This early economic evaluation assesses the potential cost-effectiveness of E-MATVR compared with E-MATE among male athletes on the basis of experiences in the feasibility trial [6]. Results support and inform the design and conduct of a future RCT. Compared with E-MATE, E-MATVR had higher expected benefits and costs, but expected costs outweigh WTP estimates, yielding negative net benefit. The higher costs were attributable to the capital costs associated with developing and delivering the intervention. Scenario analyses demonstrated whether intervention delivery costs were reduced via alternative delivery strategies in the RCT, and if WTP estimates remained constant, E-MATVR could be considered cost-effective. Furthermore, distributing costs across more participants (as would be in the case in the RCT) would reduce costs and increase net benefits, suggesting E-MATVR could be considered cost-effective in the future.
This analysis uses results from a feasibility trial to conduct an early economic evaluation. Such evaluations do rely on small sample sizes with high cost/high variable populations, risking negative outcomes, which some argue could jeopardize future applications for RCTs in otherwise clinically effective interventions [28]. Despite these limitations, economic evaluations conducted alongside feasibility studies can help develop or refine service plans and outcome measures for RCTs [29]. They can be a cost-effective means of determining whether an RCT is feasible, thereby avoiding inefficient and costly studies/trials on interventions that are unlikely to be considered cost-effective [30, 31]. Therefore, iterative and early economic evaluations can yield efficiency savings by increasing the speed of decision-making, reducing uncertainty around cost-effectiveness estimates [29], and ensuring all eventualities are considered before the main trial begins [30]. This early cost–benefit analysis of E-MATVR compared with E-MATE demonstrates that the intervention cannot be considered cost-effective in its current form. A RCT should consider alternative delivery modifications to reduce costs and to determine whether WTP estimates remain constant.
Digital health interventions are increasingly used in public health initiatives and can be useful to capture traditionally hard-to-reach audiences, such as young adult men. However, as this study shows, digital interventions have high fixed costs associated with their development [32]. Traditionally dismissed as a sunk cost, they have an associated opportunity cost. Given the limited resources available for research on developing and implementing public health interventions, acknowledging and estimating intervention development costs are important and can inform future research priority-setting and resource allocation decisions. Here, when including capital costs, negative net benefit increased. However, in a RCT intervention, costs would be averaged across greater patient numbers, as explored in the sensitivity and breakeven analyses.
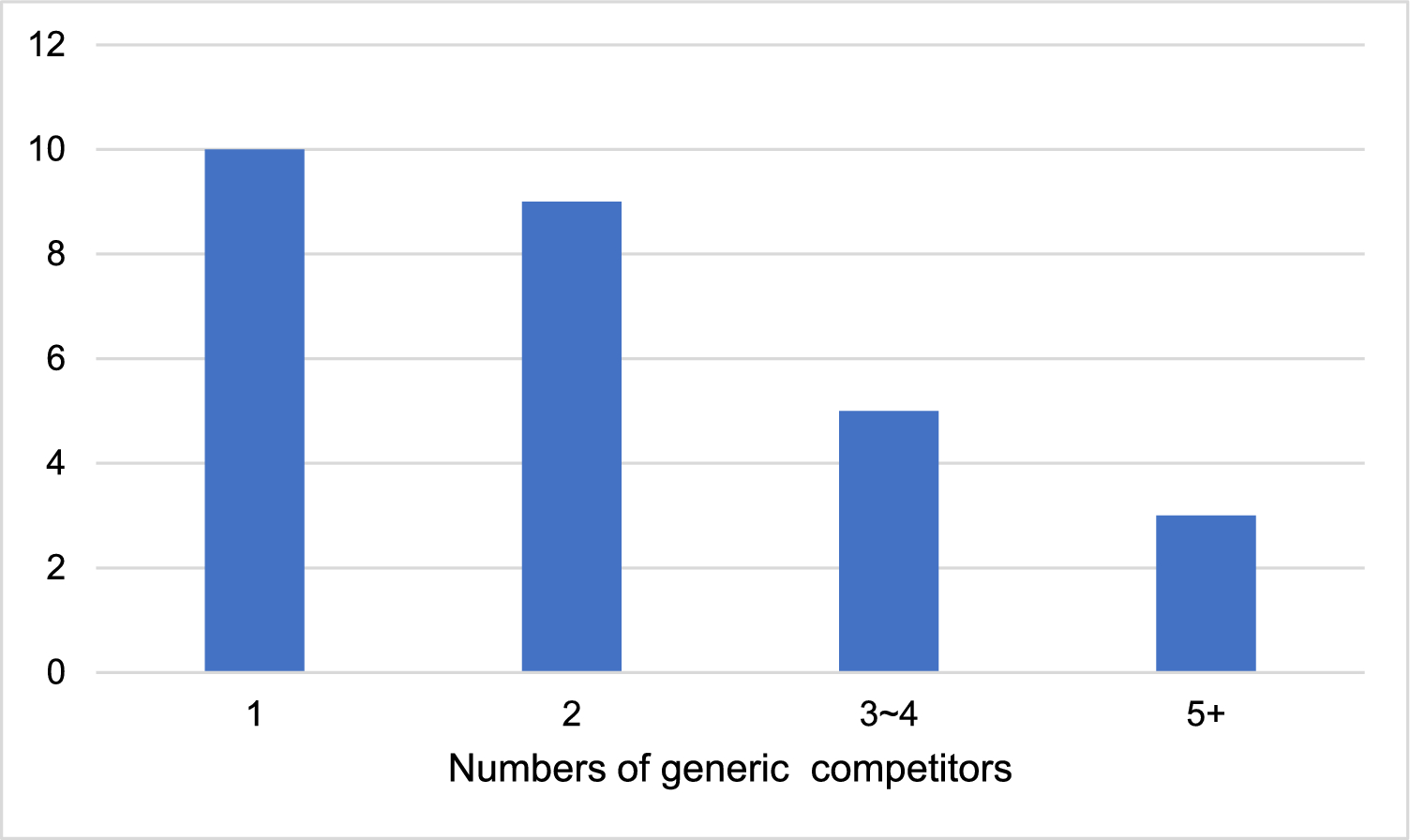
In addition, regarding costs, feasibility studies can provide an opportunity to examine the resource use associated with an intervention and savings or other service use impacts [28, 30]. Here, there were only four responses to the resource use questionnaire, as respondents were advised to skip that question if it did not apply. The low response here may not be surprising given the short follow-up time frame and high educational attainment among the group (85% had third level education) [33]. However, to ensure that blank responses correspond to “zero” use, future iterations should include a compulsory question to clarify. Here the follow-up period is short given the feasibility nature of the trial, which reduces the time horizon considered. Any potential savings (accruing from early detection, for example) would be in the longer term. Future economic evaluations, for example, using data from a RCT, could contribute to decision analytical modeling to investigate potential long-term savings from an early intervention. It was beyond the scope of the feasibility study to consider this (from both power and time horizon perspectives). Nevertheless, results of the sensitivity analysis do illustrate how varying perspective, the scope of costs included, and modifications to intervention delivery impact expected net benefit and probability of being cost-effective. These inform future trial design and associated Health Economics Analysis Plans (HEAP).
This early economic evaluation estimated expected benefits using WTP to conduct the cost–benefit analysis. We acknowledge there are some limitations around the approach and sample. While the homogenous sample is ethnically representative of the GAA population, there is a lack of diversity in the sample (which is discussed in full in the process evaluation [6]). To consider the value of the intervention beyond this group, a more diverse sample of men, in more heterogenous environments, is warranted. This may improve the external validity of the WTP results.
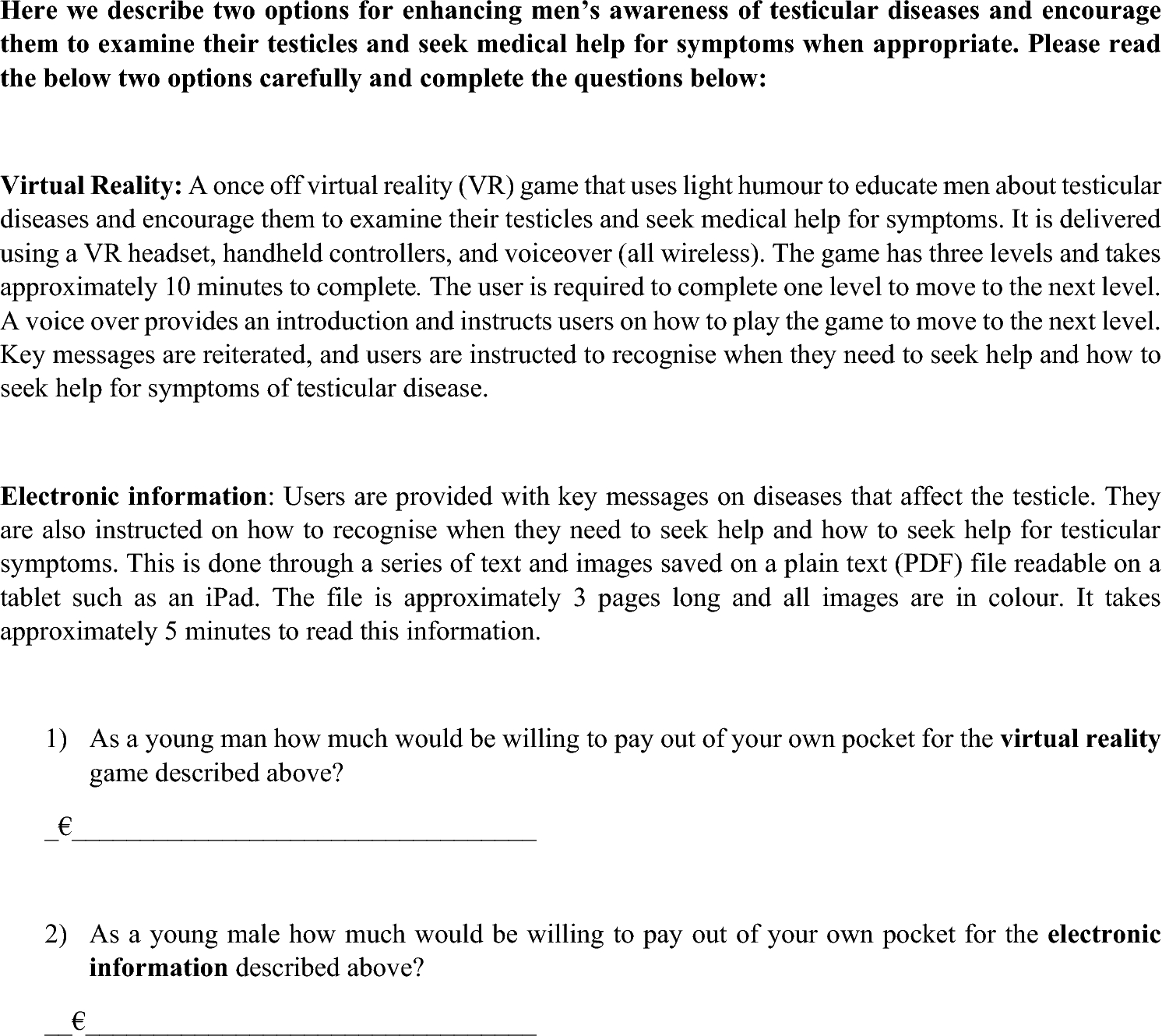
We acknowledge that the WTP analysis only employed open-ended questions, which have no upper and lower bounds (contributing to lower internal validity). While routinely adopted in the digital health literature [15, 17], we acknowledge there are limitations with its use, which are evidenced in the distribution of the data, which is skewed. In addition, the order of the WTP questions were not varied to determine whether the order impacted results. Unfortunately, the process evaluation conducted for the feasibility study [6] did not explicitly examine experiences with the WTP questions, which was a missed opportunity. This is worth considering in a future RCT.
We did include explicit information on risk perception, which was not statistically significant in the regression analyses. Given the profile of the participants (GAA players and coaches) they would be susceptible to testicular injury and consequent disease [5, 6]. The low overall perceived risk of testicular diseases is a barrier to early help-seeking for cancer symptoms among men. One explanation is that testicular diseases are often diagnosed in younger men who are relatively healthy and who have limited to no contact with the healthcare system [5]. In addition, two of the 74 participants reported a personal history of testicular disease. These were not statistically significant in the regression analyses. As discussed in the process evaluation of the feasibility study [6], inclusion of participants who have a personal and/or family history of testicular disease ought to be considered in the design of a future RCT.
Albeit the small sample, the WTP data collected here had a high response rate, suggesting it would be feasible to collect in a full RCT. We acknowledge that subjectivity and context bias, as well as the role of income, are limitations when using this type of measurement, as may be the case with this restricted sample. There is also a risk that reported WTP preferences, when part of a survey, might not truly reflect real-life behaviors, causing external invalidity. Consequently, CVM can yield hypothetical inflated responses with scope and nesting effects [34]. Nevertheless, the high absolute values are consistent with previous literature that younger, higher-income, male individuals are willing to pay more for digital services [35]. Overall, without a market for the intervention, CVM was suitable for collecting WTP estimates, allowing a direct valuation suitable for a cost–benefit analysis. This gives an understanding of what participants value in future health services. In theory, the costs and effects observed in a feasibility study can also be used in value of information analysis to explicitly examine whether the cost of a RCT is worthwhile [28]. However, as an expected difference in quality of life was not expected between the two groups, utility data were not collected to facilitate a value of information analysis here.


Comments (0)