
Remember me







The study population was drawn from the National Health and Nutrition Examination Survey (NHANES) database for eight consecutive periods from 2001 to 2016. NHANES is a cross-sectional study of multistage sampling conducted by the National Center for Health Statistics (NCHS) representing the current nutritional and health status of non-institutionalized civilians in states across the country [14]. The NHANES study was approved by the Ethics Review Committee of the National Center for Health Statistics with the written consent of each participant. Detailed survey design, sampling methods, and data are available on the website [15].
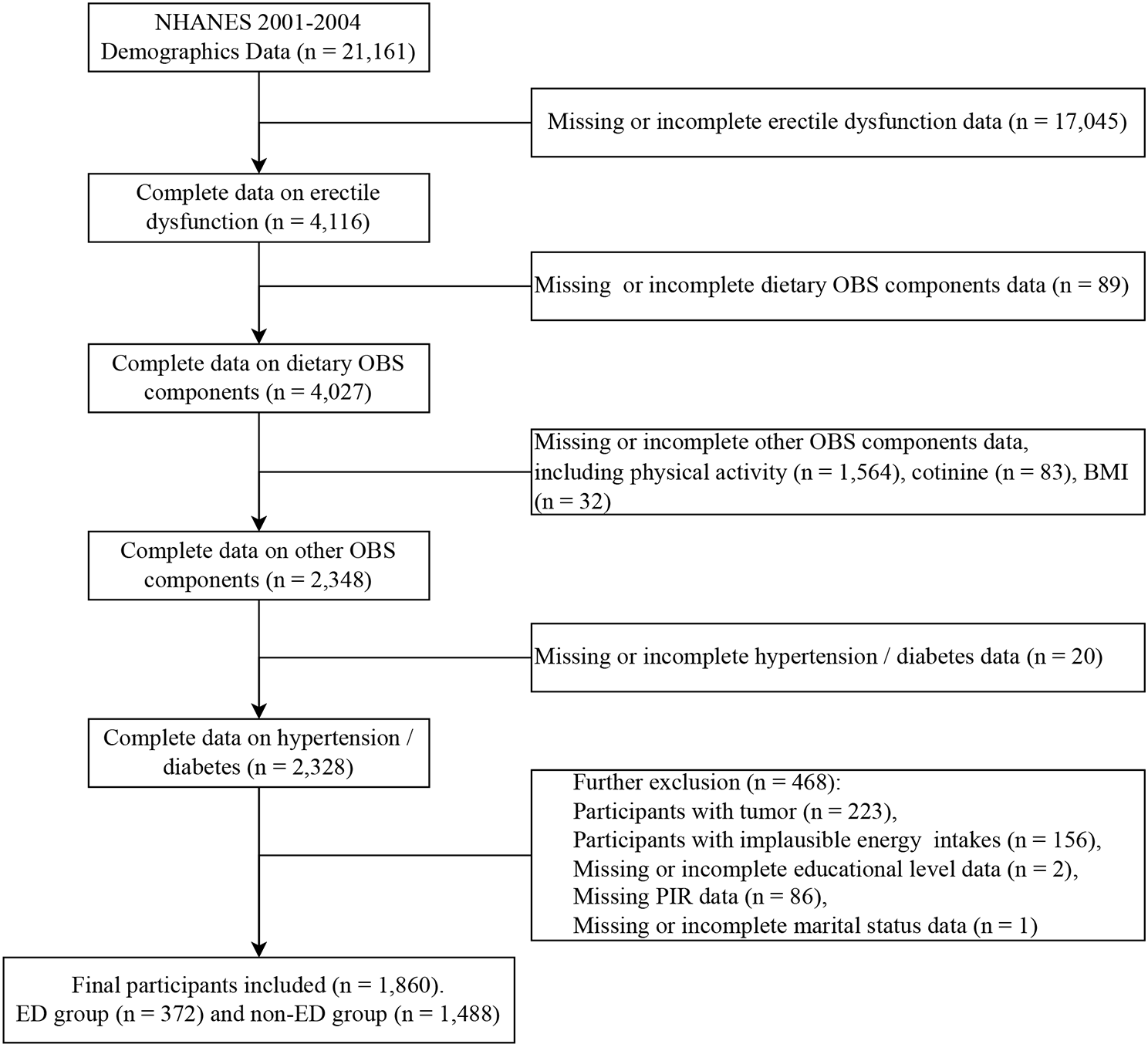
Exclusion and inclusion criteriaAdult males with dyslipidemia were selected from the NHANES database. Dyslipidemia was defined as serum triglyceride level ≥ 150 mg/dl, total cholesterol ≥ 200 mg/ dl, LDL ≥ 150 mg/dl, HDL < 40 mg/dl, or being on cholesterol medication, or being diagnosed with hypercholesterolemia by a physician (https://www.nhlbi.nih.gov/files/docs/guidelines/atglance.pdf). The total population analyzed in the study included 82,097 participants from 2001 to 2016. Participants lacking information on dietary PUFAs intakes (n = 18,138), or cardiovascular disease diagnosis (n = 28,321), or death(n = 13), or normolipidemia (n = 11,430), or female with dyslipidemia (n = 12,174), or extreme energy intake (energy intake < 800 kcal or energy intake > 8000 kcal, n = 173) were excluded and 11,848 male with dyslipidemia were recruited (Fig. 1).
Fig. 1
Flow chart of sample selection
ExposuresExposures in this study were obtained by dietary assessment using a 24-h dietary recall survey to obtain food intake discontinuously over 2 days. Dietary data were only collected on the first day during 2001–2002. Second-day dietary data were also collected after an interval of 3–10 days in subsequent survey cycles. Dietary energy and nutrient intakes were estimated using the USDA Dietary Research Food and Nutrition Database. Dietary intake components were integrated into 37 MyPyramid major groups and subgroups according to the USDA MyPyramid Equivalency Database 2.0 (MPED 2.0) User's Guide for Survey Foods. To ensure the comparability of data, two dietary survey data in the seven cycles from 2003 to 2016 were averaged. All interviewers have completed professional training to reduce bias. The exposures in this study were marine PUFAs in the diet, including eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), and docosapentaenoic acid (DPA).
OutcomesThe cardiovascular diseases in this study included five categories: congestive heart failure (n = 521), coronary heart disease (n = 860), angina (n = 465), myocardial infarction (n = 851), and stroke (n = 508). The outcome of the cross-sectional study, cardiovascular disease, was collected by questionnaire, which is a self-reported disease diagnosed by the physician. Prospective cohort study outcome, death status, as determined by the 2019 National Death Index (NDI) as of December 31. NDI is a fairly reliable and widely used resource for death recognition. ICD-10 was used to determine disease-specific death. ICD-10 codes I00-I09, I11, I13, I20-I51, or I60-I69 were assigned death due to CVD. The median follow-up time was 7.83 years. There were 2271 all-cause deaths and 749 cardiovascular deaths.
CovariatesThe covariates in our study included age (< 60 years old or ≥ 60 years old), race/ethnicity (Mexican American/ non-Hispanic white/ non-Hispanic black/ other Hispanic/ other race), education (less than high school/ high school or equivalent/ college or AA Degree/ university or above), marital status (married/ separated/ never married), ratio of family income to poverty (PIR ≤ 1.30, 1.30–1.85, > 1.85), body mass index (BMI, kg/m2), physical activity status (yes/no recreational moderate and vigorous physical activity in the past week), smoking status (yes/no smoking 100 cigarettes in a lifetime up to date), alcohol consumption status (yes/no drinking at least 12 alcoholic beverages per year), total energy intake over 24 h of dietary recall (kcal), total fat intake (g), total cholesterol intake (g), as well as hypertension, diabetes, cancer, and osteoarthritis were self-reported disease which were diagnosed by the physician.
Statistical methodsBecause the NHANES study was conducted based on complex sampling procedures, weighted analysis was used for the results of this study. The data in this study represented a national population of approximately 77 million. The logistic regression and Cox proportional hazard regression models were established for disease and death, respectively. Odds ratio (OR) and 95%CI were used for logistic multi-factor regression model results, while hazard ratio (HR) and 95%CI were used for Cox proportional hazard regression model results. Survival times in the Cox proportional risk regression model were calculated based on the time of follow-up between the date of the interview and the participant's death or the end of 2019. Dietary marine PUFAs were divided into tertiles and the lowest tertile group was used as a reference group. In the full logistic multi-factor regression model, we adjusted for age, race, education, marital status, family poverty, BMI, physical activity, smoking status, alcohol consumption, hypertension, diabetes, total energy intake, total fat intake, and total cholesterol intake. In the final Cox proportional hazard regression model, we adjusted for age, race, education, marital status, family poverty, BMI, physical activity, smoking, alcohol consumption, hypertension, diabetes, cancer, osteoarthritis, total energy intake, total fat intake, and total cholesterol intake. All continuous variables were measured by Wilcox test and expressed as median and interquartile range (Median ± IQR), while categorical variables were measured by Wald test and expressed as percentages. All statistical analyses were performed using R 4.2.2 software, and bilateral p < 0.05 was considered statistically significant.
Sensitivity analysisIn addition, six sensitivity analyses were conducted in this study. In the first group, we analyzed the association of marine PUFAs intake with cardiovascular disease, all-cause mortality, and cardiovascular mortality in obese or overweight populations (BMI > 27). Participants who had no extreme dietary fat intake and were followed for more than 2 years were in the second and third groups. In the fourth group, we analyzed the association of marine PUFAs intake with cardiovascular disease, all-cause mortality, and cardiovascular mortality in elderly men with dyslipidemia who were over 60 years old. In the last two sets of sensitivity analyses, we selected women with dyslipidemia and all male participants who met the criteria, respectively.
Comments (0)