
Remember me
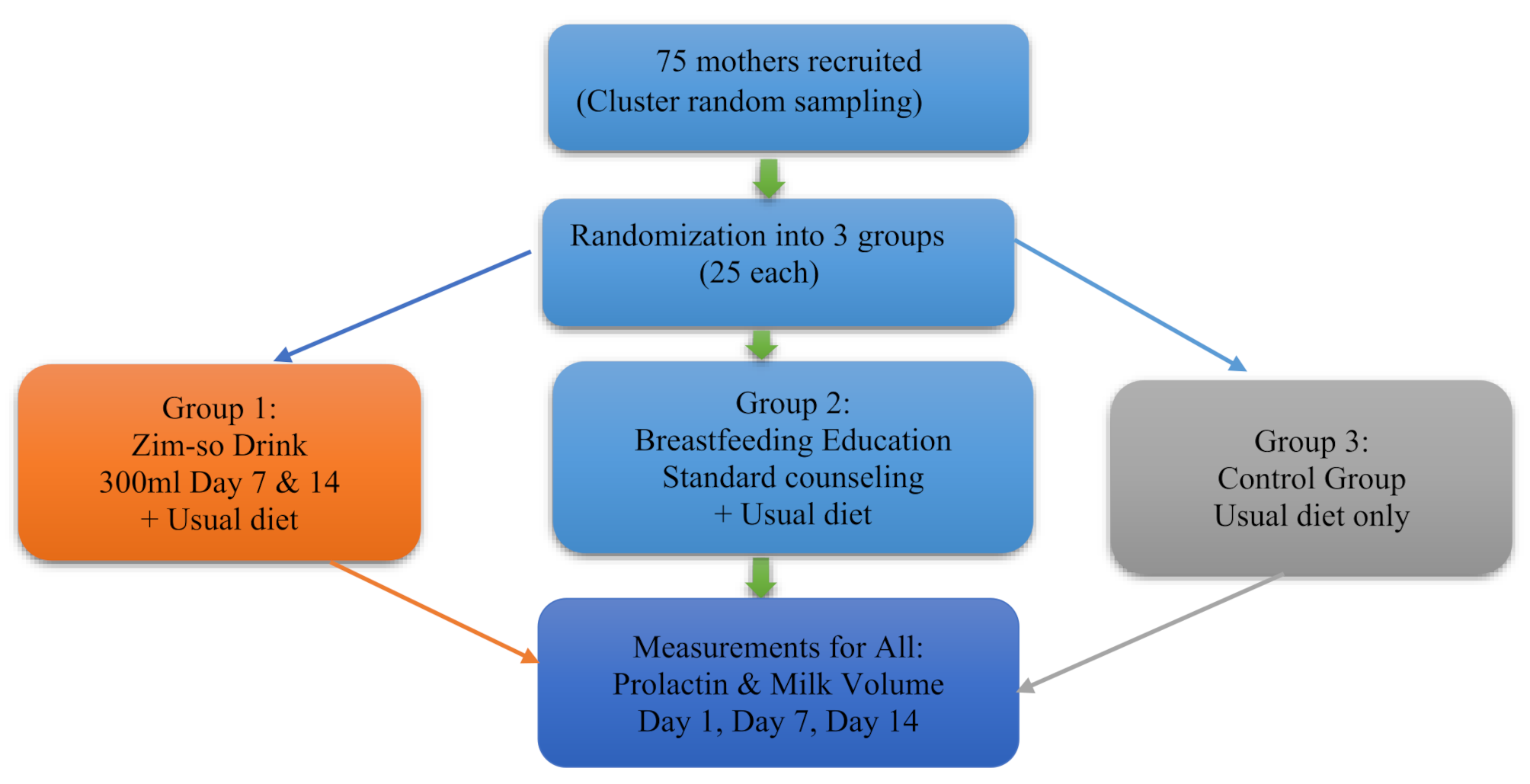


A randomized controlled trial (RCT) was conducted over 14 days. Cluster random sampling was used to recruit 75 postpartum mothers from five maternal and child health (MCH) clinics within the Tamale Metropolis. Each health facility served as a cluster, selected based on high postpartum attendance, geographic spread, and willingness to participate. Within each cluster, eligible mothers were listed and randomly selected using proportional allocation based on clinic size. This aimed to compare the effect of the Zim-so drink, a formulation made up of 74% millet, 25% soya, 1% ginger, and standard postpartum breastfeeding education based on the UNICEF counseling standard on maternal nutrition [13] on breastmilk outcomes. The Zim-so drink has a proximate composition per 100 ml of: 88.40 g Moisture Content, 0.56 g Ash Content, Potassium 0.18 g, 0.13 g Calcium, 0.04 g Magnesium, 0.03 g Sodium, 0.06 g Vitamin C, 0.25 g Crude Fat g, 0.80 g Crude Protein, 9.72 g Carbohydrate, Caloric Value of 46.38 kcal with crude fiber absent. The drink was formulated by the team and so has no standard manufacturer or branded commercial version.
Lactating women were randomly assigned to three groups: The first group, the Zim-so drink group, enrolled mothers in consuming 300 ml at two time points: the first feed on the 7th day and the second feed on the 14th day, in addition to their usual diet. The second group, breastfeeding education, had mothers receiving the standard postpartum breastfeeding counseling and continuing their usual diet. The breastfeeding education sessions were delivered on Day 1 (immediately after baseline data collection), Day 7, and Day 14, approximately two hours before each respective data collection point. The control group received nothing and continued their usual diet. Blinding of participants and study personnel was not feasible due to the distinct nature of the interventions (consumption of the Zim-So drink and breastfeeding education sessions). However, standardized data collection procedures were employed across all groups to minimize observer bias. Figure 1 shows the flow chart of the RCT.
Fig. 1
This study was registered with Pan African Clinical Trials Registry on 16 January 2025 (registration number: PACTR202501557719558 and ethics granted by the Committee on Human Research, Publication and Ethics with the identification number: CHRPE/AP/102/2.
Study participantsParticipants included were lactating women aged 18 to 38 years with hypogalactia, identified by maternal self-report of low milk supply, ineffective breastfeeding behaviors, and frequent feeding patterns indicating inadequate milk transfer. Additional inclusion criteria were: intention to exclusively breastfeed for at least one month, no medical conditions likely to cause mother-infant separation or reduced breastfeeding frequency (e.g., NICU admission, postpartum hemorrhage or sepsis), no allergies to millet, soybean, or ginger, no history of diagnosed psychological disorders, non-smokers, normal singleton term delivery, and a BMI between 19.8 and 26 kg/m² to minimize the influence of body weight extremes on prolactin levels and breastfeeding outcomes. They had no breast problems such as abscesses or flat nipples, not on any milk-interfering medications, any synthetic galactagogues, or antibiotics. Infants were mature at birth and weighed between 2.5 kg and 4 kg and did not have any abnormalities or birth defects, diseases, or nutritional problems, and were willing to participate in this study. Participants who had occurrence of any mental or physical illness during the study that interferes with breastfeeding such as hepatitis, cancer, HIV, and breast problems; use of other herbal and chemical drugs that increase milk during the intervention, use of dopamine antagonists (domperidone, metoclopramide, risperidone, and phenothiazine), cessation of breastfeeding for any reason, and unwillingness to continue the intervention were excluded. Infants with congenital abnormalities affecting growth or nutrition were also excluded. Both the inclusion and exclusion criteria were assessed with the help of midwives in these facilities.
Sample sizeThe sample size for this study was determined using G-Power software [14], applying a fixed-effect, one-way ANOVA (F-test) with a desired statistical power of 80% (0.8), a significance level (α) of 0.05, and a target effect size of 0.8. This effect size was chosen based on Cohen’s criteria, where 0.8 indicates a large and clinically meaningful difference. The selection was also informed by findings from similar intervention studies [15, 16] that examined the impact of dietary and educational interventions on lactation outcomes, which reported large effect sizes in changes to prolactin levels and breastmilk volume following galactagogue use. These studies indicated effect sizes ranging from 0.7 to 0.9, thus supporting the appropriateness of using 0.8 in this context. By adopting this estimate, the study aimed to detect significant group differences while ensuring sufficient statistical power with a feasible sample size. The total calculated sample size of 75 participants (25 per group) was thus deemed adequate to detect meaningful effects between intervention arms and the control group.
Study proceduresBaseline data collection included comprehensive demographic, maternal, and infant health characteristics. Socio-demographic data (age, education, occupation, religion, marital status, and household wealth) were collected through structured interviewer-administered questionnaires. Maternal health characteristics (including pregnancy complications, postpartum conditions, emotional concerns, and coping abilities) were also assessed using standardized checklists adapted from validated maternal health screening tools [17]. Infant health characteristics such as birth weight, latching quality, suckling strength, breastfeeding frequency, and session duration were assessed by trained midwives using observational scoring forms based on WHO breastfeeding assessment guidelines [18]. Where subjective reporting was involved (emotional concerns, motherhood coping ability, and family support), the Likert-scale responses [19] were used and then categorized for analysis. The International Physical Activity Questionnaire (IPAQ) [20] was used to assess the level of physical activity.
Dietary intake was also assessed using the 24-hour dietary recall method, conducted on Day 1, Day 7, and Day 14 of the study. These records were evaluated using the Minimum Dietary Diversity for Women (MDD-W) tool [21], which was developed by the Food and Agriculture Organization (FAO) to measure dietary diversity based on the consumption of at least 5 out of 10 specific food groups in the previous 24 h. Achieving this minimum is associated with a higher likelihood of meeting essential micronutrient needs and is used as a proxy indicator for diet quality. To accurately measure breastmilk volume, mothers received training from a midwife on the proper use of a manual breast pump (Lansinoh brand, Thailand) expressed into graduated feeding bottles. There were three evaluation time points for breast milk volume in the period of 2 weeks (14 days); day 1, day 7 and day 14. Mothers were provided with a logbook to record the time and volume of pumped milk. However, the volume of milk expressed per a single feeding session was recorded.
Prolactin Levels were assessed from venous blood samples (5 mL) obtained from all the mothers on day 1, day 7, and day 14 of the intervention and processed on the same day of sample collection. Serum prolactin concentrations were measured using a standardized Enzyme-Linked Immunosorbent Assay (ELISA) protocol [22]. Considering the biological half-life of prolactin (approximately 15–20 min), levels in the Zim-so drink group were measured 20 min post-consumption to capture peak hormonal response.
To minimize observer bias, all data collectors (including midwives and research assistants) received standardized training on study protocols, interview techniques, and use of the ELISA kit and breast milk expression tools, with mock sessions conducted prior to data collection. To ensure consistency and minimize diurnal variation, all measurements were conducted between 9:00 a.m. and 10:00 a.m. across all study groups. These standardization procedures, combined with training and structured tools, ensured high data quality and consistency throughout the study.
Data analysisDescriptive statistics (mean, standard deviation) for demographic characteristics. Dietary intake was assessed using 24-hour dietary recalls conducted by trained interviewers. Participants were asked to recall all foods and beverages consumed during the previous 24 h. Standardised multiple-pass methods were employed to enhance recall accuracy, including probing for forgotten foods and portion sizes. An Independent samples t-test was used to compare mean breast milk volumes between the intervention and control groups. ANCOVA was performed to adjust for potential confounders, including infant birth weight, maternal age, parity, and daily fluid intake, as these factors are known to influence lactation outcomes [23]. Repeated measures ANOVA was done for longitudinal data analysis of breast milk volumes. An independent samples t-test was used to compare the geometric means (SD) between the intervention and control groups, with a p-value of less than 0.05 considered statistically significant at a 95% confidence level. The analyses were done using IBM SPSS Statistics for Windows Version 23.0 [24].
Comments (0)