
Remember me
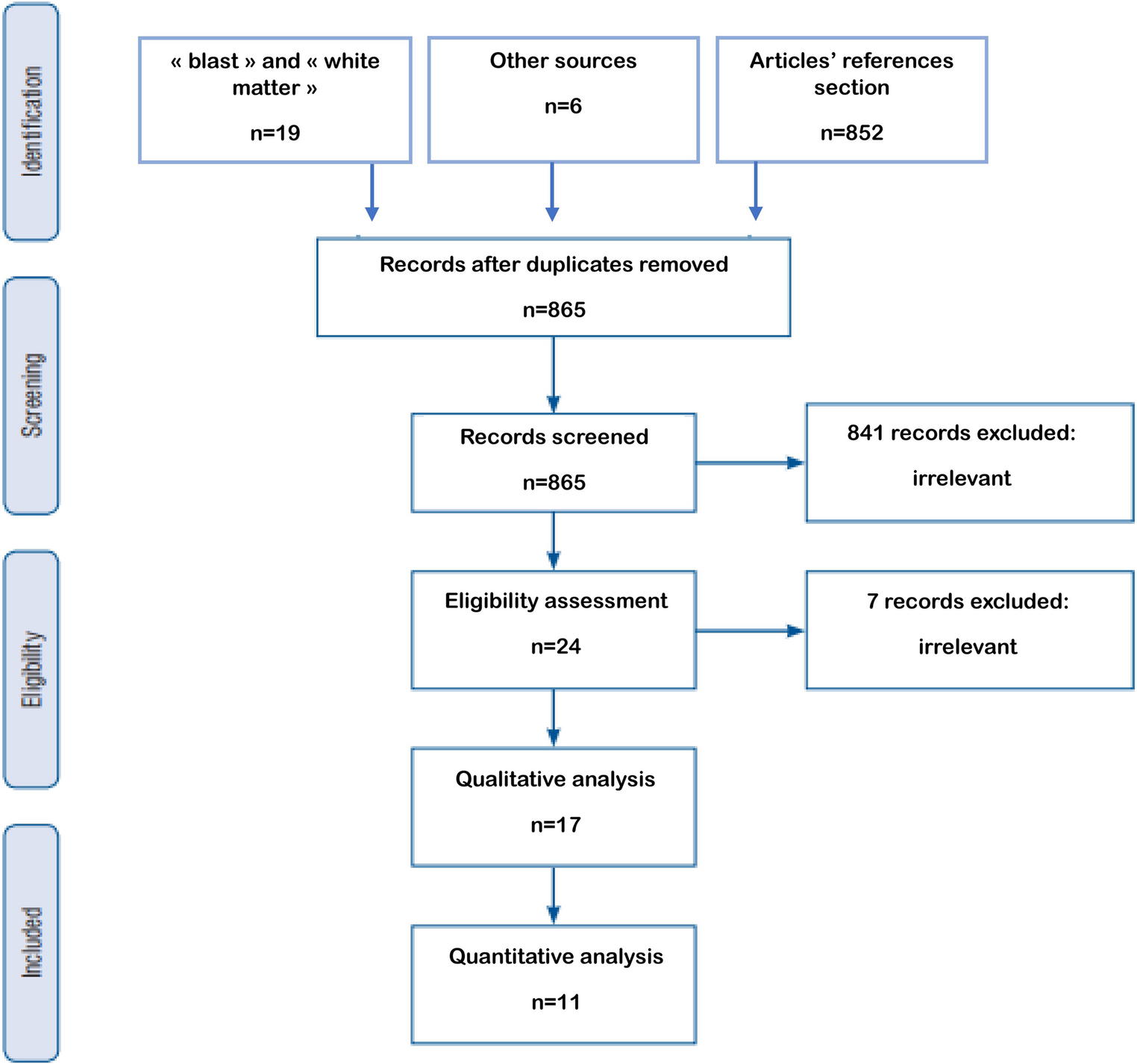
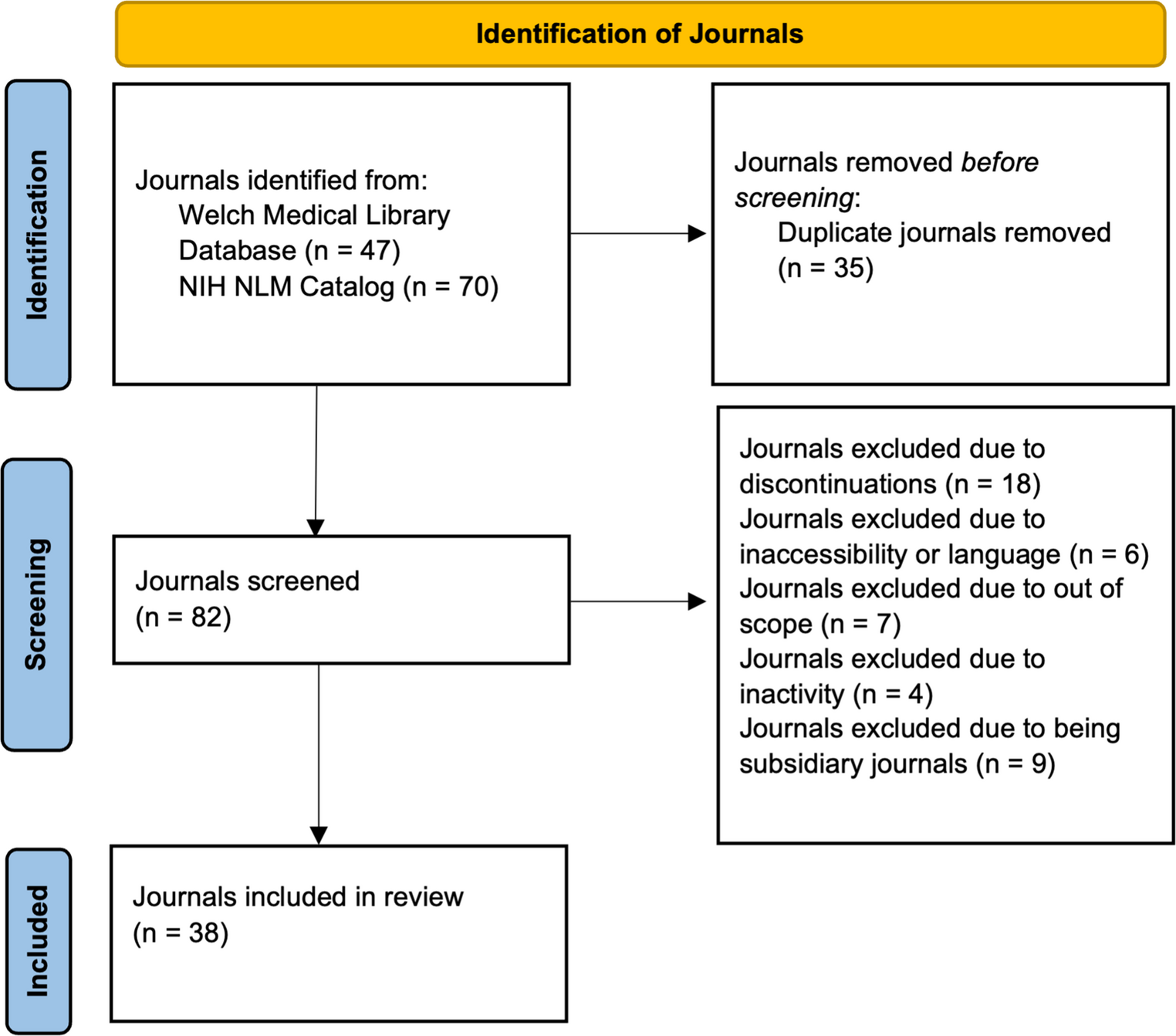
After a full-text review, 14 papers met the inclusion criteria and were included in the final analysis; Fig. 1. Of the included studies, three were based on CDC surveillance data [28,29,30], and eleven were retrospective cross-sectional studies [8,9,10, 12,13,14, 31,32,33,34,35]. Five studies were conducted at the state level [8, 14, 30, 33, 34], while nine were nationwide in scope [9, 10, 12, 13, 28, 29, 31, 32, 35]. Four studies explicitly reported the severity of TBI [12, 30, 31, 33]; Tables 1 and 2.
Fig. 1
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analysis) Flow Diagram
Table 1 Study characteristicsTable 2 Study key findingsQuality assessmentEleven studies were assessed using the NIH Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. Six studies were rated as good quality, having met most of the NIH criteria for methodological rigor [8, 10, 13, 31, 33, 35]. These studies utilized nationally representative datasets, and they featured clearly defined populations, outcomes, and robust statistical methods. Five studies were rated as fair quality [9, 12, 14, 32, 34]. While these studies contributed valuable insights, they exhibited moderate limitations, including partial data coverage (e.g., data limited to Indian Health Service facilities), potential racial misclassification, or incomplete adjustment for key confounding variables. Of the fourteen studies included in the analysis, three were CDC surveillance reports that are not eligible for this assessment [28,29,30]; Table 3.
Table 3 NIH quality assessment tool for observational cohort and Cross-Sectional studiesEmergency department visit ratesFrom a pooled three-year sample (1998–2000) of 70,900 emergency department (ED) visits in the National Hospital Ambulatory Medical Care Survey (NHAMCS). The average annual incidence rate for mild TBI was 503.1 per 100,000 [12]. The highest rates were observed among AI/ANs (1,026 per 100,000), followed by African Americans (624.6), and Whites (491) [12]. Between 2005 and 2014, a total of 44,918 TBI–related ED visits were recorded across Indian Health Service (IHS) hospitals [35]. The overall age-adjusted rate of TBI-related ED visits among AI/ANs was 333.4 per 100,000, with a statistically significant increase in rates observed from 2008 to 2014 and an average annual percent change (APC) of 4.37 [35].
Hospitalization ratesBetween 1992 and 2021, five studies reported TBI-related hospitalization rates among AI/ANs ranging from 71.5 to 81.7 per 100,000 [9, 14, 30, 32]. The highest rate was observed in Alaska, reaching 186.7 per 100,000 [8].
Mortality ratesThis review spans more than three decades (1989–2021). Seven studies reported TBI-related mortality rates among AI/ANs in the United States, with rates ranging from 27.2 per 100,000 in 1998 to 29 per 100,000 in 2020, representing the highest rates among all racial and ethnic groups at all times [9, 10, 13, 28, 29, 32]. Notably, in Alaska, the TBI-related mortality rate was markedly higher, at 65 per 100,000 [8].
Mechanism of injuryAdekoya et al. reported that MVAs, falls, and violence are the leading causes of TBI among AI/ANs [32]. In 2020, Sarmiento et al. reported that falls were the leading cause of TBI-related ED visits among AI/ANs, with violence being in second place [35]. However, falls accounted for a smaller percentage of total injuries among AI/AN individuals compared to White Patients (27.7% vs. 45.4%) [33]. On the contrary, Assault-related TBIs were twice as prevalent among AI/AN compared to other racial groups (21% vs. 10%) [14]. In comparison to White patients, AI/ANs sustained more injuries to the head and neck (42.1% vs. 37%) and intentional injuries—including those due to assault and self-harm— (20.1% vs. 6.7%) [33]. Compared to White patients, AI/AN trauma patients exhibited a significantly greater proportion of penetrating injuries (13.5% vs. 6.4%) [33].
Regarding hospitalization, in 2005, Rutland-Brown et al. found that MVAs are the leading cause of TBI-related hospitalization among AI/ANs, with a rate of 27 per 100,000, accounting for over 40% of all TBI-related hospitalizations and occurring at twice the rate of violence (13.8 per 100,000) [14]. However, in 2019, a nationwide study reported that the leading causes of TBI-related hospitalizations are falls (34.8 per 100,000 population), MVAs (20.8), and violence (14.4) [9].
The CDC reported that MVA-related TBI mortality rates were highest among AI/ANs at 11.5–12.5 per 100,000, followed by Whites (6.1–7.2), African Americans (5.4–6.3), and Hispanics (5) [28, 29]. Similarly, AI/ANs experienced the highest rate of fall-related TBI deaths (3.6 per 100,000), followed by Whites (3.2), Hispanics (2.7), and African Americans (2) [29]. Firearm-related injuries represented the second leading cause of TBI-related mortalities, with suicides accounting for 63% among AI/ANs [28]. Most recently, several studies reported that suicide and self-harm are emerging as the leading causes of TBI-related mortality among AI/ANs [8, 10, 13].
Gender disparitiesMales consistently exhibited higher age-adjusted TBI-related ED visit rates compared to females [12, 35]. Additionally, the overall age-adjusted rate of TBI-related hospitalizations in males was almost twice as high as in females [30]. This sex disparity was even more pronounced among African Americans (2.8:1) and AI/ANs (2.5:1) [10, 13, 30, 32]. In 2025, Newell et al. reported that in the state of Alaska, males accounted for 64.8% of TBI-related hospitalizations [8].
Age as a confounding factorAI/ANs experience notable health disparities, including a life expectancy approximately five years shorter than that of the overall U.S. population (73 years vs. 78.5 years, respectively) [35]. The CDC reported that males aged 20–24 years had the highest rates of MVA-related TBI mortalities: 35 per 100,000 among AI/ANs, 23.4 per 100,000 among Whites, and 17.1 per 100,000 among African Americans [28]. In another report across 14 states, the CDC reported that among individuals aged 20 to 45 years, AI/ANs exhibited the highest TBI-related hospitalization rates, ranging from 92 to 105.2 per 100,000. These rates exceeded those of African Americans (65.3–85.2 per 100,000), Asians (30.1–41.2 per 100,000), and Whites (44.8–81.5 per 100,000) [30]. Assault-related TBIs were most prevalent among African American and AI/AN males, with rates of 31.3 and 29.5 per 100,000, respectively—approximately four times higher than the rate observed in White males [30]. Interestingly, in the 25–34 and 35–44-year age groups, assaults were the most common cause, with hospitalization rates of 28.2 and 23.6 per 100,000, respectively [32]. For patients younger than 15 years and those older than 45 years, falls were the leading cause of injury, with rates of 17.7 and 19.4 per 100,000, respectively [32].
Prevention initiativesMost TBIs are preventable. Implementing effective prevention measures not only saves lives but also reduces long-term disability and generates significant cost savings within the healthcare system and across society at large. Implementing programs to prevent TBI, especially in high-risk activities like outdoor pursuits and sports, can reduce the incidence of head injuries. To improve healthcare services for AI/ANs, the IHS provides financial support for medical services to approximately 2.3 million AI/ANs [35]. Law enforcement strategies for the proper use of seatbelts, BAC levels less than 0.08 g/dL for drivers older than 21 years old, sobriety checkpoint programs, and awareness campaigns are effective in reducing the rates of MVAs among American Indians and Alaska Natives [35]. In 2012, the CDC launched the Stopping Elderly Accidents, Deaths, and Injuries (STEADI) initiative to provide healthcare providers with the necessary tools to identify patients at risk of falls, understand risk factors, implement effective strategies, and subsequently reduce the risk of falls among the older adult population [36].
Within the State of Alaska, TBI prevention initiatives are multifaceted, targeting a broad spectrum of safety and public health concerns. Public awareness campaigns and educational programs emphasize motor vehicle safety and the distribution of protective equipment [37,38,39]. Targeted interventions include fall prevention programs for older adults, such as the free provision of ice cleats and participation in balance training initiatives [40,41,42]. Suicide prevention strategies are similarly diverse, encompassing tribal-specific interventions, community-led initiatives, and expanded access to mental health services [43,44,45]. The Alaska Statewide Suicide Prevention Council partners with multiple stakeholders to address suicide rates,40 while the Alaska Native Tribal Health Consortium offers education, training, and telehealth-based support [46,47,48]. Injury prevention efforts also address head trauma resulting from motor vehicle collisions. The Center for Safe Alaskans (https://safealaskans.org) advances safe transportation practices through child passenger safety education, complimentary car seat inspections, and resources for novice drivers.
Comments (0)