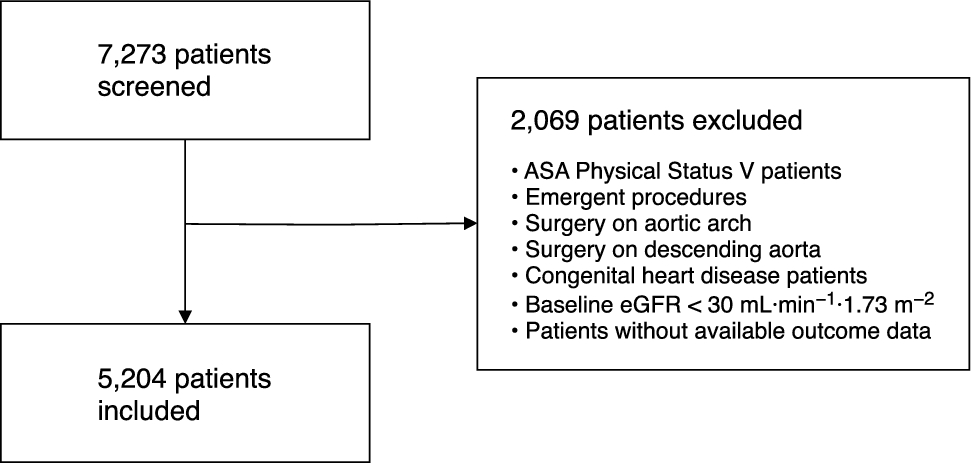
In this retrospective observational study of 5,204 cardiac surgery patients, AKI occurred in 15% of patients, with 77% classified as KDIGO stage 1, 11% as stage 2, and 12% as stage 3. Red blood cell transfusion, but not plasma or platelet transfusion, was significantly associated with the development of AKI. We observed a dose-dependent relationship between RBC transfusion and AKI severity, with patients receiving more than two units of RBCs being at a significantly higher risk of developing KDIGO stage 2–3 AKI.
Cardiac surgery-associated AKI is a multifactorial condition influenced by patient-related factors, surgical complexity, and modifiable management practices. The contribution of these individual risk factors is reflected in the variability in AKI frequencies reported across studies, which ranges from 20% to 30%.1,23,24,25 Despite a comparable patient profile in terms of age, comorbidity burden, and CPB duration to the Copenhagen cohort, where AKI occurred in 28% of patients, we observed a lower AKI occurrence of 15% in our study.9
Patients who developed AKI in this study had similar risk factors to those reported previously, including older age, reduced preoperative kidney function, extended CPB duration, and lower intraoperative hemoglobin levels—factors that create a high-risk environment for AKI. Among modifiable factors, transfusion practices—particularly RBC transfusion—may represent a key area for future prospective studies evaluating targeted interventions to potentially reduce AKI risk.
Red blood cell transfusion practices in cardiac surgery follow the transatlantic patient blood management guidelines.16,26 Nevertheless, the frequency of transfusion varies significantly across cardiac centres, ranging from 10% to 80%, likely in part reflecting differences in patient populations, surgical procedures, institutional practices and culture, and evolving transfusion protocols. When compared with the Copenhagen cohort, our study had a higher proportion of patients receiving platelet transfusions (32% vs 8%). This may reflect the fact that point-of-care platelet tests were used in all patients at our centre in Toronto, and only on demand in the Copenhagen population. This difference may also reflect a more coagulopathic patient population in Toronto, contributing to increased RBC transfusions. Despite the higher transfusion frequency in our cohort, the AKI occurrence was lower than in previous studies of cardiac surgery patients.9,23,24
The role of plasma and platelets in AKI development remains controversial. Some studies have suggested an association between procoagulant transfusions and AKI, but these associations often disappear after adjusting for the co-administration of other blood products and may be largely confounded by the association of large volume blood loss with adverse outcomes.9,24,27 Consistent with these findings, we did not observe any significant association between plasma or platelet transfusions—either alone or in combination—and AKI risk. In contrast, RBC transfusions remained a significant risk factor for AKI, even after adjusting for other blood products, aligning with previous observations.9
Nonetheless, significant bleeding requires balanced transfusion of RBCs, plasma, and platelets to restore hemostasis and hemodynamic stability. Although platelet and plasma transfusions were not independently associated with AKI risk in our study, the use of goal-directed hemostasis with alternative products, such as prothrombin complex concentrate, has been proposed as a strategy to reduce RBC transfusion requirements and AKI risk.28
A major challenge in evaluating AKI risk factors lies in the difficulty of disentangling the individual factors, as many are strongly interrelated. For example, patient vulnerability (i.e., anemia), prolonged CPB duration, volume of hemorrhage with accompanying hemodynamic compromise, and further bleeding complications, such as re-operative hemorrhage, all increase both the need for RBC transfusion and the risk of AKI.29,30 This raises the potential for confounding by indication, where the need for transfusion reflects the severity of the patient's condition rather than the direct effect of the transfusion itself.
To gain a clearer understanding of the impact of RBC transfusion, we employed inverse probability weighting to adjust for potential confounding factors, such as intraoperative hemoglobin levels and CPB duration, as well as age and preoperative eGFR as mediators. After statistical adjustment, the association between RBC transfusion and AKI remained robust across all stages.
While AKI development was not confined to transfused patients, it is important to note that approximately 10% of patients who did not receive any transfusions still developed AKI in our study, compared with 21% in the Copenhagen cohort.9 This further underscores the complexity of AKI pathogenesis, with both modifiable and nonmodifiable factors contributing to its development. Nonetheless, focusing on modifiable factors, particularly RBC transfusion and the volume administered, offers an opportunity to improve patient outcomes. Randomized clinical trials (RCTs) investigating optimal transfusion practices have primarily focused on hemoglobin thresholds as triggers for transfusion, given the ethical challenges of randomizing patients to no transfusion.31,32 Nevertheless, the frequent use of RBC transfusions (> 50% of patients in the restrictive arm) in these RCTs reduces the signal-to-noise ratio thereby blurring the effect of RBC transfusion on AKI risk.
Our study has several limitations. Owing to its retrospective nature, we cannot establish causality. In our weighting model, we used lowest intraoperative hemoglobin and total CPB time as surrogates for transfusion risk, recognizing that these final values may not have been known at the time of initial transfusion decisions. Additionally, variations in transfusion practices and thresholds between centres could affect the generalizability of our findings. Despite validating findings across two distinct cardiac centres, results may not generalize to all practice settings, particularly nonacademic or resource-limited institutions. We only assessed transfusions administered on postoperative day 0 and 1 to directly relate them to the index surgery and ensure comparability with the Copenhagen study. Nevertheless, a sensitivity analysis in the Toronto cohort, including transfusions from day 0–7 did not alter the conclusions. Similarly, our additional sensitivity analysis incorporating further clinical covariates demonstrated the robustness of our findings despite these acknowledged limitations.
Finally, AKI was primarily determined by SCr levels, as urine output data could not be reliably retrieved from the databases. While this may have led to an underestimation of the true AKI occurrence, the consistency of RBC transfusion volume as a key modifiable risk factor for AKI following cardiac surgery remains evident.
Future RCTs examining the impact of comprehensive patient blood management to improve perioperative hemoglobin levels, including long-term interventions offered post-operatively, may offer further insights on potential risk modification and the strength of the causal relationship between hemoglobin levels, RBC transfusion avoidance, and postoperative complications.33
Conclusions
This study from Toronto General Hospital corroborates findings from a previous study using a cohort from Copenhagen. Both studies found that RBC transfusion is associated with an increased risk of AKI development in a dose-dependent manner, both when administered alone and in combination with other blood products. Determining whether RBC transfusion and transfusion volume is a critical modifiable risk factor in cardiac surgery patients, and whether focusing on minimizing transfusion needs through alternative strategies may reduce the incidence of AKI, requires further prospective studies, some of which are already underway.33,34




Comments (0)