
Remember me



The randomized clinical trial (parallel groups) was conducted in the Outpatient Diagnostic Clinic, Department of Paediatric Dentistry and Dental Public Health, Faculty of Dentistry, Cairo University, from September 2022 to May 2023. Ethical approval was obtained from the Research Ethics Committee of the Faculty of Dentistry, Cairo University (approval date 28/06/2022). The trial protocol was prospectively registered at ClinicalTrials.gov (Identifier: NCT05313399).
Sample size calculationSample size determination was conducted through a power analysis targeting differences in AOB correction between the FPC and BS groups. Based on a previous trial by (Leite et al. 2016), the analysis incorporated an alpha level of 0.05, 80% statistical power, and an effect size of 1.23 (Cohen’s d), derived from changes in overbite correction. The smallest required sample size was calculated to be 24 participants. An additional 25% was added to account for potential dropouts, resulting in a final sample of 30 children, with 15 assigned randomly to each group. Sample size estimation was performed using G*Power (version 3.1.9.7) (Faul et al. 2007).
Inclusion criteriaChildren aged 6–11 years with an anterior open bite ≥ 1 mm associated with NNSHs, and adaptive tongue thrust were included. Participants were required to have fully erupted permanent upper and lower central incisors and a clinically confirmed Angle Class I molar relationship.
Exclusion criteriaChildren were excluded if they had craniofacial anomalies (e.g., cleft lip and/or palate, craniosynostosis, or syndromic conditions affecting craniofacial growth), any developmental or systemic disorders, a history of orthodontic treatment, or prior extraction of permanent teeth due to trauma or caries lesions.
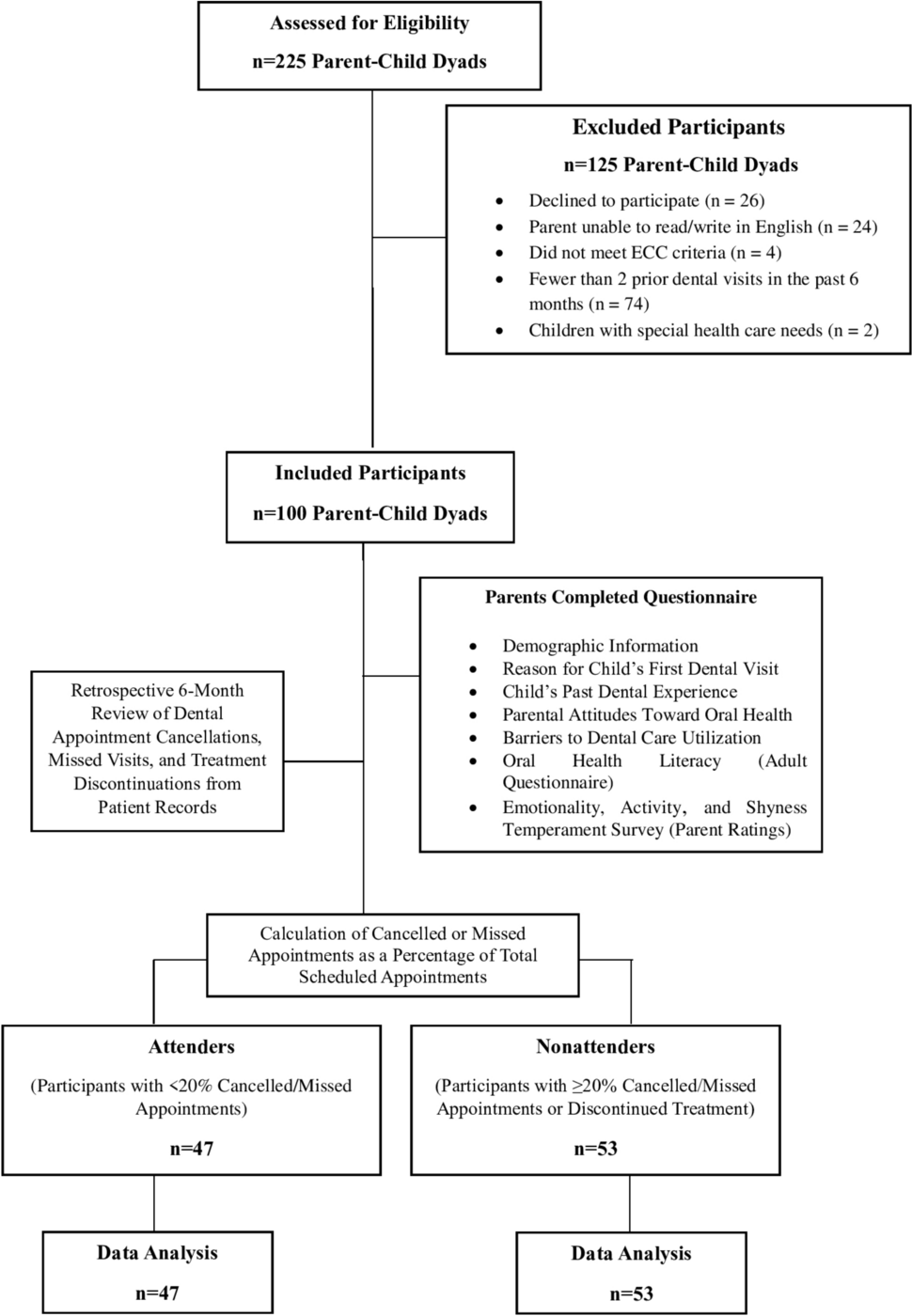
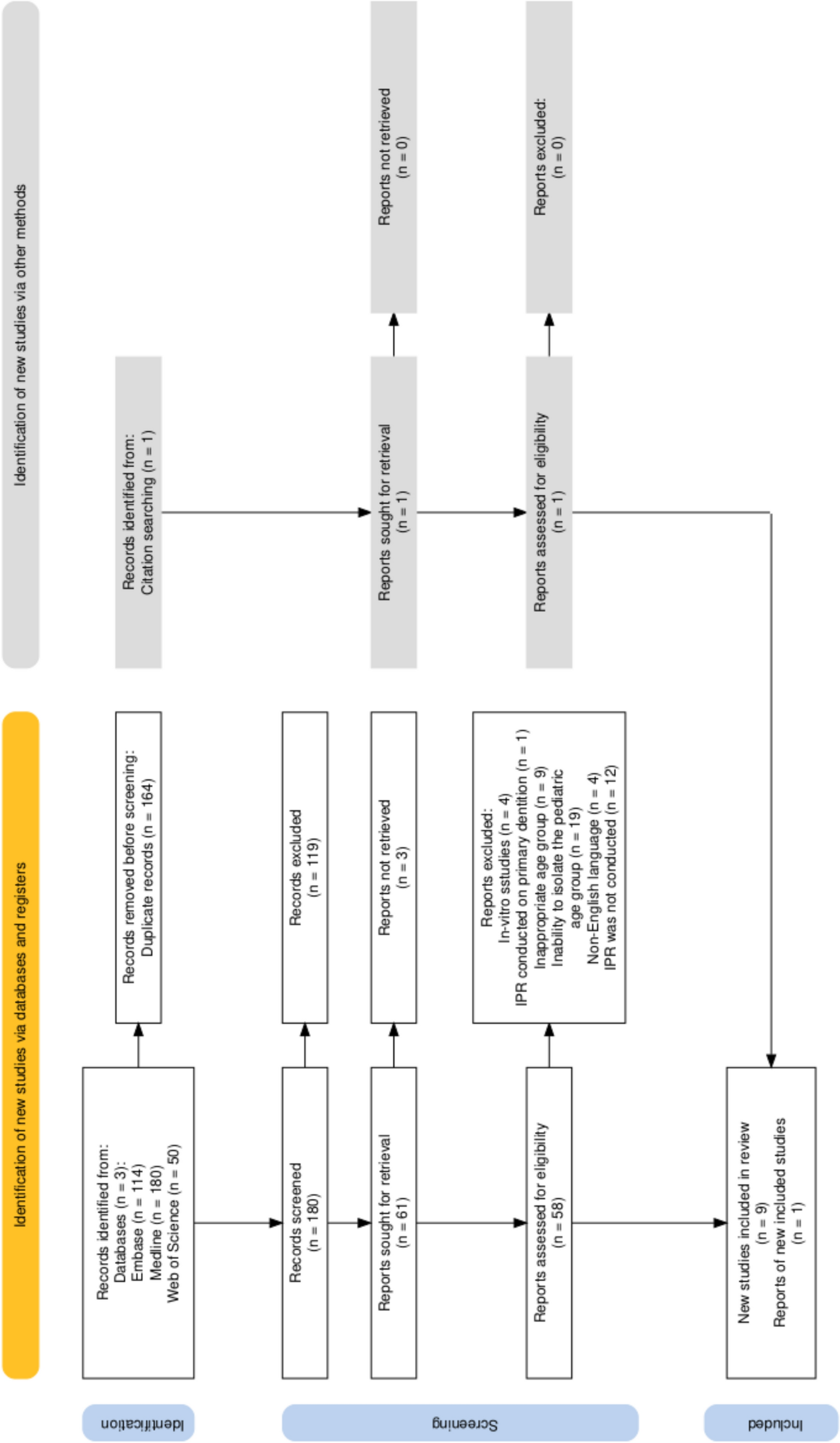
Subject recruitmentRecruitment was conducted between September 2022 and May 2023. A total of 50 participants were initially screened for eligibility, 20 did not meet the predefined inclusion criteria and were therefore excluded. The remaining 30 eligible participants were allocated randomly into two groups: the FPC group and the BS group, with 15 children in each. The randomization sequence was generated by M.M.A using www.random.org, and sealed opaque envelopes were prepared for allocation concealment, and R.H conducted group assignments, recorded participant details, and managed follow-up coordination. The randomization protocol and study design were developed and approved by A.H, who ensured proper methodological planning and compliance. Follow-up was completed by May 2024 following the scheduled course of treatment. Participant flow is illustrated in the CONSORT flow chart (Fig. 1). All 30 participants completed the 1-year follow-up, with no dropouts.
Fig. 1 Clinical examination
Clinical examinationBefore treatment, participants underwent comprehensive documentation, including intraoral and extraoral photographs, panoramic radiographs, digital lateral cephalometric radiographs, and digital bio-models were generated by scanning stone dental casts using the Medit i500 scanner (Medit Corp., Seoul, South Korea) to produce stereolithographic (STL) files for model analysis. The clinical examination evaluated AOB, molar relationship, tongue thrust, and oral habits. A preparatory behavioral phase provided each child with oral hygiene instruction and caries control measures.
BlindingOutcome assessors were blinded to group assignments; however, blinding was not feasible for the operator or patients due to the visible nature of the appliances.
InterventionsBonded spurs (Tongue Tamers®, Ortho Technology, Tampa FL) were placed on the palatal surfaces of the maxillary incisors and the lingual surfaces of the mandibular incisors, at the cervical and incisal thirds of the teeth, respectively, to reduce potential occlusal interference. Attachment of the spurs was achieved using Transbond™ XT (3M Unitek, St. Paul, MN, USA), a light-cured orthodontic adhesive after acid etching to ensure optimal retention (Justus 2001; Leite et al. 2016; Aliaga-Del Castillo et al. 2021a, b).
The FPC was fabricated by adapting orthodontic bands (Ormco Corporation, Glendora, CA, USA) with a 0.9 mm wire loop soldered to extend between the maxillary canines. Orthodontic separators were used prior to cementation to ensure a proper fit. The appliance was cemented with glass ionomer cement (Medicem glass ionomer, Promedica Dental Material GmbH, Germany) was used for secure attachment (Leite et al. 2016). Participants who did not show adequate AOB improvement or required additional treatment were referred for comprehensive orthodontic therapy.
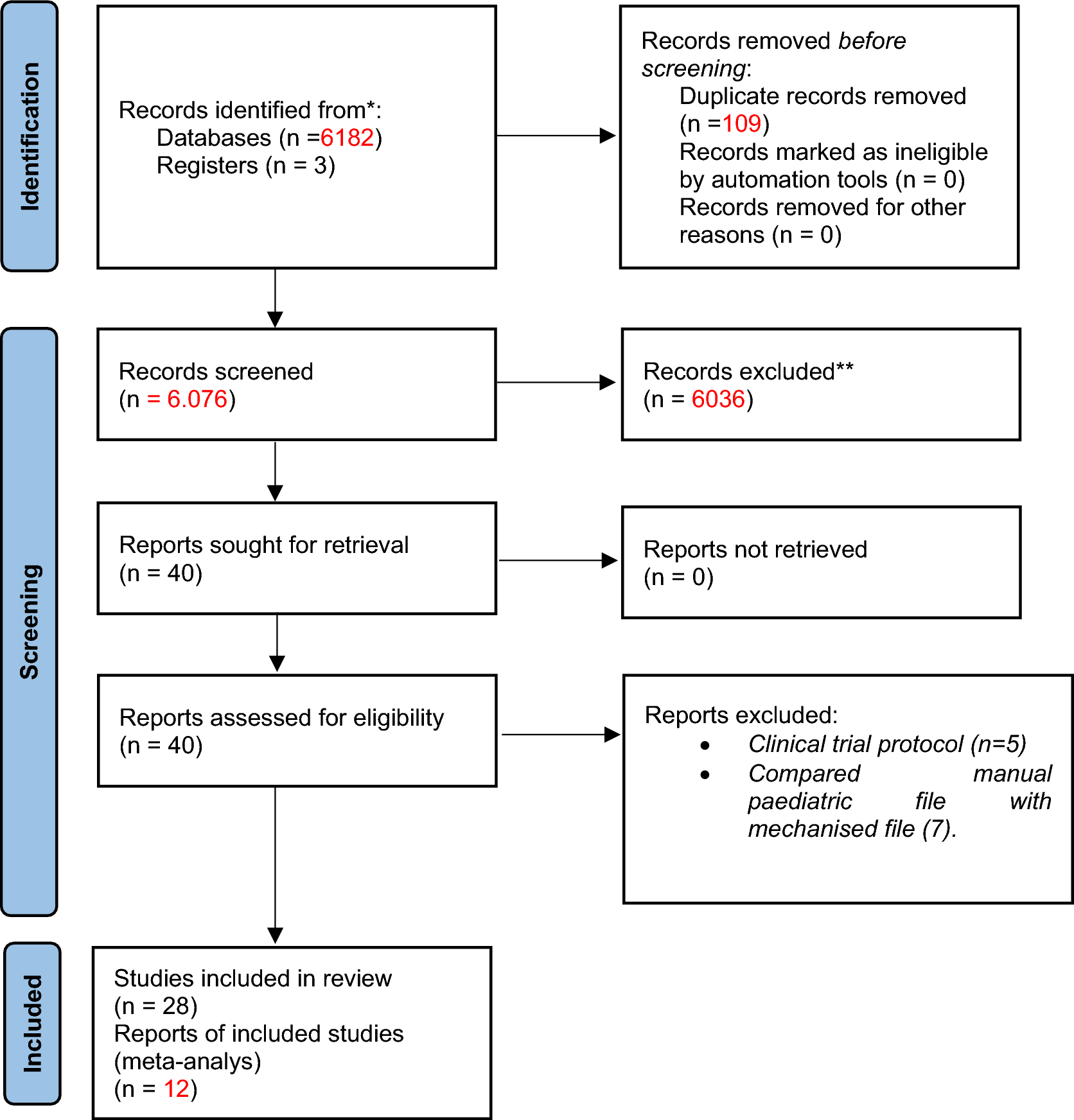
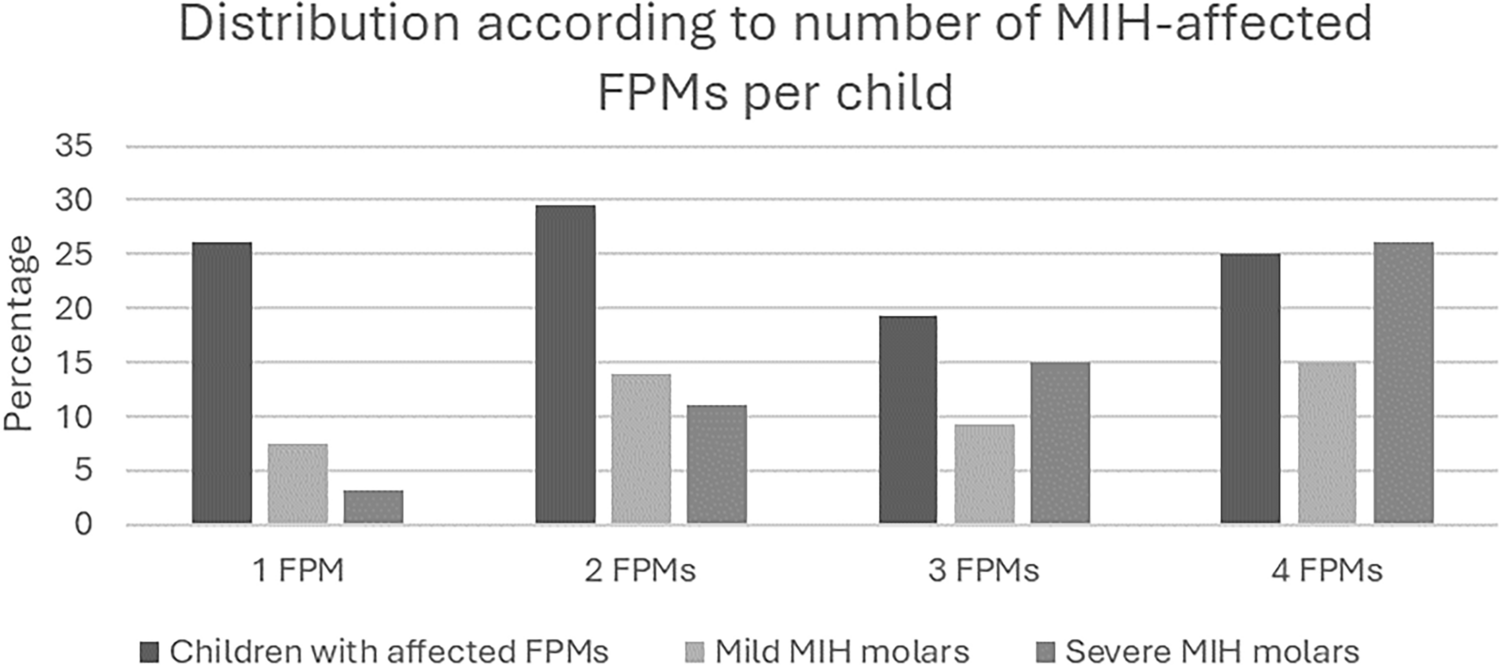
Outcome measuresThe primary outcome was overbite correction, measured in millimeters from digital bio-models. A secondary outcome included achievement of a positive overbite (incisal overlap) as a clinical success indicator (Slaviero et al. 2017; Aliaga-Del Castillo et al. 2021a, b) Other outcomes included changes in arch dimensions and vertical skeletal relationships. Digital bio-models and vertical skeletal changes were assessed through lateral cephalograms. Digital bio-models were analyzed with OrthoAnalyzer 3D software (3Shape, Copenhagen, Denmark) for overbite, arch length, arch perimeter, vertical dental development, and intermolar distance (Fig. 2). Lateral cephalometric analysis was performed with Dolphin Imaging Software Version 11.5 (Dolphin® Imaging and Management Solutions, Patterson Dental Supply, Inc., Chatsworth, CA) to assess skeletal and dentoalveolar changes. The maxillo-mandibular plane angle (MMPA) and other angular and linear variables were measured (Fig. 3). The detailed description of all measured variables is provided in (Table 1). All measurements were made by R.H. and independently verified by A.H., both of whom were trained and calibrated in the software.
Fig. 2
Digital model illustrations showing the measured dental variables A Overbite. B Overjet. C Antero-posterior position of the upper first molar. D Molar relationship. E Vertical dental development. F Maxillary and mandibular arch length. G Maxillary and mandibular arch perimeter. H Intermolar width
Fig. 3
Lateral cephalometric tracing illustrating anatomical landmarks and skeletal and dentoalveolar angular measurements used in orthodontic analysis. The key cephalometric points include: S Sella, N Nasion, A A point, B B point, Pog Pogonion, Gn Gnathion, Me Menton, Go Gonion, ANS anterior nasal spine, PNS posterior nasal spine, Or orbitale, Po porion and LAFH lower anterior facial height and numbered angular variables include 1. SNA Sella–Nasion–A point angle, 2. SNB Sella–Nasion–B point angle, 3. ANB A point–Nasion–B point angle, 4. MMPA maxillary–mandibular plane angle, 5. Y-axis, 6. Mx1.PP maxillary central incisor to palatal plane angle, 7. IMPA mandibular central incisor to mandibular plane angle and 8. 1.1 interincisal angle
Table 1 Linear measurements on digital bio-modelsData processing and analysisStatistical analyses were performed using SPSS® (version 20, IBM Corp., Armonk, NY, USA). Data normality was evaluated using both the Kolmogorov–Smirnov and Shapiro–Wilk tests, confirming that all variables followed a normal distribution in both groups, as confirmed by non-significant p values (p > 0.05) supporting the use of parametric analysis. Equality of variances was assessed using Levene’s test, which indicated homogeneity across all comparisons. Given that the assumptions of normality and homogeneity of variances were met, parametric tests were appropriately employed. Paired t tests were used for within-group comparisons and independent t tests for between-group comparisons (significance set at p < 0.05). Categorical outcomes (e.g., treatment success defined as positive overbite) were compared using the chi-square test. Relative risk (RR) with 95% confidence intervals was calculated. Intra- and inter-observer reliability were assessed by re-evaluating 10% of the measurements 1 month after initial analysis; intraclass correlation coefficients (ICCs) were 0.93 (intra-observer) and 0.91 (inter-observer), indicating excellent agreement. No changes were made to the trial outcomes after commencement.
Comments (0)