This study evaluated the therapeutic potential of Crocin in alleviating diabetic peripheral neuropathy. Our findings demonstrated that although there were no significant differences between the Crocin and placebo groups at baseline, notable improvements emerged in the Crocin group during the follow-up period. Specifically, significant reductions in pain severity were observed in the Crocin group, as evidenced by lower VAS scores at weeks 6 and 9. Furthermore, by week 9, the Crocin group exhibited significantly lower TSS and MNSI-Q scores compared to the placebo group. Therefore, Crocin may be effective in reducing diabetic neuropathy pain in patients with DPN after eight weeks of treatment.
Diabetic neuropathy is a debilitating complication of diabetes, affecting sensory, motor, and autonomic nerves. It typically presents with symptoms such as burning pain, paresthesia, and numbness, particularly in the lower limbs. These symptoms tend to worsen at night, impairing patients’ sleep and quality of life. Effective management of DPN remains a clinical challenge and is primarily focuses on symptom relief and prevention of further nerve damage [25]. Chronic hyperglycemia is thought to play a key role in the pathogenesis of DPN by inducing mitochondrial dysfunction, promoting production of reactive oxygen species (ROS), impairing neuronal blood flow, reducing the availability of neurotrophic factors, and slowing nerve conduction. Without proper glycemic control, these changes can lead to irreversible damage to the peripheral nervous system.
Natural compounds, including plant-derived substances, have long been investigated for their neuroprotective properties. Crocin, a carotenoid derived from Crocus sativus (saffron), has attracted considerable attention due to its broad pharmacological profile. Previous studies have shown that Crocin possesses antioxidant, anti-inflammatory, anti-apoptotic, and neuroprotective properties. It also appears to improve cognitive function, reduce stress, and protect against DNA damage and neuronal injury induced by oxidative stress or cerebral ischemia [26,27,28,29,30].
Several studies have investigated the effects of saffron and its active ingredient, Crocin, on various types of pain, including neuropathic pain. Our findings are consistent with preclinical studies indicating the efficacy of Crocin in models of neuropathic pain. For instance, in chronic constriction injury (CCI) models, both aqueous saffron extracts and Crocin reduced oxidative stress, inflammation, and neuronal apoptosis [31]. Amin et al. also demonstrated the effectiveness of saffron extracts in alleviating various forms of nerve pain, highlighting their potential as adjuncts to standard pharmacotherapy [32]. Moreover, another study revealed that Crocin, at a dose of 80 mg/kg, mitigated nerve damage and reduced pain responses in a cold allodynia test [33]. These findings are in agreement with our study, indicating that Crocin’s reduction of neuropathic pain after eight weeks may be attributed to its neurodegenerative effects.
Similarly, another investigation reported that saffron and Crocin extract (30 mg/kg) attenuated thermal hyperalgesia and mechanical allodynia by day 26, with these effects sustained through day 40. However, the study also reported that Crocin was ineffective at a lower dose (15 mg/kg), suggesting a dose-dependent response [34]. In our trial, only a single daily dose of 15 mg was administered, and dose-response relationships were not explored. Beyond diabetic neuropathy, Crocin has shown promise in chemotherapy-induced peripheral neuropathy (CIPN). Evidence suggests that Crocin may alleviate CIPN symptoms with fewer side effects compared to traditional agents such as antidepressants, lamotrigine, and gabapentin [35].Several mechanisms may contribute to Crocin’s effectiveness in reducing diabetic neuropathic pain. One proposed mechanism involves the modulation of intracellular calcium levels. Crocin has been shown to inhibit the influx of extracellular Ca2+ and release Ca2+ from intracellular stores in the endoplasmic reticulum, thereby reducing intracellular calcium concentrations [36]. This calcium reduction may lead to vasodilation and subsequent tissue hyperemia, which could improve peripheral nerve perfusion [37].
Oxidative stress and ROS overproduction are pivotal in the pathogenesis of neuropathic pain. There is substantial evidence supporting the role of antioxidant agents in alleviating neuropathic pain. Both ethanolic and aqueous extracts of saffron, Crocin in particular, exhibit significant antioxidant activity by reducing lipid peroxidation. These compounds inhibit deoxyribose degradation in red blood cell membranes and liver microsomes, thereby preserving cellular integrity. Recent studies have also demonstrated that saffron and Crocin can protect against hippocampal oxidative damage and cognitive dysfunction induced by chronic stress, suggesting that Crocin’s antioxidant and potential glucose-lowering properties may play a central role in alleviating neuropathic pain [38].
Furthermore, Crocin has been shown to reduce acrylamide-induced neurotoxicity in Wistar rats by attenuating oxidative stress. Dose-dependent administration of Crocin suppressed lipid peroxidation and increasing glutathione (GSH) levels, further confirming its neuroprotective effects [39].
In PC-12 cells, Crocin inhibited lipid peroxidation formation, partially restored superoxide dismutase (SOD) activity, preserved neuronal morphology and reduced apoptotic cell death, highlighting its cytoprotective and anti-apoptotic properties [40,41,42].
Another proposed mechanism by which Crocin reduces diabetic neuropathy pain is its involvement in glycemic control and glucose metabolism [33, 43]. A study by Kianbakht et al. demonstrated that saffron increased blood insulin levels without causing liver or kidney toxicity in diabetic rats, implicating Crocin, Croscetin, and Safranal in this effect [44]. Additional studies have shown that Crocin reduces blood glucose levels and increases the expression of phosphoenolpyruvate carboxykinase 1 (PCK1), a key enzyme involved in gluconeogenesis and glucose homeostasis [45]. Moreover, the neuroprotective effects of Crocin and Safranal may therefore be partially mediated through their anti-hyperglycemic and antioxidant properties [46]. While our study did not evaluate blood glucose levels, these findings align with the observed reduction in neuropathic symptoms.
Study limitations
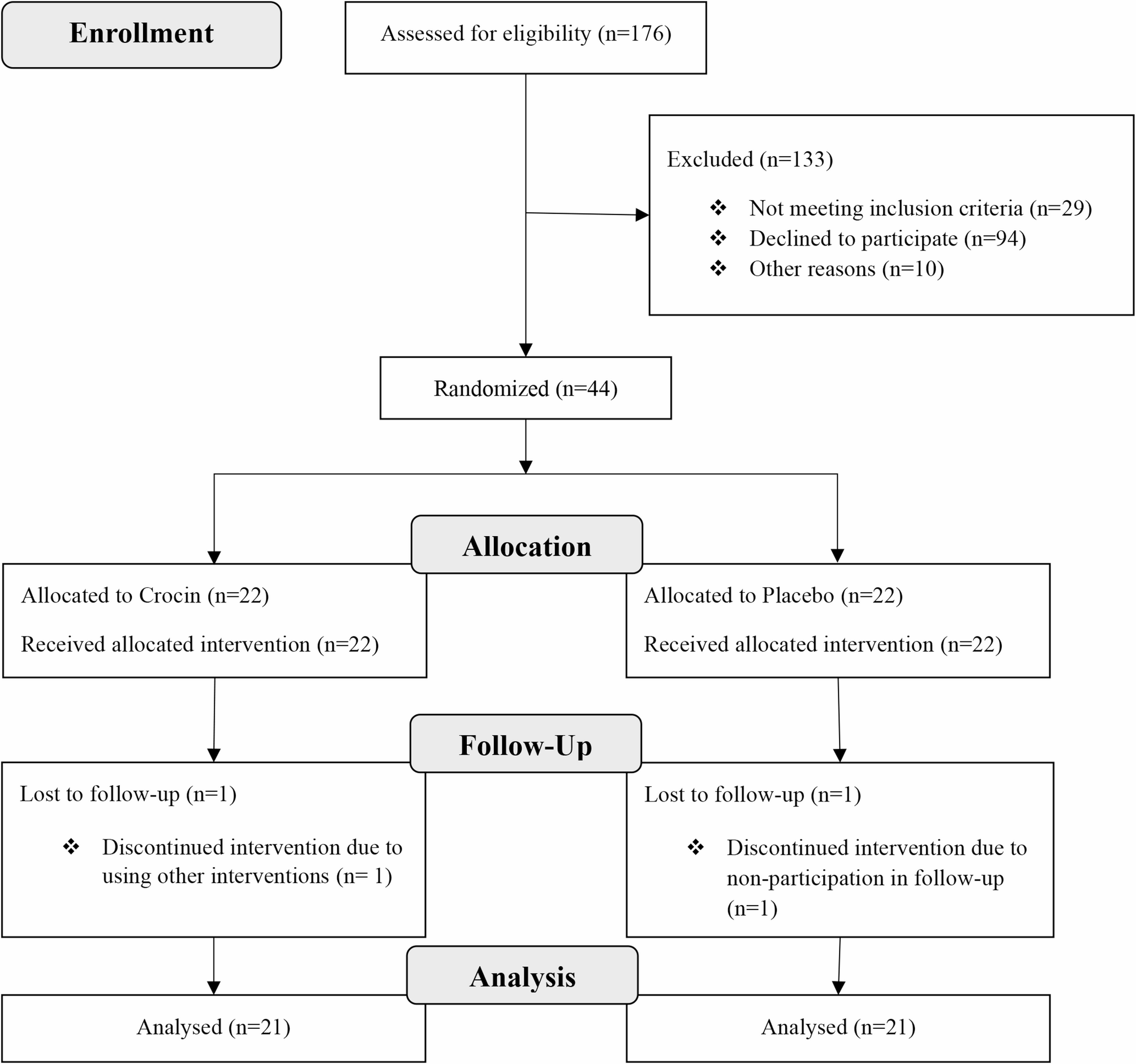
While this clinical trial yielded promising findings, the limitations of the study should be acknowledged when interpreting the results. First, the sample size was relatively small. Although 176 individuals were assessed for eligibility, only 42 patients ultimately completed the study, which may affect the generalizability of the findings. Second, the study was limited to 12 weeks, potentially insufficient to assess the long-term efficacy and safety of Crocin in managing diabetic neuropathy. Additionally, the primary outcome measures included patient-reported instruments such as the MNSI, which, despite being validated tool, may be subject to response bias and variability in individual perception of symptoms. The use of a single fixed dose (15 mg/day), chosen based on previous studies, represents another limitation. The lack of dose comparison restricts our understanding of the optimal therapeutic dose or potential dose-response effects. While nerve conduction and use of objective diagnostic tools are ideal for assessing diabetic neuropathy, since the present study was a preliminary trial, our focus was on evaluating patient-reported outcomes using validated clinical scales (TSS, MNSI, and VAS).
It should be noted that although the mean reduction in symptom score was statistically significant, the absolute change may be considered modest in terms of clinical practice and the clinical relevance of these changes should be interpreted with caution. Therefore, further trials incorporating objective neurological assessments and validated clinical benchmarks are warranted to confirm whether these changes translate into meaningful functional or quality-of-life improvements for patients with diabetic neuropathy.
Another limitation of our study was not evaluating the specific anatomical sites of peripheral neuropathy, separately. Although the validated instruments applied in this clinical trial primarily reflect symptoms in the lower limbs which are commonly affected in diabetic neuropathy, we did not collect data on the precise localization (e.g., distal versus proximal involvement, or foot versus hand symptoms). To determine treatment effects based on the location of neuropathic pain, future studies with detailed mapping of neuropathic involvement should take this limitation into account.
Future research should include larger sample sizes, extended follow-up durations, exploration of various dosing regimens, and objective electrophysiological assessments. Investigating the precise molecular mechanisms by which Crocin alleviates diabetic neuropathy will provide deeper insights, particularly its role in neuroinflammatory pathways, oxidative stress, and intracellular calcium signaling. Furthermore, studies assessing Crocin in combination with other conventional treatments (e.g., analgesics, anti-inflammatories) may elucidate potential synergistic effects.





Comments (0)