
Remember me



The study protocol, with well-defined methodology and inclusion criteria, was registered on PROSPERO with reference number CRD42025645366.
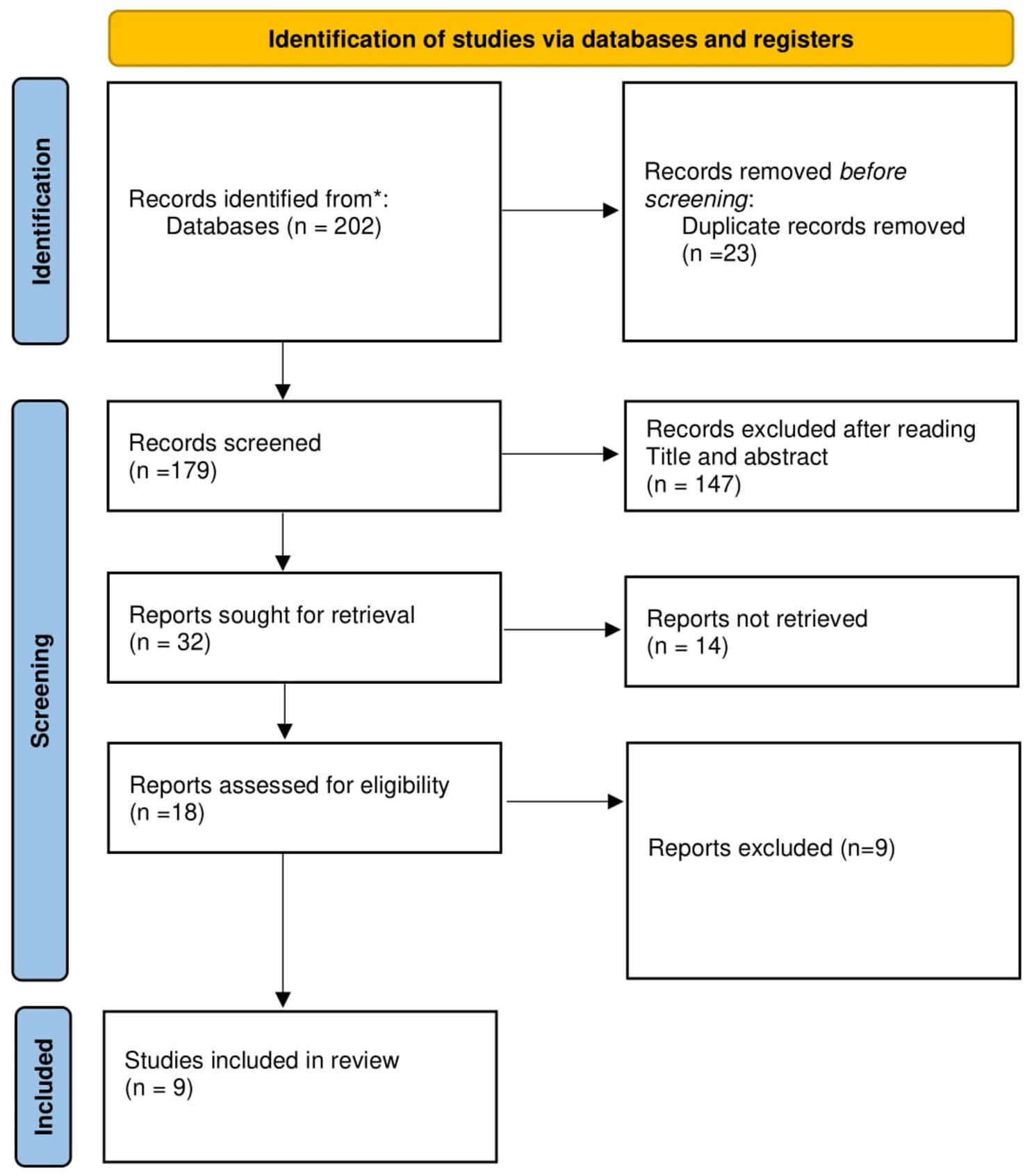
Search StrategyThis systematic review and meta-analysis followed the principles of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses. The PRISMA diagram detailing the selection process is shown in Fig. 1. The PubMed, Embase and Google Scholar databases were searched from 1990 to 9 March 2025. Studies were also obtained from supplementary sources, manual searches and other repositories. Cross-references from the published articles were manually searched to retrieve additional literature.
Fig. 1
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram detailing the study identification and selection process
To create an extensive search strategy that encompassed all fields in the records as well as Medical Subject Headings (MeSH words) for broadening the search in an advanced PubMed search, the predefined phrases were identified. For the PubMed database, medical subject headings (MeSH terms) and relevant keywords were systematically combined via Boolean operators (AND, OR) to identify records. Similarly, for Embase, Emtree terms and keywords were combined with Boolean operators to ensure the comprehensive retrieval of relevant studies. A similar approach was applied in Google Scholar to capture additional literature via targeted search terms. Details of the preliminary search strategy are provided in the S1 Appendix.
Eligibility CriteriaStudies were considered eligible if they met the following criteria: (i) evaluated the diagnostic potential of microRNAs as biomarkers for myasthenia gravis (MG); (ii) included MG patients diagnosed via established clinical and laboratory criteria, such as serological tests, electrophysiological studies, or histopathological examinations; and (iii) reported sufficient data to construct a 2 × 2 contingency table, including true positives (TPs), false positives (FPs), true negatives (TNs), and false negatives (FNs), or provided sensitivity and specificity values. Articles were excluded on the basis of the following criteria: (i) not published in English; (ii) not conducted on human subjects; (iii) reviews, meta-analyses, letters, editorials, or conference abstracts; (iv) studies that did not assess the relationship between MG and miRNAs; (v) focused solely on gene polymorphisms rather than miRNA expression; (vi) datasets derived exclusively from bioinformatics databases without experimental validation; and (vii) studies with incomplete or insufficient data for statistical analysis. Eligible studies were grouped on the basis of study design, miRNA profiling methods, and diagnostic outcomes to ensure a systematic and quantitative synthesis of the findings.
Exclusion CriteriaArticles were excluded on the basis of the following criteria:
(i)not published in English;
(ii)not conducted on human subjects;
(iii)reviews, meta-analyses, letters, editorials, or conference abstracts;
(iv)studies that did not assess the relationship between MG and miRNAs;
(v)focused solely on gene polymorphisms rather than miRNA expression;
(vi)datasets derived exclusively from bioinformatics databases without experimental validation;
(vii)studies with incomplete or insufficient data for statistical analysis;
(viii)studies focusing on congenital myasthenic syndromes or other autoimmune neuromuscular junction disorders, such as Lambert-Eaton myasthenic syndrome (LEMS).
(ix)studies that investigated only ocular myasthenia gravis (OMG) without inclusion or comparison to generalized MG (GMG).
Selection of StudiesThe literature search was performed by PP1. The included studies were exported to Google Sheets in compatible format. Duplicate articles were screened manually. Duplicates were then recorded and removed. After removing duplicates, two independent authors, PP1 and AS, screened the title and abstract of every article that remained. Full-text articles were obtained for the relevant studies satisfying the inclusion criteria. The data were extracted by the two authors, PP1 and AS, independently. Any disagreements were resolved through discussion with third author (PP2).
Data ExtractionThe following search strategies were employed to identify relevant studies: for PubMed, we used a combination of MeSH terms and keywords, including"micrornas,""mirna*,""micro RNA,""miRNAs,"and their variations, combined with terms related to biomarkers ("biomarker*,""biological marker*") and diagnostic performance ("diagnosis*,""diagnostic*,""ROC") in relation to myasthenia gravis. For Embase, a similar approach was applied via the respective indexing system, ensuring the comprehensive retrieval of studies on microRNAs as diagnostic biomarkers for myasthenia gravis. Additionally, Google Scholar was searched via a broad keyword-based strategy to capture relevant articles that may not be indexed in traditional databases. A comprehensive search strategy is provided in S1_Appendix.
Quality Assessment of the StudiesWe assessed the quality of diagnostic studies on the basis of the Quality Assessment of Diagnostic Accuracy Studies‐2 (QUADAS‐2) criteria. It consists of 4 key domains: patient selection, index test, reference standard, flow and timing, and judgement of bias and applicability. Each domain was assessed in terms of risk of bias, and the first 3 domains were assessed with respect to applicability. Each item is answered with “yes,” “no,” or “unclear.” An answer of “yes” means a low risk of bias, whereas “no” or “unclear” means the opposite.
Statistical AnalysisWe extracted the number of true positives (TPs), false positives (FPs), false negatives (FNs), and true negatives (TNs) from each study to calculate the pooled sensitivity, specificity, Positive Likelihood Ratio (PLR), Negative Likelihood Ratio (NLR), Diagnostic Odds Ratio (DOR), and their corresponding 95% confidence intervals (CIs). The pooled diagnostic value of miRNAs was evaluated using the summary receiver operating characteristic (SROC) curve and the area under the curve (AUC). Deeks’ funnel plot was constructed to assess publication bias. Heterogeneity among studies was assessed using the chi-square test and Higgins’ I2 statistic, with I2 values of 25%, 50%, and 75% interpreted as low, moderate, and high heterogeneity, respectively. Heterogeneity was considered significant if P < 0.1 or I2 > 50%. Between-study variance (τ2) was also estimated, and standard deviations from the bivariate random-effects model were used to quantify variability in sensitivity and specificity. To assess potential threshold effects, we used Spearman’s rank correlation between logit-transformed sensitivity and specificity, with a p-value < 0.05 indicating a significant threshold effect. Meta-regression, subgroup, and sensitivity analyses were conducted to explore sources of heterogeneity. All statistical analyses were performed using R and Stata (version 12.0), and results were considered statistically significant at P < 0.05.
Subgroup and meta-regression analyses were conducted to investigate sources of heterogeneity, focusing on geographic region (Asia vs. Europe), clinical subtype (ocular vs. generalized MG), and serostatus (e.g., AChR-positive). As all included studies employed RT-qPCR for miRNA quantification, platform-related variability could not be assessed. Demographic variables such as age and ethnicity were inconsistently reported and therefore excluded from analysis.
Comments (0)