
Remember me



An in vitro, observational, descriptive, and comparative study was designed, which was approved by the Ethics Committee of the Hospital Clínico San Carlos with internal code 21/375E.
Primary maxillary first molars (1 M) and second molars (2 M) were collected from donated teeth with the approval and signing of the informed consent of the parents of the child patients. This donation occurred both in public and private dental clinics. The indication for tooth extraction was due to clinical reasons such as orthodontic reasons or delayed eruption.
Eligibility criteria and sample sizeThe study unit was all root portions without resorption and a complete apex, including the mesio-buccal (MB), disto-buccal (DB), and palatal roots. All teeth had Type I root canal anatomy according to the classification described by Vertucci et al. (Vertucci 1978). The minimum root length was 4 mm. Roots presenting any signs of external or internal pathological or physiological resorption that affected the apical foramen or pulp treatment were excluded.
The sample size was calculated using the G*Power® statistical programme. The diameters of the cervical third of each canal were taken as the reference point: M: 1.18 ± 0.6; D: 1.17 ± 0.25 and P: 2.56 ± 0.37 (Gaurav et al. 2013). Additionally, a power of 80% and a significance level of p < 0.05 were established, estimating that a sample size of at least 12 canals is required for each group. The study included six groups in total, which were classified according to the type of primary molar—first or second, and the canal type: mesio-buccal (MB), disto-buccal (DB), or palatal (P).
Storage samples and formation GroupAll treating dentists extracted and initially stored the teeth in isotonic saline solution (0.9% NaCl), which was provided in advance to ensure consistent storage conditions. Subsequently, the researcher collected them weekly and took them to the laboratory where they were debrided using Dentasept® Tri Enzymatic soap (DÜRR DENTAL, Bietigheim-Bissingen, Germany) a commercial enzymatic detergent containing protease, lipase and amylase, designed for the removal of organic residues. The teeth were then disinfected by immersion in 3% sodium hypochlorite for one week. The final storage was performed in sterile containers with sodium chloride 0.9% and kept at 4 ºC until use. The average storage period until analysis was 45 days.
The roots of the teeth were distributed into six groups:
Groups 1 and 2: mesio-buccal roots (MB) of the 1 M and 2 M, respectively.
Groups 3 and 4: disto-buccal roots (DB) of the 1 M and 2 M, respectively.
Groups 5 and 6: palatal roots (P) of the 1 M and 2 M, respectively.
CBCT image acquisition and 3D reconstructionThe roots were invested into addition silicone material blocks (polyvinyl siloxane, PVS) (V-Posil Putty Fast, VOCO®, Cuxhaven, Germany) for irradiation, with DICOM images with a slice thickness of 0.75 µm obtained using a CS 8100® tomograph (Carestream Dental, GA, USA) with a voltage of 90 kV, a tube current of 15 mA, exposure time of 7–15 s, voxel size of 75 µm, and a field of view (FOV) of 4 mm × 4 cm.
With the images and the 3D-Slicer® programme the 3D reconstruction of the root portions was performed (Fedorov et al. 2012). The "Threshold" tool allowed the calculation of the Hounsfield Units (HU) of the different structures. A range of −1000 to 250 HU was established for the root canals and 1294.4 ± 183.58 HU for the root portions.
Calculation of the taper of root canalsThe root canal length was measured from the apical constriction to its most superior sector with the 3D-Slicer® programme using the "Line" Tool. The mean lengths helped standardise the number of transverse measurements (diameters) for each canal root (MB, DB or P). Each canal was then proportionally divided based on its relative length compared to the mean length of canals in the same group (MB, DB, or P), using the following formula to obtain the distance between sections (DBS).
$$DBS=\frac }\left(\text,\text\right)}$$
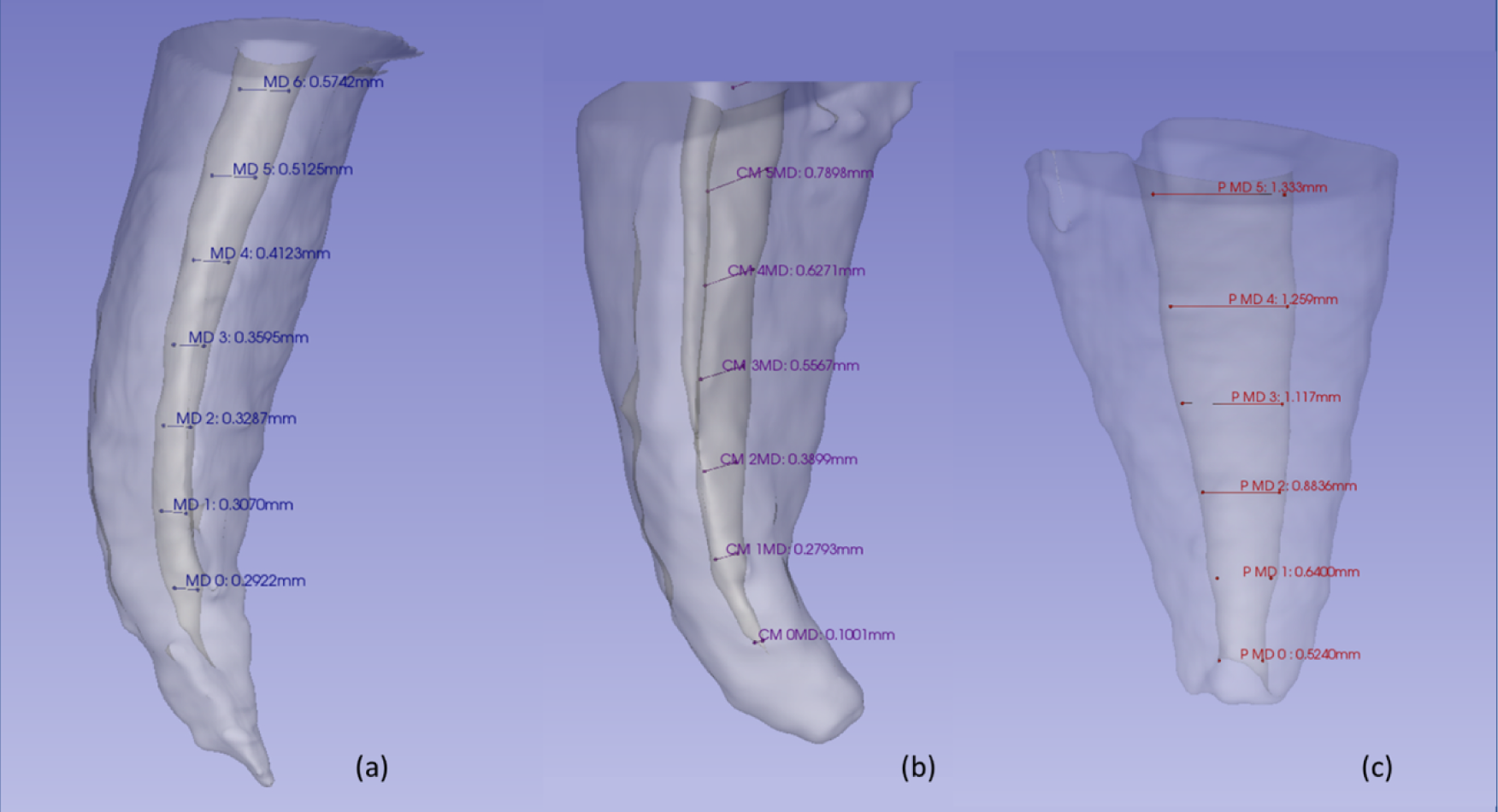
Next, all the diameters along the canal in the bucco-palatal (BP) and mesiodistal (MD) directions were calculated, as shown in Fig. 1.
Fig. 1
Representation of taking measurements in all three-dimensional reconstructions. a Mesio-buccal root; b Disto-buccal Root); c Palatal root
The bucco-palatal (BP) diameter refers to the horizontal measurement across the root canal, extending from the buccal to the palatal wall of the root canal, whereas the mesiodistal (MD) diameter corresponds to the measurement from the mesial (proximal to the midline of the dental arch) to the distal (away from the midline) wall of the root canal.
The apical constriction was considered the initial measurement (D0) (Kayabasi and Oznurhan 2020). Subsequently and equidistantly, the remaining measurements were obtained according to the result obtained by the DBS of each root canal.
The taper expressed in percentage (%) was calculated for each segment, according to the following formula (Torres-Ramos et al. 2020):
DL and Ds were the longest and shortest diameters recorded, respectively. Furthermore, the d value corresponded to the distance between both diameters.
Canals and files comparisonThe MD and BP diameters were measured from D0 with an interval of 1 mm up to the cervical third regardless of the total length of the canal. These measurements were compared with the diameters of the files of the Endogal®, Protaper universal®, Mtwo® and Protaper Next® systems. (Table 1).
Table 1 Diameter per millimetre of each instrumentCalibration, internal validityOne researcher was instructed in using the 3D-Slicer program (Fedorov et al. 2012) by a faculty professor, unrelated to the research, who specialises in radiology, with extensive practical knowledge in medical imaging and 3D analysis and experienced in the use of the 3D-Slicer software. A pilot test was carried out to train the principal investigator and verify the reliability and reproducibility of the study. The intraclass correlation coefficient statistical test evaluated the intra-observer agreement obtained a result of 0.95 (95% CI 0.91–0.97), which is considered is excellent according to the interpretation by Koo (Koo and Li. 2016).
Statistical analysisThe statistical analysis was carried out using IBM® SPSS® Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA). The qualitative variables were described by means and standard deviation (SD). After checking the normality (Shapiro–Wilk BP: p = 0.276 and MD: p = 0.249) and homoscedasticity (Levene BP: p = 0.209 and MD: p = 0.087) of the sample, the MANOVA test was applied to assess the increase in conicity along the root canals. In addition, the Huynh–Feldt test was applied to corroborate the sphericity criteria (W Mauchly p < 0.05), whilst the comparison between different roots was analysed using the Bonferroni test. The interclass correlation coefficient test was used to assess the compatibility of the different rotary systems with root canals, and the ANOVA test was used to determine statistical significance.
A bilateral hypothesis was established, with a power of 80% and a statistical significance level of p < 0.05.
Comments (0)