
Remember me

A decision-analytic model was developed, comprising a decision-tree model for the acute COVID-19 phase (30 days), followed by a lifetime Markov model. This structure follows that of a previously published cost-effectiveness model of molnupiravir in the US [15].
The target population was individuals aged ≥ 65 years with mild-moderate COVID-19 who were at risk of disease progression leading to hospitalization, in Japan.
Of this population, 82.4% were assumed to have acquired immunity due to at least one prior infection or vaccination, as per estimates from molnupiravir-treated individuals by Shinozaki et al. [16]. Cost effectiveness of molnupiravir versus best supportive care was primarily compared to a willingness-to-pay (WTP) threshold of ¥5,000,000 per quality-adjusted life year (QALY) gained. This threshold of ¥5,000,000 per QALY is a common benchmark for determining cost effectiveness in Japan [17].
The model compared molnupiravir with best supportive care only, even though several different treatments (nirmatrelvir/ritonavir and ensitrelvir) were recommended for outpatient COVID-19 in Japan (depending on the characteristics of the patient) [18]. The decision to exclude active comparators in our cost-effectiveness analysis of molnupiravir is based on two primary reasons. First, the rapid evolution of the COVID-19 pandemic requires the consideration of data from randomized-controlled trials (RCTs) and real-world evidence (RWE) to accurately assess the efficacy of antiviral treatments and identify the most beneficial populations. Significant variability in study design, enrollment periods, geographic regions, inclusion and exclusion criteria, patient characteristics, concurrent treatments, outcomes, and circulating variants complicates simple cross-trial comparisons. This variability can result in differences in placebo arm event rates. For a valid network meta-analysis, the assumption of transitivity—requiring no systematic differences between comparisons other than the treatments analyzed—must be met [19]. This assumption is both strong and restrictive, necessitating careful evaluation of its validity in our analysis context [20].
Second, we considered the current prescription trends in Japan. A substantial portion of COVID-19 outpatients, particularly among those aged 65 years and older, are not prescribed any antiviral medications during their treatment course. A recent report by Miyawaki et al. showed that 64.2% of this population did not receive guideline-recommended antivirals, with molnupiravir being the most commonly prescribed option at 31.5% [21]. Given this clinical reality, we justify our focus on molnupiravir and the second most common treatment option (best supportive care without antivirals) in our analysis, which aims to reflect standard clinical decision making in the real-world healthcare setting in Japan.
Additionally, adverse events or treatment-emergent adverse events were not examined as part of this model, as phase III clinical trial data and real-world studies support the efficacy and safety profile of molnupiravir [12, 16, 22, 23].
The cost-effectiveness model was developed in Microsoft Excel 365, with some calculations and functionalities also programmed in Visual Basic for Applications (VBA).
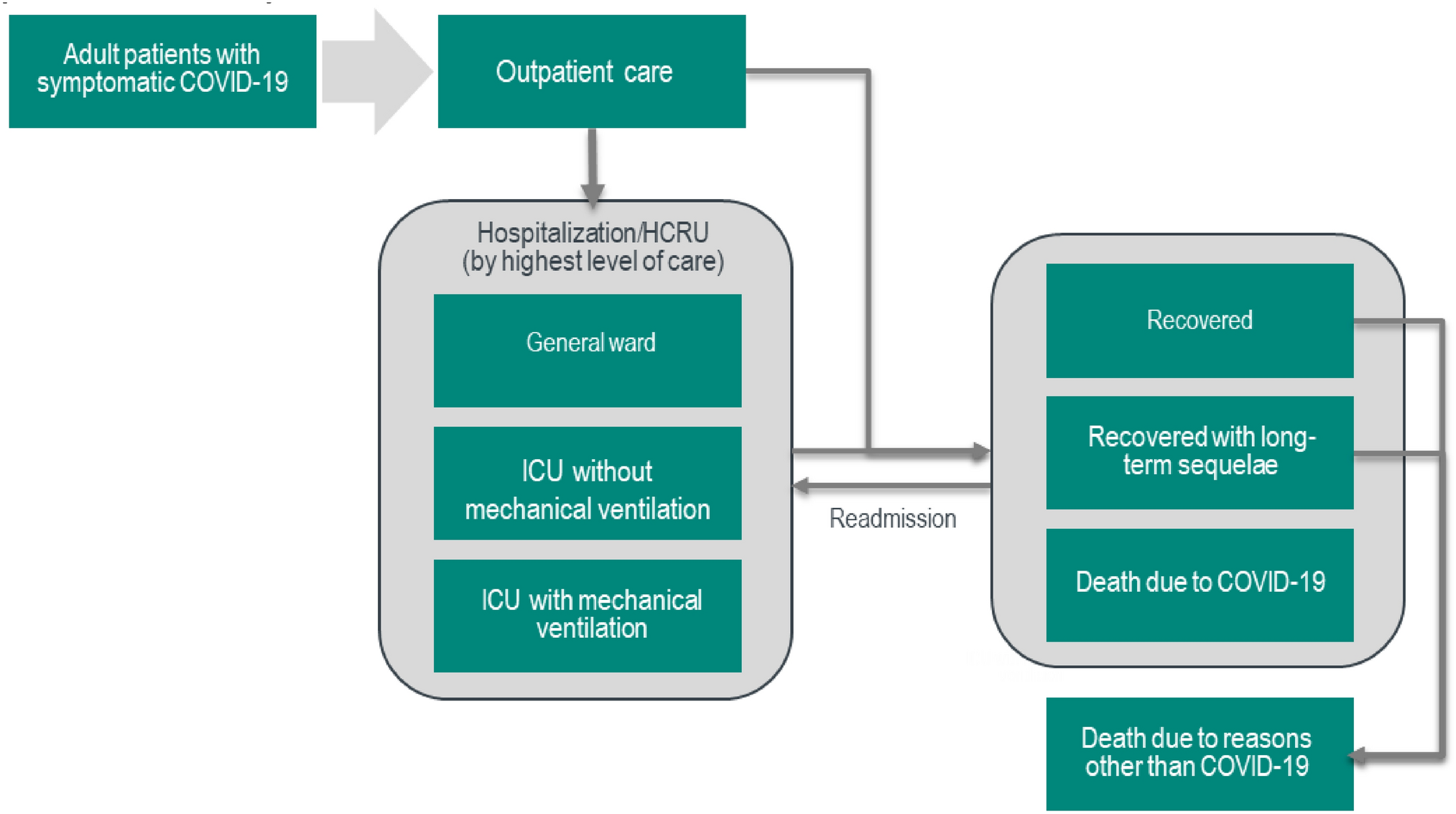
2.1 Model StructureAt model start, 100% of target patients, described previously, entered a decision-tree model for the acute COVID-19 phase (30 days), where patients begin in the outpatient setting and may subsequently be hospitalized (see Fig. 1). Those patients who are hospitalized may experience general ward care, intensive care unit (ICU) care, ICU care with mechanical ventilation, or death. After discharge from hospital, patients may recover completely, recover with long-term sequelae of COVID-19, be readmitted due to COVID-19 (within 60 days of initial hospitalization), or die due to COVID-19.
Fig. 1
Structure of cost-effectiveness model, comprising decision-tree model for acute COVID-19 phase, followed by lifetime Markov model. HCRU health care resource use, ICU intensive care unit
After the acute phase, patients entered a Markov model with a cycle length of 1 year. Patients moving from the acute phase without readmission or long-term sequelae continued as per the general population. Patients moving from the acute phase with readmission and/or long-term sequelae also experienced associated consequences throughout the Markov model. The model did not assume any reinfections. Patients were followed to death or 100 years, whichever occurred first.
2.2 Model InputsInputs used to parametrize the model were derived from a real-world data analysis using a large administrative database provided by Medical Data Vision Co., Ltd. Tokyo, Japan (in the case of patient characteristics and medical costs except for patients who underwent ICU care with mechanical ventilation and other related estimates) [24], and from ad-hoc literature searches and other research (for disease progression, medical costs for patients who underwent ICU care with mechanical ventilation, and utility estimates).
2.2.1 Baseline Characteristics InputsCharacteristics of the modelled population (see Table 1) were predominantly derived from a retrospective analysis of the Medical Data Vision (MDV) database in Japan [24]. The MDV database collates administrative data from more than 460 hospitals and 39 million patients, covering ~ 26% of acute care hospitals across Japan, as of April 2022. In the retrospective analysis that provided these estimates, records corresponding to patients diagnosed with COVID-19 (ICD-10 code U07.1) between January 2020 and June 2022 were identified, and data were extracted for key outcomes such as outpatient visits, emergency department visits, dates of hospitalization and discharge, procedures during hospitalization, prescribed drugs, discharge status, readmission, revisits due to post-COVID symptoms, and the healthcare resource utilization with the associated costs from the index date until a censoring event (i.e., death or end of patient record).
Table 1 Characteristics of the modelled population, from the MDV database and published sources [26,27,28]Of note, the baseline hospitalization rate parameter was sourced from a meta-analysis of RWE [25], which included published studies from the Omicron era [26,27,28], including proportions of individuals with prior immunity against SARS-CoV-2 either by prior infection or by vaccination that are similar to those observed in Japan for individuals aged ≥ 65 years (for example, Bajema et al. in 2022 reported that 85.2% of their sample had received at least one vaccination or prior infection, Xie et al. in 2023 reported 82.7%, and Van Heer et al. in 2022 reported 100%) [29].
While other hospitalization rate estimates were available specifically for ≥ 65-year-old patients in Japan from an alternative source [30], the RWE sources used were more similar to the modelled population in Japan in terms of age and vaccination status [16, 26,27,28].
In addition, a standardized mortality ratio of 1.5 was applied to the background mortality rate for those individuals who survived hospitalization, to model the increased mortality risk in hospitalized patients surviving the acute phase of COVID-19 based on the approach taken by Goswami et al. [15].
Other required parameters of the modelled population (see Table 1), including symptom duration in outpatients, number of outpatient visits, number of emergency department (ED) visits, proportion with ED visit, and proportion with readmission, were again derived from ≥ 65-year-old patients within the MDV database.
The prevalence of long-term sequelae in surviving patients was derived from a prospective population-based survey study conducted in an urban region of Japan in early 2023 [31]. Estimates stratified by severity of acute COVID-19 were mapped to the structure of the current model (‘asymptomatic’ to outpatient, ‘mild’ to general ward admittance, and ‘moderate’ to ICU or mechanical ventilation, respectively) to assign the prevalence of long-term sequelae reported in Table 2. In the model, long-term sequelae were defined as the following symptoms if persisting >2 months after the acute phase: fever, cough, fatigue, sore throat, chest pain, anorexia, brain fog, difficulty concentrating, anosmia, ageusia, shortness of breath, hair loss, muscle weakness, palpitations, sleep disorder, rhinorrhea, headache, joint pain and swelling, muscle aches, nausea/vomiting, abdominal pain, skin rash, eye-related symptoms, dizziness, erectile dysfunction, and menstrual change [31].
Table 2 Treatment effect of molnupiravir [25]2.2.2 Treatment Effect InputsThe treatment effect of molnupiravir on hospitalization and death was again parametrized using estimates from a meta-analysis by Mesfin et al. (2024), who collated real-world studies on the effectiveness of molnupiravir and nirmatrelvir + ritonavir against these outcomes (vs no antiviral treatment), up to 35 days, among vaccinated and unvaccinated non-hospitalized adults with COVID-19 (see Table 2) [25]. The use of these estimates from a meta-analysis (rather than from a single source) was considered to be a more robust option; however, various other estimates of treatment effectiveness were also tested in scenario analyses, for completeness.
As molnupiravir is an outpatient treatment, the model did not assume treatment effect after hospitalization. The model also did not consider any reduction in symptom duration. Additionally, the model did not consider any additive effect of vaccination and treatment.
The baseline risk of mortality from COVID-19 was affected by the highest level of care a patient reached (see Table 3). Therefore, this analysis modelled death averted due to COVID-19 hospitalization as an indirect effect of molnupiravir (through preventing hospitalization). These estimates were again derived from ≥ 65-year-old patients within the MDV database. For patients surviving beyond the acute phase, background mortality was calculated and applied according to standard Life Tables reflecting the Japanese population [32], to a lifetime horizon of age 100 years.
Table 3 Mortality risk by hospital setting for ≥ 65-year-old patients hospitalized with COVID-19, from the MDV database (see Model Inputs section; see electronic supplementary material)2.2.3 Health State Utility InputsAs no suitable COVID-19 health state utility values were identified in the published literature, data from a previously conducted de novo utility study were used to parameterize the model (see Table 5) [33]. Within that study, members of the UK general population (n = 500) completed the EQ-5D-5L questionnaire in response to written descriptions of COVID-19 health states [33]. For the purpose of this model, those EQ-5D-5L results were converted to utility values using the existing EQ-5D-5L value set for Japan developed by Shiroiwa et al. [34].
2.2.4 Cost InputsCost inputs for management of COVID-19 (see Table 4) were derived from the MDV database and Japan National Health Insurance (NHI) medical fee schedules [35], and a published source [36]. The NHI list price of molnupiravir (¥86,596 per course) was used [37]. Japan's healthcare system is characterized by universal coverage, ensuring that all citizens have access to medical services through a mix of national and employer-sponsored insurance. In this system, the medical expenses incurred are standardized nationwide through a common medical fee schedule and drug price regulations.
Table 4 Utility values [33] and costs of COVID-19 health states, from the MDV database and published source [36]2.3 Model OutputsOutputs of the analysis included rates of hospitalization, survival, readmission, and long-term sequelae, as well as costs (total, and by resource type/health state), and total QALYs by health state.
Costs were expressed in 2022 Japanese yen (¥; JPY), from the perspective of payers (the base case) or society (in a scenario analysis). We replaced all medical cost inputs derived from the MDV database with those calculated by uniformly applying the unit price of the 2022 NHI tariff instead of those from the years of claims used previously. Costs and QALYs were discounted at 2% per year, as per Japanese cost-effectiveness evaluation guidelines [38].
Cost effectiveness was then subsequently determined by the incremental cost-effectiveness ratio (ICER) of molnupiravir against best supportive care, compared with specific WTP thresholds (e.g. ¥5,000,000 per QALY gained).
The sensitivity analysis in this study was conducted using both deterministic sensitivity analysis (DSA) and probabilistic sensitivity analysis (PSA).
The DSA involved varying parameters within their 95% confidence intervals. In cases where variance information was unavailable, a standard error of 10% of the mean was assumed for literature-based parameters, as indicated in electronic supplementary material (ESM) Table 2 [39].
For the PSA, pre-defined distributions were used based on recommendations from Briggs et al. (2016) [39]. A beta distribution was employed for probabilities (Dirichlet for polytomous parameters) and health state utility values, while a gamma distribution was used for costs related to COVID-19 management. Continuous variables such as length of stay were modelled using a normal distribution, and for treatment effect parameters (relative risk), a log-normal distribution was utilized. The PSA involved sampling from the distribution of each model parameter in 1000 iterations. Additionally, the study represented the results of each probabilistic model run using a cost-effectiveness acceptability curve.
Further scenario analyses (excluding long-term sequelae and readmissions) using five-, 10-, and 15-year time horizons; using other estimates of molnupiravir treatment effect from other real-world studies; incorporating societal perspective through productivity loss; and exploring quality-of-life parameters from published literature [40,41,42,43] other than de novo vignette-based utility studies (see ESM Table 3) were also conducted to explore the impact of structural model changes on the ICER for molnupiravir.
Incorporating a societal perspective through productivity loss scenario analysis assumed that patients with COVID-19 were not working for the duration of any hospital stay. Productivity loss was calculated through multiplying the average daily wage [44] by length of hospital stay. The employment rate was assumed to be 69% for males and 52% for females [45].
Comments (0)