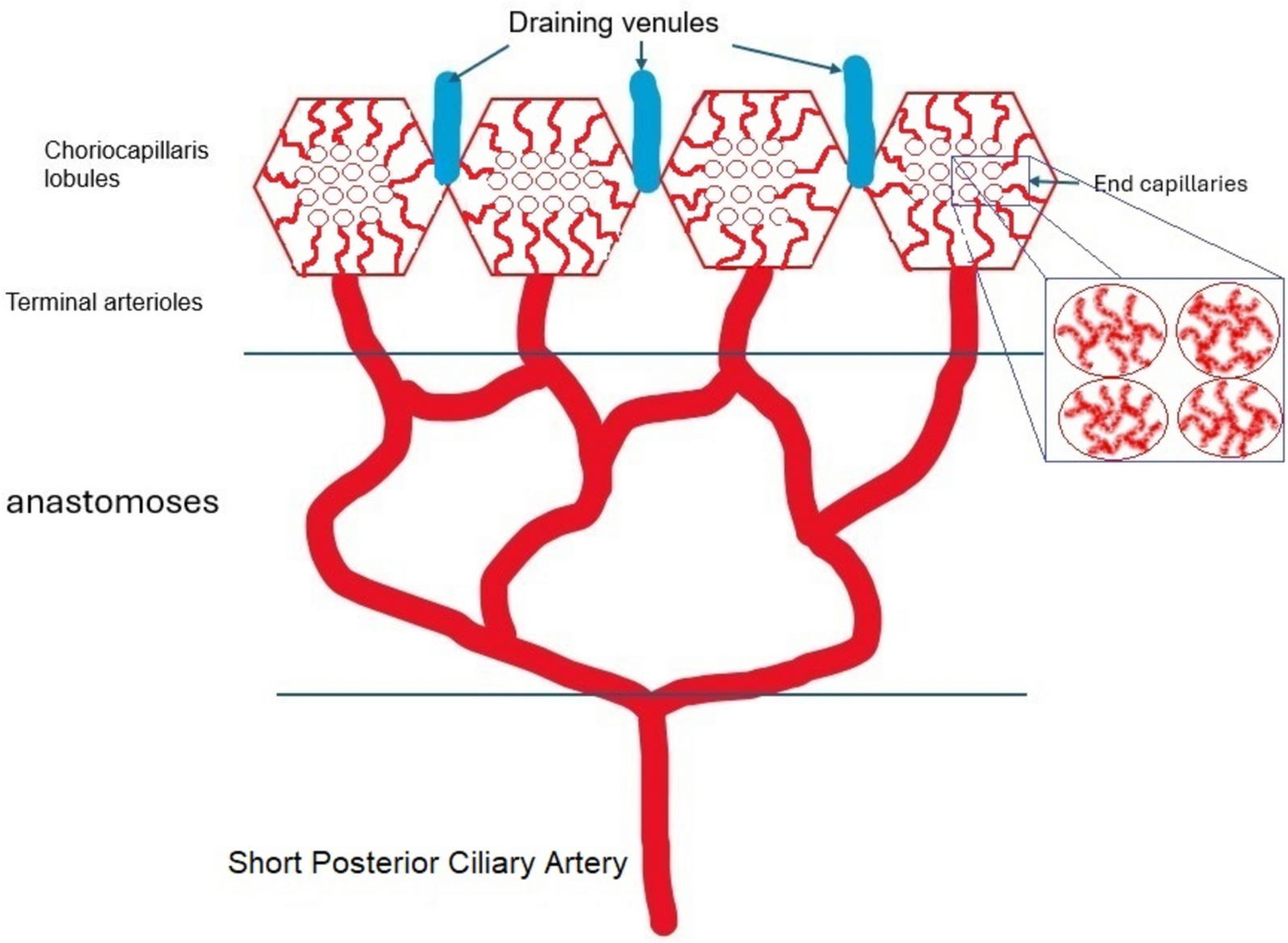


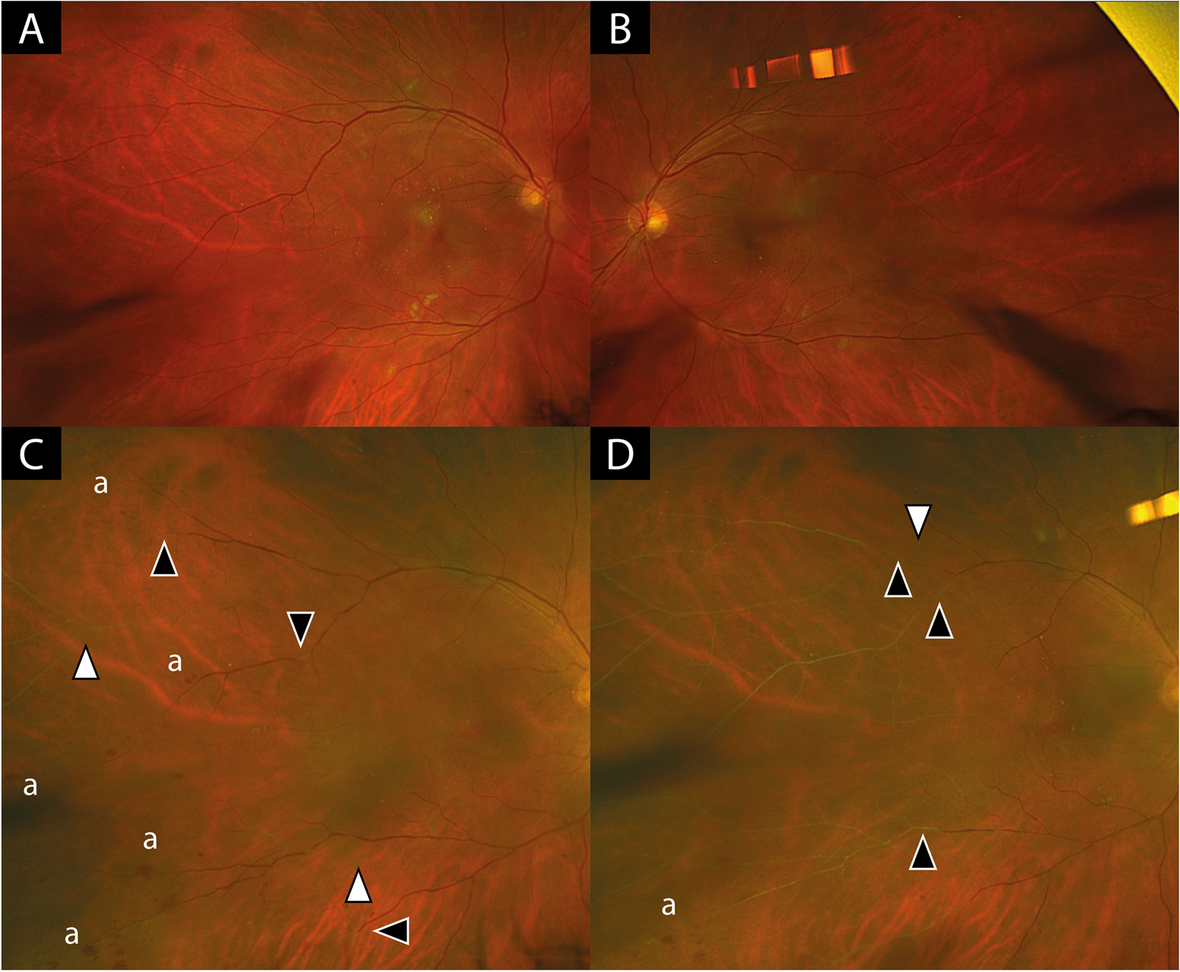

Table 1 lists and classifies non-infectious choroidal vasculitis.
Table 1 Classification of non-infectious choroidal vasculitisPrimary choroidal vasculitisPrimary choriocapillary vasculitis (choriocapillaritis)As mentioned before the choriocapillaris is a lobular mesh with a central arteriolar feeder. This anatomic characteristic explains the pattern of choriocapillaritis/choriocapillary vasculitis seen on ICGA. Indeed, choriocapillaritis/ choriocapillary vasculitis appears as scattered or geographic areas of hypofluorescence, indicating the lobe that is not perfused. Depending on the localization of the inflammation, in the arterial tree, there is a diverse severity of extension and involvement (Fig. 14). Very often there is a generalised choriocapillaris perfusion delay on the early frames in the area where choriocapillaris non-perfusion is seen on the late frames (Figs. 15 and 16).
Fig. 14
Cartoon showing choriocapillaris architecture. Depending on the size of the inflamed vessels, choriocapillaris inflammatory non-perfusion ranges from small hypofluorescent dots when endcapillary vessels are involved as in MEWDS to large hypofluorescent areas in case of MFC, APMPPE or SC
Fig. 15
MEWDS. Young lady presenting faint visual disturbance. Typical hypofluorescent dots of non-perfusion scattered all over the posterior pole and mid-periphery in the late ICG angiographic phase. Interestingly there is an additional circulatory disturbance in delayed choriocapillaris perfusion on early FA frames and less so on ICGA beyond the temporal arcades, (2 top frames)
Fig. 16
MEWDS. Young man presenting a faint subjective scotoma, Right frame: scattered areas of small dark dots representing choriocapillaris non-perfusion co-localized with FAF hyperautofluorescence caused by secondary photopigment loss (bottom left) and associated with choriocapillaris perfusion delay (top left, yellow arrows)
Choriocapillary vasculitis/choriocapillaritis at the origin of Multiple evanescent white dot syndrome (MEWDS)MEWDS is considered as the mildest form of primary choriocapillaritis / choriocapillary vasculitis, affecting the end-capillary vessels of the choriocapillaris. The disease is usually unilateral. The cause is clearly localised end-capillary hypo-perfusion and/or non-perfusion of the choriocapillaris and not primary photoreceptor disease [9] (Fig. 5). Secondary alterations of the outer retina are detected by SD-OCT corresponding to the dark hypofluorescent dots on ICGA precisely identifying the small scattered non-perfusion lesions. Corresponding hyperautofluorescent areas are attesting the secondary loss of photopigment of the outer retina. The vasculitic process in MEWDS is analysed in a few illustrative cases hereafter.
Illustrative case of the type of choriocapillaris vasculitis present in MEWDS
This 33-year-old lady consulted for visual disturbance of her left eye and reported to see shadows and glistening of surfaces, retaining, however, full visual acuity and discreet visual field impairment. Early FA and ICGA frames showed disturbed choriocapillaris perfusion with delay in some areas. The late ICGA frame showed numerous small non-perfusion area. It seems therefore, taking into account of the early perfusion anomalies seen in this case, (Fig. 15) that there is a more widespread perfusion problem in MEWDS apart from the typical small hypofluorescent non-perfused dots.
Circulatory disturbances in a case of MEWDS
This 27-year-old man complained of a subjective scotoma in his right eye with minimal visual field impairment and typical ICGA vasculitis findings of small areas of choriocapillaris non-perfusion on the late frames associated with more general choriocapillaris perfusion delay during the early frames (Fig. 16).
Case of MEWDS showing asymmetry between FAF and ICGA
This MEWDS case shows asymmetry of FAF and ICGA lesions suggesting that hyperautofluorescent areas seem to be maximal in areas where ICGA is comparatively less intense probably indicating re-perfusion whereas in other regions ICGA is intensively dark compared to less pronounced FAF hyperautofluorescence indicating that non-perfusion is preceding and present before consequent secondary damage to photoreceptor occurs (FAF-hyperautofluorescence) (Fig. 17a). SD-OCT at presentation passing through one of the darker lesions in ICGA showed hyperreflectivity of the outer segment and disruption of IS/OS (Fig. 17b).
Fig. 17
a Discrepancy between ICGA and FAF images indicating that end-choriocapillary non-perfusion is at the origine of photoreceptor damage. Left frame: autofluorescence of a patient diagnosed with MEWDS. The lesions nasally to the optic disc (yellow arrows) demonstrate established outer retinal damage (marked hyperautofluorescence) while the lesions temporal to macula (red arrows) are less marked. Comparing to the ICGA (right frame) it is noticed that the lesions nasally to the ON (green arrow) are less hypofluorescent (probably due to reperfusion) than the lesions temporal to the macula which are darkly hypofluorescent (crimson arrows). Probably the lesions nasally to ON are older lesions that already affected the outer retina as seen in FAF. The temporal lesions are fresher with the outer retina damage not yet completely established. This comparison can explain why MEWDS is a primary choriocapillaritis / choriocapillary vasculitis and not a photoreceptoritis as the hypoperfusion precedes the outer retina damage. b Comparison of SD-OCT at presentation (top image) and in 6 weeks follow-up (bottom image). OCT through one of the lesions (seen hypofluorescent in ICGA) showing hyperreflectivity and disruption of the IS/OS (yellow arrows, top picture). After 6 weeks, without any treatment, OCT showed improvement (red arrow, bottom picture)
Acute posterior multifocal placoid pigment epitheliopathy (APMPPE)APMPPE also belongs to the group of primary choriocapillaritis / choriocapillary vasculitis entities. It is called primary because the trigger is also unknown. The name is a misnomer as the lesion process was attributed to the retinal pigment epithelium (RPE) when first described by Don Gass [18]. The pathophysiological explanation was reoriented, thanks to ICGA, towards the exact explanation of the disease process, namely inflammatory choriocapillaris vasculitic non-perfusion. Deutman had already understood the exact disease mechanism before the availability of ICGA. He had mentioned that in the early FA frames of APMPPE, there was perfusion delay of the choriocapillaris and he suggested the more appropriate denomination of the disease by calling it Acute Multifocal Ischaemic choriocapillaritis (AMIC) [13, 19] Indocyanine green angiography (ICGA) later confirmed the theory of choriocapillaris perfusion disturbance, showing that the perfusion delay described by Deutmann was not only a perfusion delay but choriocapillaris non-perfusion as the dark non-perfused areas remained until late angiographic frames [10].
In APMPPE/AMIC, inflammatory non-perfusion is bilateral and affects larger choriocapillaris or pre-choriocapillaris vessels than in MEWDS. Therefore, the areas of hypoperfusion are more extended and coalescent. It was considered to be a self-resolving condition, but later studies established that treatment with systemic corticosteroids was necessary, especially in cases with extended macular involvement [20]. APMPPE is a vasculitis affecting the choriocapillaris and is sometimes associated with cerebral vasculitis. ICGA can demonstrate choriocapillaris vasculitis as will be shown in the illustrative cases reported below. FA can demonstrate the choriocapillaris non-perfusion in the first 60 s of the angiogram which corresponds to the hypofluorescent areas seen on the ICGA up to late frames (Fig. 18).
Fig. 18
Correlation of late ICGA phases with early FA phases in APMPPE. a ICGA late phase demonstrated geographic area of non-perfusion of the choriocapillaris. The lesions correlate well with those seen in early stages of FA. b It is on these FA images that Deutman elaborated his correct interpretation of the disease process in APMPPE
Case of APMPPE
A 25-year-old female patient presented with bilateral scotomas and vision loss. Fundus examination showed diffuse scattered white lesions in the posterior pole and mid-periphery. FA in the early angiographic phase and ICGA in the intermediate-late phases showed hypofluorescent areas of choriocapillaris non-perfusion (Fig. 19a).
This patient’s clinical case gave a very precious insight into the potential vascular pathophysiology of APMPPE as shown by ICGA (Fig. 19b/A). High magnification of ICGA angiographic frames of the intermediate phase showed that in the close vicinity adjacent to many hypofluorescent non-perfusion areas there were often punctiform or elongated hyperfluorescent structures probably indicating an inflamed vessel at the origin of the hypofluorescent areas of choriocapillaris non-perfusion (Green arrows in Fig. 19b/B).
Fig. 19
a Fundus appearance of APMPPE. Multiple bilateral placoid lesions. b/A. ICGA image of same patient as 19a. Numerous geographic areas of hypoperfusion. Note that the stromal vessels are minimally involved and can be well distinguished outside the choriocapillaritis APMPPE lesions (A general view; Intermediate phase of the ICGA of the RE of a patient with APMPPE. We note the hypofluorescent areas corresponding to the non-perfusion of the choriocapillaris. b/B. Same APMPPE patient as in 19a & 19b/A. B) Blow-up of part of the global view A, zoomed on the posterior pole. Green arrows pinpoint multiple hyperfluorescent spots or lines, adjacent to the areas of the hypoperfusion, showing vasculitis of the choriocapillaris vessel corresponding probably to the vasculitic occluded feeding vessel of the hypofluorescent dark lobules
Case of APMPPE
This 28-year-old patient consulted for bilateral photopsias and subjective scotomas. Fundus examination showed multiple posterior pole and mid-periphery placoid lesions. On ICGA these lesions corresponded to numerous sometimes coalescent dark areas of choriocapillaris non-perfusion indicating larger vessel involvement. OCT-A showed large areas of choriocapillary drop out with absence of flow (Fig. 20a). This is in contrast with MEWDS, where circulatory impairment involves end-capillary choriocapillaris with reduced flow that cannot be detected by OCT-A. Consequently OCT-A is unable to determine whether there is end-choriocapillary closure and complete absence of flow which can only be detected by ICGA (Fig. 20b).
Fig. 20
a APMPPE. Young male patient complaining of subjective scotomas and photopsias presenting widespread geographic and confluent areas of hypofluorescent non-perfused areas, precisely delineated on ICGA. The lesions in the posterior pole are also detected by OCT-A, showing the areas of choriocapillary drop-out. OCT-A is very useful for non-invasive follow-up of lesions, being however limited to the posterior pole. b MEWDS. Young male patient who consulted for unilateral photopsias and subjective scotomas. ICGA (left) shows numerous limited areas of end-choriocapillary non-perfusion that, in contrast to APMPPE (Fig. 20a) do not appear as drop-out areas on OCT-A (right) because OCT-A does not detect slow flow perfusion and therefore cannot show its drop-out
Idiopathic Multifocal Choroiditis (MFC)The vasculitic process in MFC is comparable to that of MEWDS. Indeed, it is not rare to make the diagnosis of MEWDS at the time of the first episode of MFC. The findings are absolutely similar to MEWDS (Fig. 21). It is only when a second inflammatory episode occurs that the diagnosis has to be rectified. MFC is a recurrent disease ultimately affecting both eyes and characterized by chorioretinal scars, which is not the case of MEWDS that is unilateral, usually limited to one episode and does not produce scars. The severity of MFC is very diverse but the inflammatory non-perfusion of the choriocapillaris is often prolonged and widespread, the consequent ischemia being at the origin of the scars and of choroidal neovascular membranes that develop in up to 30% of cases [21]. MFC very often needs aggressive immunosuppressive treatment [21].
Fig. 21
Multifocal choroiditis (MFC). Case of bilateral MFC, active in the left eye (top left) and inactive in the right eye (bottom left) with only chorioretinal scars but no vasculitis of the choriocapillaris. Fundus pictures (bottom right) show bilateral scars but do not allow to determine whether the disease is active. The widespread occult choriocapillaris vasculitis is shown by ICGA (top left), which is absolutely not suspected on FA (3 top right frames)
Serpiginous choroiditis (SC)SC is the most severe form of choriocapillaritis involving larger and progressing areas of non-perfusion probably due to vasculitis of larger choriocapillaris vessels or pre-choriocapillary arterioles [22]. One possible trigger of SC is due to Mycobacterium tuberculosis which has to be excluded by performing an interferon-gamma release assay (IGRA). In case of IGRA negativity the condition is called idiopathic SC which needs dual to triple immunosuppressive treatments to halt the progression of the disease.
Illustrative case of idiopathic SC
This 64-year-old patient had been treated on and off with systemic corticosteroids for several years with, however regular progression of the serpiginous lesions (Fig. 22). An IGRA test was negative, indicating that the patient had never been exposed to Mycobacterium tuberculosis, the diagnosis being thus the idiopathic form of SC. The initiation of a combined immunosuppressive therapy including systemic corticosteroids, azathioprine and cyclosporin allowed to halt the progression of the disease.
Fig. 22
Serpiginous choroiditis. Non-perfusion in SC involves larger choriocapillaris vessels and produces extended areas of non-perfusion leading to chorioretinal atrophy if treatment is not initiated promptly. ICGA clearly delineates atrophic in addition to non-perfused areas (yellow arrow on ICGA frame), whereas FA only shows atrophic areas but not non-perfused areas (yellow arrow on FA frame). In addition, ICGA shows perilesional hyperfluorescence (dark blue arrows) indicating possible disease activity
Primary stromal choroidal vasculitisThe most characteristic sign of stromal choroiditis on ICGA is the presence of HDDs. These choroidal foci represent an inflammatory process taking its origin within the choroidal stroma which, logically, generates and is accompanied by inflammation of the stromal choroidal vessels. In contrast to choriocapillaris vessels which are fenestrated, these larger stromal vessels are impermeable in a normal non-inflammatory situation. In case of choroiditis these vessels become leaky and allow ICG to egress rendering the vascular pattern fuzzy in the intermediate angiographic phase and does not allow to see the normal course of the choroidal vessels in the late phase because of the abnormal ICG coming from inflamed larger vessels, adding to the physiological egression of ICG from the choriocapillaris fenestrations causes late diffuse hyperfluorescence [23]. Because the lesion process is originating from within the choroid, involvement is quite uniform in all the fundus areas with evenly distributed HDDs and diffuse hyperfluorescence. Vogt-Koyanagi Harada disease (VKH), Sympathetic Ophthalmia (SO) and HLA-A29 Birdshot Retinochoroiditis (BRC) are considered as primary stromal choroiditis entities because the inflammatory process starts from within the choroidal stroma.
Choroidal stromal vasculitis in VKH diseaseIn VKH, histopathologic evaluation reveals thickening of the choroid with stromal cellular inflammation constituted by macrophages, lymphocytes, and epithelioid cells containing melanin, as the consequence of an autoimmune process directed against melanin-associated proteins within choroidal stromal pigmented islets. The presence of evenly sized and evenly distributed HDDs is the characteristic finding by ICGA in VKH. The process is at first limited to the choroidal stroma before spilling over secondarily to neighbouring structures such as the retina and optic disc. VKH can therefore be considered as a purely stromal choroiditis, as inflammation starts exclusively in the choroidal stroma [24]. The consequence of the choroidal autoimmune infiltration is the presence of choroidal vasculitis evidenced by ICGA and characterised by individualised early hyperfluorescent choroidal vessels, general staining of large choroidal stromal vessels making them appear fuzzy in the intermediate angiographic phase followed by diffuse hyperfluorescence that overshadows HDDs less well discernible in the late phase. Other ICGA signs include disc hyperfluorescence rarely seen on ICGA unless choroidal inflammation is pronounced which is the case in VKH and ICGA hyperfluorescent pinpoints marking points of leakage from the choroid at the origin of the serous retinal detachments (Figs. 23, 24 and 25).
Fig. 23
a Choroidal vasculitis in VKH disease, intermediate angiographic phase. Pronounced choroidal vasculitis is present overshadowing HDDs barely detectable (top 2 sets of 9 frames). After treatment (bottom 2 sets of 9 frames) the normal pattern of choroidal vessels are again clearly identifiable with resolution of HDDs. b Choroidal (ICGA) vasculitis in VKH disease, late angiographic phase. Pronounced choroidal vasculitis with late hyperfluorescence obscuring the normal pattern of choroidal vasculature (top 2 sets of 9 frames). After treatment, the normal vascular pattern is again identifiable, in negative, as there is no ICG dye any longer within the circulation (bottom 2 sets of 9 frames). c VKH ICGA mid-phase (10’). c/a) At presentation, we notice marked choroidal vasculitis (green arrows) as well as choroidal ischemia (red arrow). The inflammation was such that the patient developed choroidal detachment (blue arrow). c/b) After treatment there is improvement of the choroidal vasculitis (yellow arrows) and reperfusion of the choroid
Fig. 24
Choroidal vasculitis in VKH disease. Early angiographic phase showing early hyperfluorescent vessels (arrows) and ICGA disc hyperfluorescence only seen on ICGA in hyperacute inflammation
Fig. 25
Choroidal vasculitis in VKH disease, EDI-OCT thickening of the choroid. At the early stage of VKH, there is pronounced choroidal thickening barely measurable (top image), gradually returning to normal thickness after treatment (bottom image)
Choroidal stromal vasculitis in Sympathetic OphthalmiaThe disease process is similar to VKH. The autoimmune reaction is thought to be triggered by the exciting eye that has suffered a penetrating injury or multiple intraocular surgeries. Therefore, the angiographic findings are comparable to VKH disease, being usually, however, less severe [25] (Fig. 26).
Fig. 26
Stromal vasculitis in Sympathetic Ophthalmia. This 24-year-old Indian lady had undergone vitrectomy followed by cataract operation and filtering surgery in her right eye.Two months after the last surgery VA in her left eye decreased and laser flare photometry indicated subclinical anterior chamber inflammation with flare amounting to18.2 ph/ms. Intermediate phase ICGA showed numerous HDDs and choroidal stromal vasculitis (top 2 frames). Late panorama frames (bottom 9 frames) showed substantial choroidal stromal vasculitis with persistent HDDs and some evanescent HDDs in the posterior pole indicating partial thickness foci. All angiographic signs resolved after introduction of systemic corticosteroid, Mycophenolate and Infliximab therapy
Choroidal stromal vasculitis in HLA-A29 Birdshot retinochoroiditis (BRC)BRC is a presumptive autoimmune condition involving both the retinal and the choroidal compartments. Unlike in VKH disease which is a purely stromal choroiditis, in BRC inflammation develops concomitantly in parallel in the retina showing a pathognomonic vasculitis (Fig. 27) and in the choroid which distinguishes it from VKH disease [26]. Nevertheless, the choroidal involvement is a genuine stromal choroiditis (Figs. 28 and 29a). Thus, ICGA signs of vasculitis in BRC are comparable to VKH disease, although less severe. Early hyperfluorescent vessels and disc hyperfluorescence are rarely seen. As for VKH disease the presence of HDDs is a prominent feature associated with choroidal vasculitis. However choroidal infiltration is often of partial thickness explaining that in the late ICGA angiographic frames HDDs have a tendency to fade (Fig. 29b).
Fig. 27
Retinal involvement in BRC. Retinal vasculitis is a constant finding in BRC and develops concomitantly to stromal choroiditis. Diffuse bilateral retinal vasculitis is present in 100% of BRC and is an early occurrence. It is characterised by a very leaky vasculitis of small and large vessels with profuse exudation, macular oedema often sparing the fovea, thick FA sheathing/staining of large posterior pole vessels, arterio-venous circulatory pseudo-delay, and pronounced disc hyperfluorescence
Fig. 28
BRC choroidal vasculitis in a case of moderate severity. Posterior pole involvement is seen in the left quartet of frames (left), in the intermediate and late frames, normal choroidal vasculature is less well recognizable; note that HDDs are fading away on the late frame, indicating partial thickness of choroidal infiltrates. On panfundal intermediate and late frames (middle and right sets of 9 frames) peripheral choroidal vasculitis is minimal, as both intermediate and late angiographic phases, the normal vascular pattern is identifiable. Note the fading away of HDDs in the late angiographic phase (right set of 9 frames), indicating partial thickness lesions
Fig. 29
a BRC choroidal vasculitis in a case of pronounced severity.Numerous HDDs are seen in the intermediate phase (left set of 9 frames) remaining until late phase (right 9 frames). However, choroidal stromal vasculitis is usually always less than in VKH disease, as choroidal vessel pattern is still identifiable in both intermediate and late phases. b Partial thickness HDDs. Top 2 frames and corresponding cartoon on right: In the intermediate angiographic phase (top left) of this BRC case, numerous HDDs that fade away in the late angiographic frame (top middle), corresponding to partial thickness lesion as illustrated on cartoon on the right. Bottom 2 frames and corresponding cartoon on the right: HDDs visible in the intermediate angiographic phase (bottom left) still visible in the late angiographic frame (bottom middle) corresponding to full thickness lesion as illustrated on the corresponding cartoon on the right
Secondary choroidal vasculitisSecondary choriocapillary vasculitis / choriocapillaritis Acute Syphilitic Posterior Placoid Chorioretinitis (ASPPC)Acute Syphilitic Posterior Placoid Chorioretinitis (ASPPC) is one of the disease expressions caused by ocular syphilis. It is not a direct infectious process but an immunologic reaction triggered by Treponema Pallidum causing secondary non-perfusion of the choriocapillaris [27,28,29]. It has been shown that such an expression of syphilitic eye disease can be suppressed by corticosteroid therapy indicating the immunologic component of this condition [30]. However, a definitive cure of the disease can only be achieved by appropriate antibiotic therapy.
Case report illustrating choriocapillaris non-perfusion in ASPPC
This 27-year-old lady had been suffering from angina which was followed by a decrease of visual function in form of dim vision and subjective scotomas. At presentation visual acuity was reduced to 0.6 RE and 0.5 LE. There was subclinical anterior chamber inflammation detected by laser flare photometry amounting to 14.7 ph/ms OD and 8.3 ph/ms OS (normal values = 4–6 ph/ms). OCT showed bilateral cystoid macular oedema and extended areas of loss of outer photoreceptor segments corresponding to areas of hyperautofluorescence on fundus autofluorescence frames. FA showed bilateral retinal vasculitis, cystoid macular oedema and disc hyperfluorescence. ICGA showed extensive areas of geographic hypofluorescence indicating widespread choriocapillaris non-perfusion. Syphilis serology yielded an elevated VDRL test and elevated TPHA (treponema pallidum hemagglutination assay) serology. After antibiotic treatment (Ceftriaxone 2000 mg/day IM for 14 days) all the hypofluorescent areas of non-perfusion were again re-perfused (Fig. 30).
Fig. 30
Acute Syphilitic Posterior Placoid Chorioretinitis (ASPPC). At presentation (2 left frames) numerous geographic areas of hypofluorescence are present on ICGA delineating the extensive choriocapillaris vasculitis producing choriocapillaris non-perfusion, which is co-localized with fundus hyperautofluorescence (FAF, right top 2 frames) indicating photoreceptor outer segment loss. On the middle and bottom left 2 frames all the non-perfused areas have recovered after treatment
Tuberculosis related serpiginous choroiditisSimilar to syphilis, tuberculous ocular involvement can be twofold. It can take the form of direct infectious chorioretinitis or can present as a predominantly immune process causing tuberculosis-related multifocal/serpiginous choroiditis. In all forms of multifocal/serpiginous cases an Interferon-Gamma- Release Assay (IGRA) should be performed. In case the IGRA test is positive, the condition should be considered as a tuberculosis related immune form of serpiginous to be distinguished from idiopathic serpiginous choroiditis [31]. As for ASPPC, the mechanism consists of an immune-mediated choriocapillaris non-perfusion. The level of involvement in the vascular tree is more proximal than other choriocapillaris entities and involves larger vessels, producing extended ischemia. It is non-reversible and leaves choriorertinal scars if not treated in time. Adequate treatment consists of concomitant dual multiple anti-tuberculous antibiotic treatment and multiple immunosuppressants.
Illustrative case of choriocapillary vasculitis/ choriocapillaritis in tuberculosis-related serpiginous choroiditis
This 35-year-old male patient had been treated for a bilateral chorioretinitis on and off systemic corticosteroids and on and off anti-tuberculous antibiotics because of a positive IGRA test. These treatments were, however, never given concomitantly. At presentation in our centre, ICGA a
Comments (0)