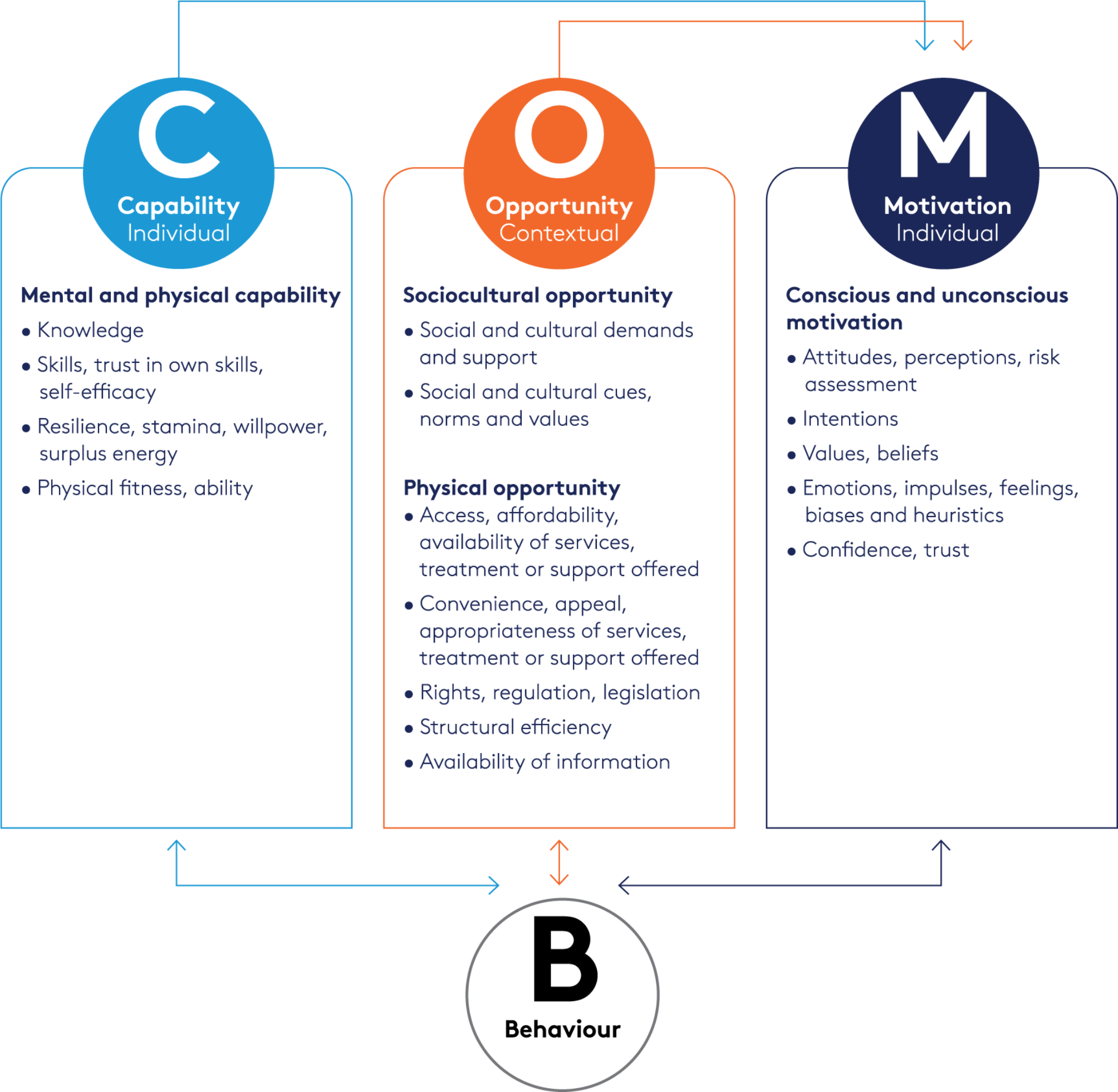
Mothers’ and health workers’ perceived barriers and drivers to exclusive breastfeeding and supporting exclusive breastfeeding in the first 6 months respectively, are presented below. Findings are organised by COM factors [20], with participants’ behaviours (of exclusive/ supporting exclusive breastfeeding) presented prior to individual level factors (motivation and capability) then contextual factors (physical and sociocultural opportunity). Where there were differences in barriers or drivers by study site, or professional role for health workers, or by infant feeding practice for mothers, these are indicated. Otherwise, there were no differences. Illustrative quotes are presented in Tables 3, 4 and 5.
Table 3 Illustrative quotes for BehaviourTable 4 Illustrative quotes for individual factors: capability and motivationTable 5 Illustrative quotes for contextual factors: sociocultural and physical opportunityBehaviour
All the mothers said that during their pregnancy they had planned to exclusively breastfeed. Most commenced breastfeeding immediately after delivery (Quote B1, Table 3). Those who didn’t typically offered medical explanations (that were not always correct), namely mother and baby were in the intensive care unit (ICU), the baby was delivered by caesarean-section, had a low birth weight, or needed medical attention (Quote B2, Table 3). While all stated they were breastfeeding when they left the maternity hospital, this was not always exclusively.
Mothers described a variety of infant feeding practices in the first 6 months of their child’s life. Some had given the baby additional fluids (e.g., boiled water, dill water or tea) soon after birth or after one week. Some gave additional solids (e.g., porridge, bananas, apples, cookies softened in water) from the age of 3–4 months. The mothers supplementing with formula either started this in hospital or typically began around 2–3 months later. This was the same time that one mother switched fully from breastfeeding to formula. Multiple reasons for these practices are described below in Capability and Motivation. Notably most had adopted the same feeding practices for this child that they had used with their older children. Some, however, used different feeding practices with this baby; for example, amongst those now supplementing with formula had exclusively breastfed their older children (Quote B3, Table 3).
The perception amongst doctors was that most mothers exclusively breastfeed for 6 months (Quote B4, Table 3). Some mentioned a small minority (mostly from rural areas) who give additional fluids/solids to their baby before 6 months (Quote B5, Table 3). Similarly, some had heard of mothers giving formula milk to babies under 6 months of age, either alongside breastmilk or as a replacement. This was typically 1–2 times a day (morning and evening), commencing when the baby is 1–3 months old (Quote B6, Table 3). Of note, nurses in Bishkek believed more mothers use only formula milk referring to “several” mothers.
Health workers described recommending and supporting women with exclusive breastfeeding during antenatal appointments and classes as well as in post-natal visits/check-ups at home or the health facility (Quotes B7-B9, Table 3). Most believed that both family doctors and nurses were responsible for providing this support, although the health workers in Kara-Say city (Oshskaya oblast) said this work mainly fell to nurses. They also suggested that the “mothers’ schools” (antenatal classes) could be better organised and more fully staffed. Health worker support comprised promoting the benefits of breastfeeding, providing advice, answering questions as well as guidance on breastfeeding techniques (described further in Skills in supporting women to breastfeed exclusively). Providing written information appeared to be less common. Health workers also tried to educate and encourage mothers who were using alternate infant feeding practices to try to exclusively breastfeed (Quote B10, Table 3).
Mothers’ accounts of their interactions with health workers reflected those of the health workers. Most recalled receiving advice, guidance, and practical support from a variety of health workers (e.g. family doctor, nurse, gynaecologist, paediatrician) at multiple timepoints (Quotes B11, B12, Table 3). Also consistent with health workers’ accounts was the scarcity of written information (Quote B13, Table 3; mentioned also in Availability of tools and resources).
Capability
Capability relates to mothers’ and health workers’ knowledge of exclusive breastfeeding and its benefits, knowledge of alternate infant feeding practices and associated risks, mothers’ physical skills and ability to breastfeed and health workers’ skills in supporting exclusive breastfeeding.
Knowledge of exclusive breastfeeding
Most, but not all, mothers across all infant feeding practices demonstrated understanding of what exclusive breastfeeding is, why it is recommended, and were aware of the health and nutritional benefits for mothers and babies. They knew about breastfeeding from talking to their family doctor, nurse, or paediatrician and seeing information on social media (Instagram, Facebook, from their health facility), the internet (including YouTube for learning breastfeeding technique), TV commercials and UNICEF materials (Quote C1, Table 4). Mothers wanted information with clear, consistent messages, from pregnancy onwards, focused on topics such as good nutrition to stimulate milk production, how to overcome perceived low supply of milk, the risks of giving formula and videos on good breastfeeding technique.
All health workers demonstrated good understanding of exclusive breastfeeding e.g. the benefits, the recommendations, how to overcome challenges, practical techniques. Most had received training on infant feeding (including exclusive breastfeeding), either during their medical/nurse training, as part of ongoing professional development e.g. BFHI training, refresher course run by Kyrgyz State Medical Institute for Retraining and Advanced Training. Many also mentioned informal training from colleagues. A few suggested that regular training updates were needed for health workers, to ensure that clear and consistent information was shared with women during pregnancy, birth, and post-natal interactions.
Knowledge of alternate infant feeding practices
Important knowledge gaps and misperceptions were evident for mothers using alternate infant feeding practices. Mothers who supplemented breastfeeding with additional fluids/solids did not seem aware of the risks and thought it was necessary to supplement for the baby to hydrate, achieve satiety and/or alleviate constipation (Quotes C2 and C3, Table 4).
Similarly, those who supplemented breastfeeding with formula or switched to formula understood that breastmilk was optimal but lacked awareness of the risks of using formula. Common misconceptions were that their breastmilk was insufficient or ‘bad’ and supplementing with formula (once or twice a day in the morning and evening) was needed to satiate their baby and improve their sleep. There also appeared to be limited awareness that further suckling helps to increase the mother’s supply of breastmilk and that giving additional fluids/solids/formula interrupts the natural supply and demand process (Quote C4, Table 4).
By contrast, health workers appeared to have a good understanding of the risks associated with alternate infant feeding practices and communicated these to mothers.
Physical skills and ability for breastfeeding exclusively
Mothers across all four infant feeding practices mentioned some physical challenges of breastfeeding. Importantly those mothers in the exclusive breastfeeding and additional fluids/solids groups who had difficulties managed to overcome them. For example, when they perceived they had a lack of milk, they continued to breastfeed to stimulate the milk supply, or they massaged and used salve to manage cracked nipples (Quote C5, Table 4). In contrast, the mothers who switched to formula who described the same challenges, were unable to resolve them (described in Emotions).
Health workers acknowledged the difficulties some mothers face with breastfeeding technique, i.e. positioning, latching on, suckling (Quote C6, Table 4). They also suggested that mental or physical health challenges i.e. depression, anxiety, tuberculosis, HIV could negatively impact on mother’s ability to breastfeed (Quote C7, Table 4).
Skills in supporting women to breastfeed exclusively
Most health workers appeared competent in their knowledge and communication skills to recommend and support women to breastfeed exclusively. There was clear acknowledgment of the importance of explaining the health, nutritional and convenience benefits of exclusive breastfeeding to mothers and offering explanations e.g. how the baby feeds, the difference between foremilk and hindmilk; as well as providing advice e.g. on frequency and duration, how to prevent mastitis. Health workers also described teaching, observing, and correcting breastfeeding techniques, sometimes using a doll with areoles, pacifiers, or an artificial breast (corroborated by mothers’ accounts). They explained why additional fluids/solids were unnecessary, e.g. crying can mean many things (not just thirst or hunger), breastfeeding is very rarely contraindicated. They highlighted the risks for the baby and offered advice for breastfeeding challenges (Quote C8, Table 4).
Motivation
Motivation barriers and drivers relate to mothers’ and health workers’ attitudes to infant feeding practices and mothers’ emotions.
Attitudes towards infant feeding practices
Consistent with their knowledge (described in Knowledge of exclusive breastfeeding) most mothers expressed positive attitudes towards exclusive breastfeeding and their perceptions of the benefits, typically focused on infant nutrition and health, were clear drivers. Those who went on to use alternate infant feeding practices did this because they believed exclusive breastfeeding to be insufficient to hydrate and/or satiate their baby or they believed solids (in addition to breastmilk) were good for the baby e.g. bananas are rich in vitamins, or apples alleviate constipation. Common explanations for supplementing or switching to formula were persistent breast problems (sore/cracked nipples) and the belief their baby was still hungry after breastfeeding because of a perception of low milk supply and/or the baby was crying or not sleeping. Some of these beliefs may be grounded in a lack of knowledge or misperceptions (as described in Knowledge of alternate infant feeding practices) (Quotes C2-C4, Table 4).
Health workers were highly positive toward exclusive breastfeeding and were clearly motivated to support mothers to breastfeed. They believed in the benefits of exclusive breastfeeding for the first 6 months of life mentioning health benefits to the baby and the mother, the mother-baby connection; as well as convenience and finance. Moreover, they did not see any disadvantages of exclusive breastfeeding, or benefits of alternate infant feeding practices (Quote M1, Table 4).
Emotions
Mothers who supplemented with formula expressed an inability to resolve the physical challenges they encountered with breastfeeding. This meant these challenges were viewed as persistent problems, prompting anxiety, undermining mothers’ confidence in breastfeeding culminating in the belief that formula was needed to satiate the baby (Quote M2, Table 4).
Around half of the mothers reported feeling uncomfortable about breastfeeding in public places, explaining they felt ashamed, shy, as well as concerned about hygiene and the risk of catching viruses (Quote M3, Table 4).
Sociocultural opportunity
Sociocultural opportunity factors relate to the socio-cultural context for breastfeeding, specifically health workers’ views related to social and cultural demands, and mothers’ views on social support and pressure.
Social and cultural demands
Discussions with health workers about sociocultural opportunity focused on the influence of the formula industry on their professional practice. Those from Oshskaya and Narynskaya oblasts were adamant they are not visited by industry representatives, with doctors and nurses in Uzgen district indicating this had happened in the past, but not since they were collaborating with the BFHI. (Quote SO1, Table 5). A key difference was evident for the doctors in Bishkek who were currently being visited by these representatives, confirmed by the nurses (Quote SO2, Table 5). They said that marketing of formula is “prohibited” in health facilities but found it useful to know about these products for the mothers who need them.
Social support and pressure
There were clear differences in social support and pressure for exclusive breastfeeding across the infant feeding groups. Mothers who had exclusively breastfed for 6 months described an entirely positive social environment. They had all been encouraged by their family (husband and extended family) and health workers to exclusively breastfeed, mentioning family members had offered advice as well as practical help with household chores or looking after older children. Significantly they had not experienced any advice or pressure to give their baby additional fluids, solids, or formula (Quote SO3, Table 5). They also appeared to have friends who believed in the importance of exclusive breastfeeding with whom they shared experiences and challenges.
The social environment was more mixed for the mothers using alternate infant feeding practices. Whilst they received some encouragement and practical help to breastfeed, they had all been advised by friends and family to supplement with fluids, solids or formula or switch to formula (Quotes SO4, SO5, Table 5). Several had also been advised by a health worker to supplement at some point. Whilst health workers suggested that mothers’ mothers-in-law were particularly influential in these infant feeding decisions (Quote SO6, Table 5), this was not evident in the mothers’ accounts.
A few health workers commented that sometimes family members take on childcare of babies as young as 2 months when mothers return to work, or migrate abroad for work, meaning that alternate infant feeding practices occur (Quotes SO7, Table 5). No mothers talked about expressing milk for this purpose.
Physical opportunity
Physical opportunity factors related to availability of tools and resources, convenience, and legislation linked to breastfeeding and formula for health workers, and mothers returning to paid work.
Availability of tools and resources
Most health workers felt they had practical tools and resources to teach women about breastfeeding, such as a baby doll, model breast, visual aids (posters), booklets. A few doctors in At-Bashy district (Narynskaya oblast) and Bishkek expressed the need for more tools, such as videos, breast pumps and more baby dolls to help them support women, as well as specific breastfeeding rooms in healthcare facilities (Quote PO1, Table 5). As discussed above (in Behaviour) both health workers and mothers mentioned a lack of written information for mothers.
Convenience
Health workers reported having multiple opportunities as part of their scheduled appointments with pregnant women and mothers of infants to support them with breastfeeding. Crowded clinics and lack of time and space for these conversations was only mentioned as an issue for a small minority working in the At-Bashy district (Narynskaya oblast) and Kara-Say city (Oshskaya oblast) (Quote PO2, Table 5).
Legislation related to breastfeeding and formula
Health workers mentioned a wealth of legal documents from the Ministry of Health that provided a national imperative to support exclusive breastfeeding in Kyrgyzstan, e.g. Decree for the Food Security and National Programme (Quote PO3, Table 5). These were overwhelmingly viewed positively and seen to guide all health workers in their everyday practice.
Returning to paid work
For all mothers in the study, returning to work was not seen as a barrier to exclusive breastfeeding, although a few felt that maternity leave policies (70 days before childbirth and 56 days after childbirth [33]) should create more opportunities for mothers to stay at home rather than return to work. Most were either still on maternity leave or not in paid employment. A few had returned to work after the baby was 6 months old.



Comments (0)