This study demonstrates an association between an increase in antithrombin activity of less than 1%/IU/kg with worse patient outcomes. Our findings demonstrate that higher SOFA scores and higher FDP levels are associated with a smaller increase in antithrombin activity.
As previously performed in trauma-associated DIC [7, 8], antithrombin activity increased by approximately 1%/IU/kg in our study. Approximately 38.2% of patients with a baseline SOFA score > 13 and 39.7% with an FDP score > 25 μg/mL showed a 1%/IU/kg or more increase in activity. Patients with greater organ dysfunction and stronger coagulation/fibrinolysis activation exhibited a smaller increase in antithrombin activity, possibly due to increased consumption, suppressed hepatic production, and vascular leakage [19]. These findings underscore the importance of considering these factors when determining the optimal dosing and timing for administering antithrombin concentrate.
The observed association between increased antithrombin activity and improved survival may partly reflect baseline severity bias, as patients with greater responses might have had more favorable clinical conditions at the outset. To address this concern, we conducted a multivariate Cox proportional hazards analysis adjusted for baseline SOFA and JAAM DIC scores. The association between increased antithrombin activity and improved survival remained statistically significant after adjustment, supporting the robustness of the observed relationship.
To improve prognosis, the cutoff of post-treatment antithrombin activity was reported to be approximately 80% [6]. Given that the baseline antithrombin activity in our cohort was approximately 49% and the average body weight was 54 kg, patients who received a standard dose of 1,500 IU/day likely reached this cutoff. This suggests that an increase of 1%/IU/kg antithrombin activity may differentiate favorable therapeutic outcomes. However, this response was not consistent across all patients—those with higher baseline SOFA scores or elevated FDP levels appeared to require larger doses of antithrombin to achieve comparable increases. Notably, the 80% target level has been suggested in retrospective studies but has not been validated in prospective trials. Therefore, further prospective investigation is warranted to determine the optimal target antithrombin activity level.
Previous reports, such as the KyberSept trial, have suggested that high-dose antithrombin administration may increase bleeding risk [11]. On the contrary, our study did not find a direct association between antithrombin activity and bleeding risk. Concomitant use of anticoagulants, including heparin, protease inhibitors, and thrombomodulin, was also not associated with increased bleeding. A sensitivity analysis limited to major bleeding events yielded similar results (Suppl. Table 3). In the KyberSept trial, approximately 70% of patients received heparin during the first 4 days of treatment, while in our cohort only 14.1% did. Moreover, the total antithrombin dose in KyberSept was 30,000 IU over 4 days, markedly higher than the standard Japanese regimen of 1,500 IU/day, typically administered for 3 days. These differences in both concomitant heparin use and total antithrombin dose may partly explain the lower bleeding incidence observed in our cohort. In our cohort, the overall incidence of bleeding was 5.5%, consistent with previous reports such as Umemura et al. [20]. Similarly, J-SSCG 2024 notes that bleeding complications may increase by 8 per 1,000 patients (95% CI: − 24 to + 89) with antithrombin administration, based on randomized controlled trial data [5]. These findings suggest that although anticoagulant therapy using antithrombin may carry a risk of bleeding, the risk appears to be lower in patients with sepsis-associated DIC.
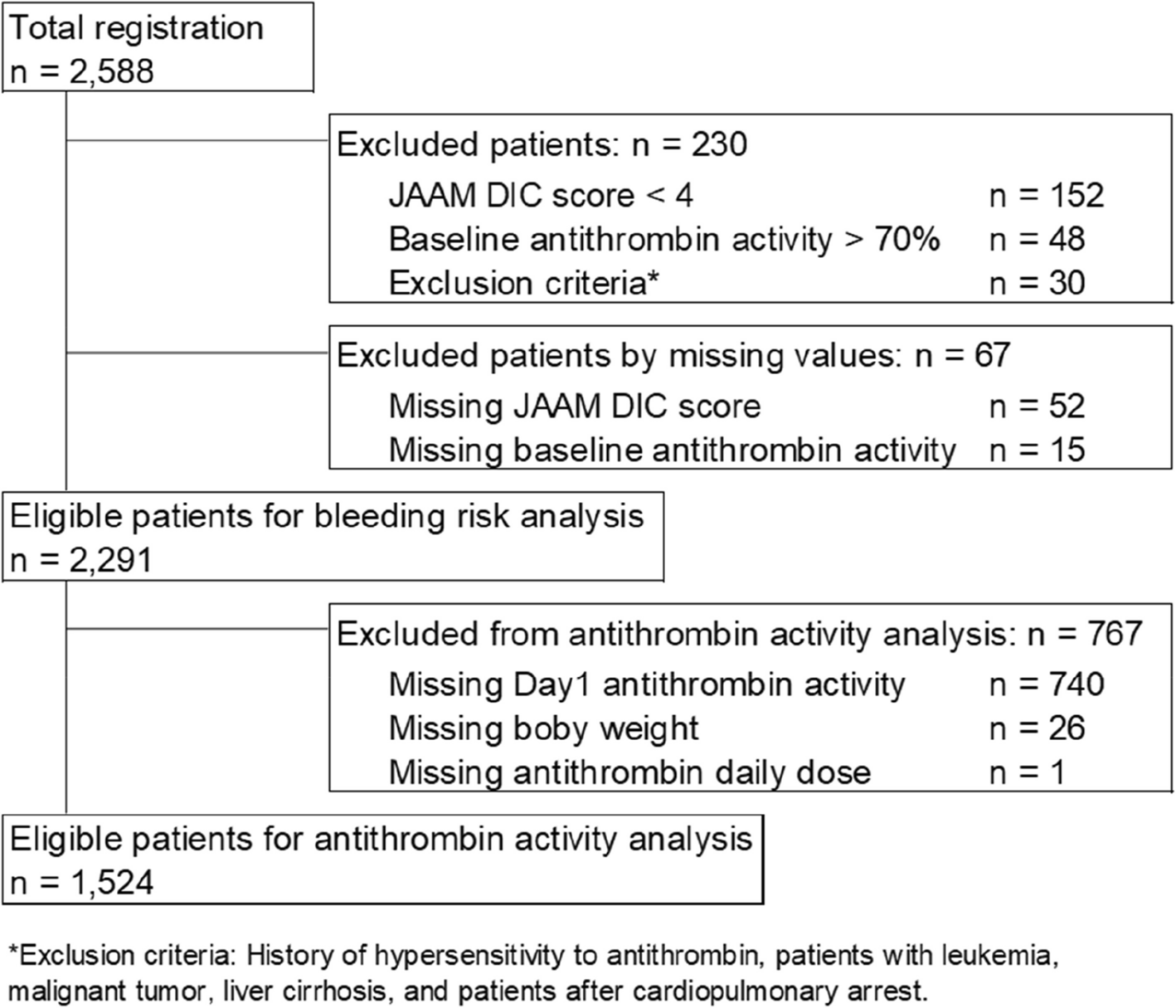
This study had several limitations. First, because of the retrospective nature, missing data were relatively common. In particular, antithrombin activity on Day 1 was frequently missing. Second, the antithrombin dosage was not standardized and was administered at the discretion of the attending physician, potentially introducing variability in dosing and treatment decisions. Although post-administration activity levels were available, treatment adjustments based on these values were not protocolized, raising the possibility of clinician-driven bias and residual confounding. Third, although we utilized only baseline and Day 1 data, 58.5% of cases received treatment over three days, which might affect patient outcomes. Finally, because our analysis only included patients who received antithrombin, we were unable to compare the incidence of bleeding with that in patients without treatment.




Comments (0)