
Remember me





Pterygium is a prevalent ocular disease characterized by the development of triangular mucosal tissue on the ocular surface. The intricate relationship between pterygium and dry eye disease has long been a topic of study. Pterygium can cause ocular irritation, photophobia, and impaired tear stability [16]. Pterygium formation destabilizes the ocular surface by changing tear film dynamics, damaging conjunctival blood vessels, and altering meibomian glands [17]. Our research has revealed that the severity of pterygium is closely linked to the duration of tear film disruption. It is possible that the angle of tear evaporation may not be the underlying cause of the dry eye symptoms resulting from pterygium growth. This association is thought to be a result of structural changes brought on by pterygium growth, which can lead to an imbalance in the ocular surface [18], including tear secretion is reduced, tear film stability is compromised, evaporation is increased, epithelial cells deteriorate, tear osmolality rises, and goblet cell density decreases [19]. In this study, we showed a comprehensive evaluation of ocular surface parameters and structural integrity impacted by pterygium.
In healthy eyes, the conjunctiva and cornea maintain a stable relationship in both structure and function. However, the development of pterygium causes the conjunctival tissue to grow and extend onto the surface of the cornea, resulting in instability. This abnormal growth can cause eye irritation, redness, and a foreign body sensation [20]. Furthermore, it may disrupt the natural distribution of tears, which can lead to an uneven tear film on the eye surface and impact the eye’s protective function. Consequently, the eye can become more vulnerable to external factors like dry air and ultraviolet radiation [21]. Research has indicated that corneal abnormalities may play a role in the tear film’s instability within the eye [22]. Patients diagnosed with pterygium are likely to suffer from dryness and ocular discomfort due to the disturbance in the homeostatic balance and uneven distribution of tears, as demonstrated in various studies [23]. This may lead to pterygium patients with similar symptoms to patients with dry eye, further increasing eye discomfort. In this study, we found that pterygium had worse dry eye indicators than healthy eyes. In addition, pterygium patients were more destructive to the cornea and meibomian glands, but it had a more abundant LLT content than in patients with mild and moderately dry eyes. Therefore, the dry eye symptoms caused by the ocular surface structure and homeostasis changes of pterygium may not originate from the excessive evaporation of tears.
Studies have suggested that there may be several reasons for the shortening of tear breakup time, including impaired blink pattern, epithelial drying and subsequent reduction in NIBUT, and irregularity of the ocular surface epithelium, which disrupts tear film stability by impairing surface tension and stability [24]. It is crucial to consider other factors such as hyperpermeability, inflammation, and instability in the structure of the ocular surface in the pathogenesis of ocular surface imbalance caused by pterygium [25]. Previous studies have shown that pterygium is characterized by marked vascular responses and marked inflammatory infiltrates [26]. Pterygium can cause inflammation and significant damage to the corneal epithelial surface and conjunctiva. During an active phase, it may lead to changes in the ocular surface and tear film abnormalities when compared to eyes without pterygium (Fig. 1). Our observations suggest that pterygium growth can cause corneal conjunctival defects, changes in vascularity, and congestion, and the inflammation that causes these changes is often overlooked as a risk factor for pterygium.
Fig. 1
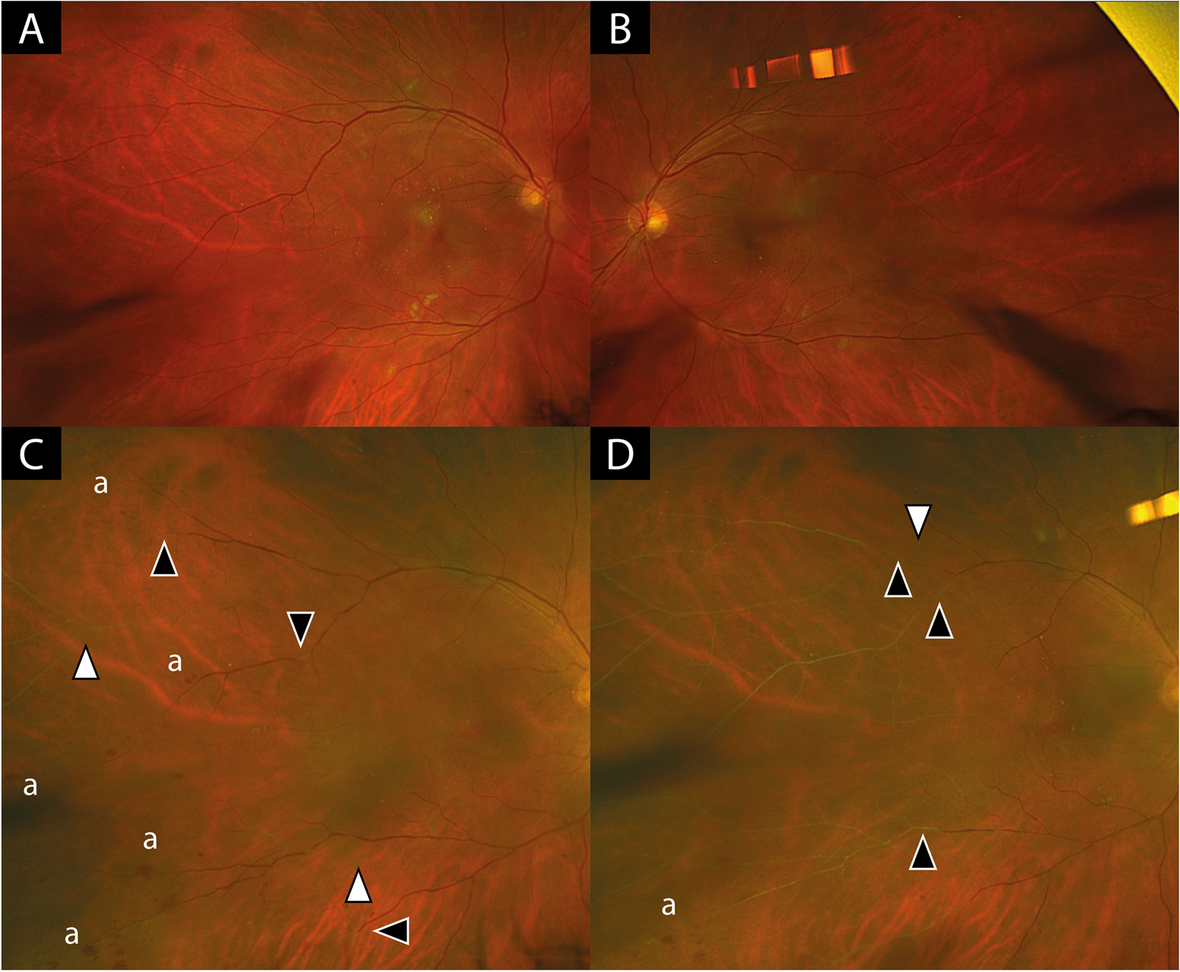
Relationship between pterygium and ocular surface homeostasis. (A) There may be an interactive relationship between pterygium growth and the imbalance of ocular surface homeostasis. When the irregular cornea, abnormal tear membrane and continuous inflammation may cause the growth of pterygium and the destruction of the ocular surface may lead to dry eye symptoms; (B and C) In the examination of tear membrane rupture, B shows abnormal tear break up time in the growth area, while C shows the lower half
Research has indicated that UV radiation can result in genetic alterations impacting the cytokines IL-6 and IL-8 expression in individuals with pterygium [27]. These cytokines promote the production of MMPs and are commonly detected in the anterior portion of the pterygium. The discharge of IL-6, IL-8, and MMPs into the tear film may cause harm to the ocular surface [28], resulting in instability of the tear film, loss of epithelial cells, lowered mucus secretion, and enhanced tear permeability [29]. Patients with pterygium will have disturbances in tear film quality and quantity, and the reduction of conjunctival goblet cells may lead to tear film instability. Studies have shown that the pterygium resection can significantly increase the average goblet cell density and increase the secretion of mucin in the tear film [30]. Therefore, we believe that tear hypertonicity and tear membrane dysfunction are associated with pterygium and influence each other through certain mechanisms, ultimately leading to the ocular surface homeostasis imbalance.
LT α is a protein complex composed of three identical LT α subunits that mainly act on regulatory T cells (Treg). Treg and protein-mediating factors are essential for maintaining immune balance [31]. Treg suppresses the immune system and promotes tissue repair. Tregs have been shown to play a beneficial role in tissue repair, goblet cell differentiation, mucin secretion, and suppression of Th1 and Th17 cell proliferation. LT α helps maintain ocular surface immune balance through the LT α tumor necrosis factor receptor 2 Treg axis [32,33,34]. Our study revealed the state of LT α in pterygium, indicating the inflammatory activity of pterygium. Based on the measurement of LT α in ocular surface tear film, we found that the concentration of LT α in tears of patients with pterygium decreased. The absence and decrease of LT α reflect a decrease in cell proliferation and tissue repair ability, a decrease in the number and function of goblet cells, and a decrease in mucin secretion [35]. When there is an immune imbalance, mucus secretion and goblet cells decrease, leading to apoptosis and shedding. Additionally, Th17 cells secrete IL-17, which promotes the secretion of various vascular endothelial growth factors, resulting in corneal lymphangiogenesis [36]. These immune responses involve both the ocular mucosa and the systemic immune response. squamous metaplasia of ocular surface epithelial cells caused by immune imbalance may be responsible for the active state [37]. This leads to immune cell entry into the ocular surface, which hinders Treg activity, further expanding and migrating Th17 and Th1 cells and exacerbating epithelial damage [38].
Immune cells such as macrophages, goblet cells in ocular surface tissue, and Tregs secrete important growth factors, cytokines, immune tolerance factors, antimicrobial enzymes, peptides, and mucins that are crucial for maintaining normal conjunctival epithelial tissue proliferation, differentiation, and function [39]. These factors are essential for ocular surface homeostasis, epithelial tissue density, repair, and other normal functions. Therefore, maintaining tear film quality, immune tolerance, and tissue repair are critical for maintaining eye surface immune homeostasis. In order to gain a complete understanding of the relationship between pterygium-induced structural changes in ocular surface structure and ocular surface homeostasis, additional histopathological studies are required. This study evaluated the clinical parameters of the ocular surface in individuals with pterygium and examined the correlation between pterygium status and ocular surface homeostasis (Fig. 2). Our findings indicate that changes in the ocular surface structure can compromise ocular surface homeostasis, and the “irregular” ocular surface resulting from pterygium warrants further investigation. This study compared the decrease of related dry eye indicators caused by pterygium with those of dry eye patients without pterygium. The limitation of this study is the need to further explore a confounding factor in the dry eye cohort in future studies, requiring further validation in more prospective studies. These results contribute to our understanding of the disease and provide a fresh perspective for future research.
Fig. 2
Pterygium causes an inflammatory reaction and LT α may serve as one of the inflammatory factors. Repetitive inflammation involved with ultraviolet (UV) combined with matrix metalloproteinases (MMPs) and vascular endothelial growth factor (VEGF) acts at the conjunctiva can cause the formation of pterygium. This abnormal growth triggers the release of inflammatory substances like IL-6, IL-8,IL-17, interferon gamma (IFN-γ) and tumor necrosis factor alpha (TNF-α) into the tears, causing an inflammatory reaction that destabilizes the tear film. Additionally, lower levels of LT α indicate impaired tissue repair on the eye’s surface. As pterygium advances, the reduction in goblet cells and tear mucin may be linked to the decreased LT α which The reduced ability of the activation of NF-kB leading to an impaired anti-inflammatory response from Treg / Th and / or M2 to reduce the IL-4, IL-10 as well as the immune regulatory function of IL-13 which to inhibit Th 1 and Th 17 leads to inflammation.This progression leads to a harmful cycle of immune inflammation and chronic irritation, ultimately disrupting the ocular surface balance
Comments (0)