
Remember me
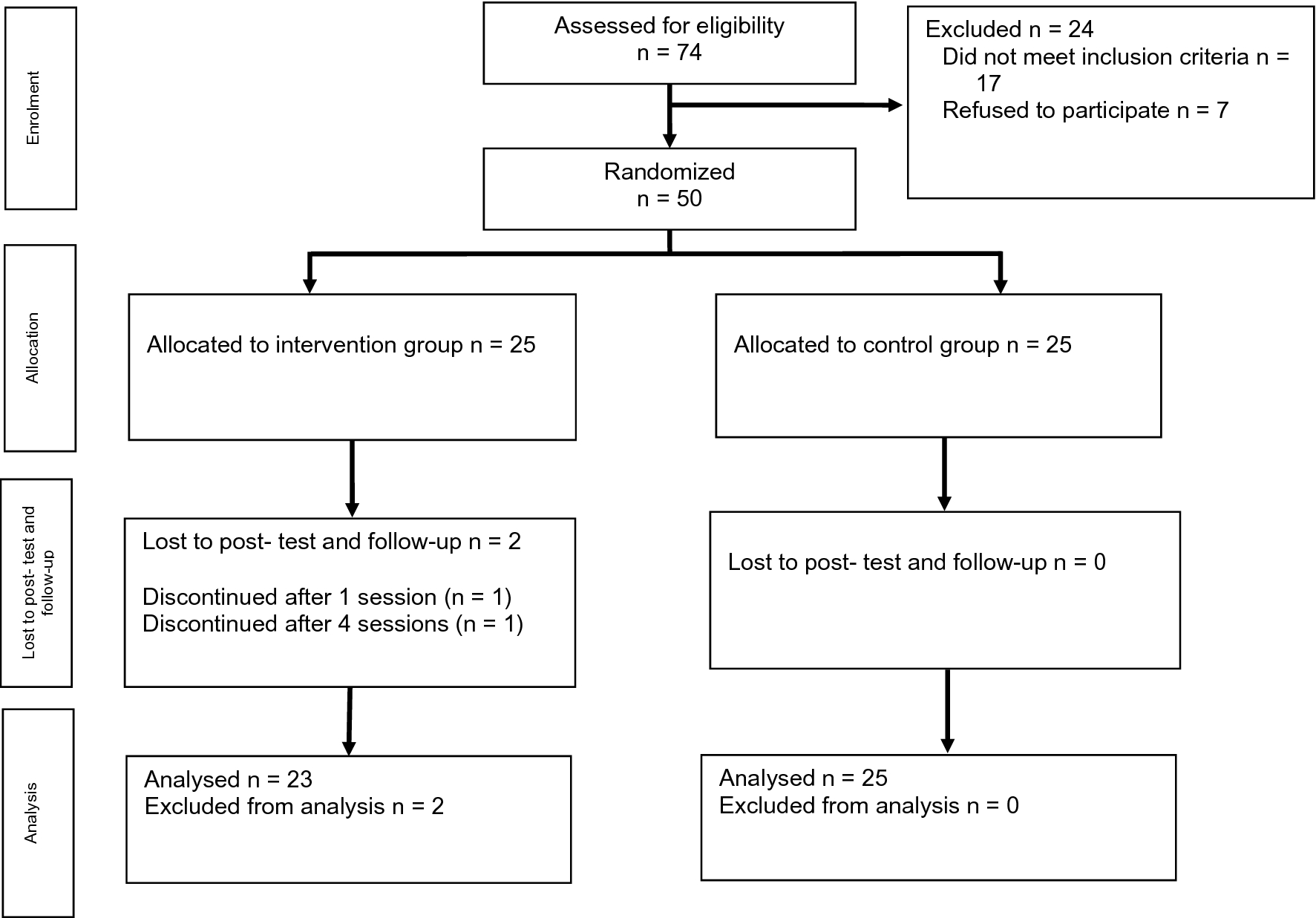


The presented case-study is a woman in her mid-forties with a reduced threshold of endurable load since her first SARS-CoV-2 infection, about a year before beginning psychotherapy. She was diagnosed with post COVID-19 condition, unspecified (U09.9), adjustment disorder with anxiety (F43.22), and other specified mental disorders due to known physiological conditions (F06.8), based on ICD-10. She attended 24 primarily weekly sessions of individual Cognitive Behavioral Therapy. The patient had been employed full-time in an administrative role until her SARS-CoV-2 infection. One year later, at the start of therapy, she was undergoing vocational reintegration, working 1–2 h daily. She reported cognitive deficits in concentration and memory alongside a mood marked by worry, despair, and sadness. She expressed feelings of helplessness and fear of losing autonomy, worthlessness, self-doubt, and excessive rumination, as well as exhaustion ranging from weakness to complete depletion. Physically, she described headaches, a burning, itching sensation on her scalp, an increased need for rest and sleep, rapid sensory overload, and noise intolerance.
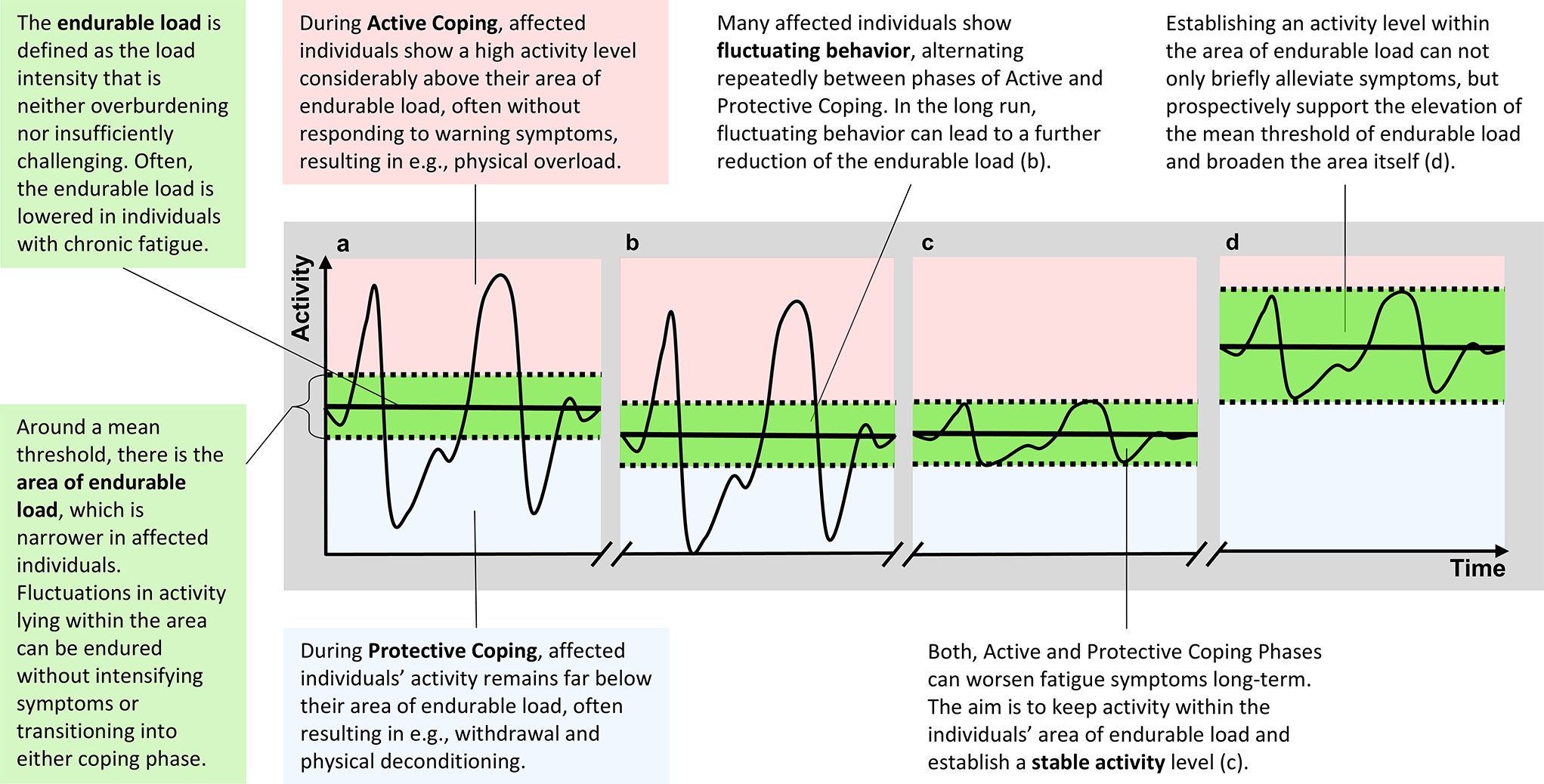
Clarification of ObjectivesAt the beginning of treatment, therapeutic objectives should be clarified early on to prevent false expectations. It should be communicated that the first aim is to achieve stable activity levels and prevent symptoms from further deteriorating (see also Gaber, 2021) by staying within the area of endurable load. The chance to gradually increase the threshold of endurable load, however, may arise in the long term.
Introduction of the APC-Model as Common Therapeutic FrameworkAfter clarifying the objectives, the Model of Active and Protective Coping for Chronic Fatigue (APC-Model) can be introduced as a common therapeutic framework to keep track of both dysfunctional and functional behavior and phasic shifts. An important goal of psychoeducation is to convey a clear understanding that activity levels significantly higher and lower than the endurable load may risk worsening symptoms. Therefore, activities should require load within the area of endurable load. As one goal of treatment, this concept focuses on the management of behavior instead of symptoms in order to strengthen a person’s perceived self-efficacy and sense of control.
Conceptualizing Behavioral Patterns: Applying Behavioral AnalysisGiven the interindividual heterogeneity of symptoms, we argue that it is essential to identify individual factors that contribute to the dysfunctional behavioral patterns. In the following, we focus on a deeper understanding of specific behavioral patterns within Active and Protective Coping and on analyzing them to derive targeted therapeutic implications.
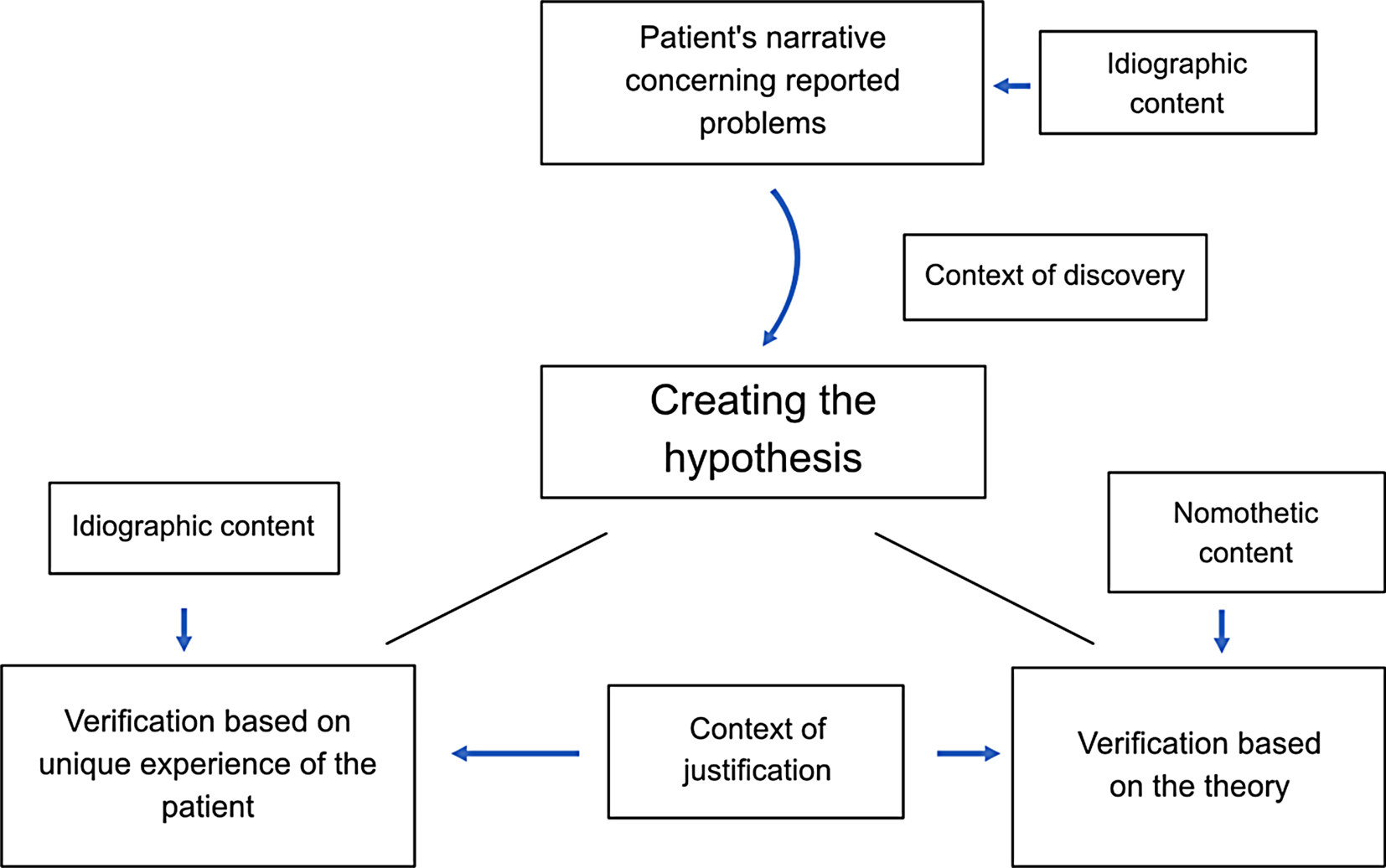
As an established framework for behavioral analysis, the SORCK model developed by Kanfer et al. (2012) is a supportive tool to explain and derive therapeutic interventions for problematic behaviors linked to complex syndromes. It explains behavioral (problematic) responses (R) in specific situations (S) along with their consequences (C) and contingency (K), while, within the organism variable (O), considering relatively stable bio-psycho-social factors that influence an individual’s spectrum of behavioral patterns. Since we identified Active and Protective Coping as the two major behavioral patterns between which chronic fatigue patients characteristically shift repeatedly (see Fig. 1), it is central to our model to work with two distinct conceptualizations —one for each coping pattern. By adapting SORCK principles, the therapeutic process now focuses on understanding the dynamics of emotion, cognition, and behavior for both phases, aiming to identify individual factors that drive and maintain patients in the Active and, respectively, Protective Coping phase (as depicted in Fig. 2). This said, these analyses can also lead to revealing situations with functional behavior, which then should be reinforced. Ultimately, these insights guide deriving and implementing interventions that provide the patient with adaptive strategies to keep activities within the endurable load.
Fig. 2
Application of an adapted version of the SORCK-model to active and protective coping
Conceptualization of Active CopingOrganism-Variable (OA)On the biological level, the patient reports neuropsychological deficits in memory and executive functions. Psychosocially, she has high performance standards, as measured by the Young Schema Questionnaire (YSQ; Young, 2005). Work is a significant source of her self-worth, and autonomy and control are crucial psychological needs (Grawe, 2004) to her, as indicated by the Questionnaire for the Analysis of Motivational Schemas (FAMOS; Holtforth & Grawe, 2000).
We argue that when vulnerable aspects of the organism variable (OA) are triggered or become the patients’ focus, they respond to daily life situations and challenges with dysfunctional behavioral patterns. Our patient’s aversive representation of low performance is amplified by the unmet need for autonomy and control as a consequence of her illness. To compensate, she responds with Active Coping behavior, which manifests in motor-behavioral, cognitive, emotional, and physiological levels as indicated by the response variable.
Response-Variable (RA)Active Coping is characterized by a burst of activity on a motor-behavioral level, such as working, sports, leisure, or caring for others. In our study case, this pattern is linked to cognitions like “Only if I perform and take responsibility, I can provide for myself safely” and “Relaxation is not possible for me and would lead to an immediate breakdown.” These cognitions are highly threatening to her due to their strong link with her aversive perception of low performance. She responds with fear of losing independence and feelings of worthlessness and with a diffuse sense of inner restlessness and heightened physiological arousal.
Consequences (CA)In the short-term, Active Coping allows the patient to momentarily show a heightened performance and fulfill her (work/social) roles and duties (positive reinforcement; C+). Her high activity level is negatively reinforced as it helps to temporarily avoid confronting her deficits and fear of losing autonomy and control (C-/). Shaped by her biography, this compensating behavior with the underlying motives was likely effective before post COVID. However, with reduced energy, maintaining high activity levels is associated with physical and psychological overload and a further performance decline (C-). As symptoms of overload, our case reported, for example, heightened sensitivity to noise, headaches, and prolonged sleep (> 11 h per night plus sleep around lunchtime).
Derived Points of Intervention and Treatment Strategies for Active CopingApplying the Model of Active and Protective Coping (APC-Model) and behavioral analysis resulted in two separate case conceptualizations, one for each coping phase. For Active Coping, we identified the following major points of intervention: (1) perceived neuropsychological deficits, (2) lowered self-worth, (3) high activity level leading to overexertion, (4) avoiding confrontation with deficits, and (5) perceived loss of autonomy and control. Once the points of intervention are derived from the conceptualizations, the therapist can use established treatment strategies for the respective points. In the following, we elaborate on possible therapeutic strategies by use of examples from our study case.
(1) Addressing perceived neuropsychological deficits: The reported deficits in memory and executive functions can be addressed with established neuropsychological training strategies while ensuring that the training remains within the area of endurable load. However, for our case mainly compensatory strategies with a focus on energy management were implemented. The patient’s priority was to establish a stable performance during reduced working hours. Time with more intense cognitive activity was therefore purposefully saved for work.
(2) Addressing reduced self-worth based on performance and external evaluation: The patient’s attention was directed towards sources of self-worth beyond work achievements or external judgment and towards realizing small steps in the process.
(3) Phases of overexertion: We hypothesize that during Active Coping, the individual’s attentional focus is external, lying on performance, financial consequences, and/or the evaluation of the social environment while ignoring internal symptoms, such as emotions, early signs of fatigue like bodily symptoms of overexertion. Awareness of these symptoms were improved through regular mindfulness exercises and a fatigue diary, considering emotional, physical, and cognitive aspects. To prevent overexertion and crashes, the therapeutic process included empowering the patient to set healthy boundaries, and teaching pacing strategies like incorporating regular and mindful breaks within her (work) day structure.
(4) Careful confrontation with deficits: The study case was gently confronted with her current deficits and the unforeseeable course of her illness, validating emerging emotions such as mourning the loss of her former self. This process was supported by elements from Acceptance and Commitment Therapy (ACT).
(5) Addressing perceived loss of autonomy und control: Through psychoeducation, we helped her understand the mechanisms behind her symptoms, thereby restoring a sense of control. This includes redefining autonomy and control considering her current capabilities. By applying an adapted fatigue diary (see Online Resource 2), and weekly assessing and categorizing her behavior into Active and Protective Coping phases, she was able to establish a link between activities and symptoms, enhancing her sense of control and self-efficacy.
Conceptualization of Protective CopingOrganism-Variable (OP)Protective Coping (OP) as a response may come particularly at play, when on a biological level the patients have experienced harmful consequences of overload. These include intense fatigue symptoms and muscle pain, often referred to as “crashes,” especially in the context of Post-Exertional Malaise (PEM). Relevant developmental experiences of our study case include severe impairment after an Epstein-Barr virus infection approximately 25 years earlier, causing significant career changes. During phases of Protective Coping, her tendency towards pessimism may be amplified, as indicated by the Young Schema Questionnaire (YSQ; Young, 2005). Other traits triggering Protective Coping include a high need for safety and control and low risk-taking tendencies. The attentional focus shifts to internal factors like bodily symptoms.
Response-Variable (RP)We again argue that when critical aspects of the organism variable (OP) are pronounced or activated, patients may respond to daily life situations and other challenges (see, e.g., Shifts SP) with Protective Coping strategies that reach dysfunctional levels. In our study case, Protective Coping occurred when being overly anxious about a relapse. Her behavior was characterized by avoidance of activities, e.g. avoiding noisy crowds or any work and social interactions. This behavior was accompanied by cognitions such as “I must avoid another relapse”, and “I may need my energy for something more relevant”, which are strongly associated with previously experienced crashes. On a physiological level, the individual exhibited signs of high physiological arousal, such as increased heart rate and muscle tension, reflecting a bodily response to perceived threats and stressors. The arising emotions included anxiety, a sense of threat to health, and a fear of losing control over her own body.
Consequences (CP)As a short-term consequence of the Protective Coping response pattern, individuals are able to recover physically from overload (negative reinforcement; C-/) and experience relaxation (positive reinforcement; C+). However, in the long term, a dysfunctional low level of activity is associated with physical deconditioning (C-). Additionally, by withdrawing from professional and social roles (e.g., beloved creative tasks, coffee breaks, family dinners), the patient lost significant sources of self-worth and endangered the fulfillment of her need for attachment (C+/).
Derived Points of Intervention and Treatment Strategies for Protective CopingWhile mainly showing a tendency towards Active Coping, our study case shifted into Protective Coping behaviors after viral infections. We identified the narrow focus on fear of symptom deterioration and the responded withdrawal as major points of intervention during Protective Coping.
Treatment strategies involved (1) validating the triggered fears of massively worsening symptoms and explaining them within the context of the previously mentioned developmental factors. At the same time, we (2) gently educated her about the relationship of monitoring body symptoms too closely and thereby reinforcing them (Bushnell et al., 2013). We also elaborated that withdrawing from rewarding activities more than necessary can cause her to remain below her potential for antidepressant behavior and risk further deconditioning of her body. We helped her (3) broaden her attentional scope from a narrow focus on fear of symptom deterioration to more external stimuli, such as other unmet basic needs, e.g., attachment. We identified her values and needs (i.e., based on Grawe’s concepts; Grawe, 2004) and (4) derived and planned activities to meet them within her potential and limitations.
Phasic Shifts (SA and SP)Since patients experience unexplained fluctuations in their behavior, we consider it essential to identify typical situations that precede a shift to Active or Protective Coping. We assume that these turning points can be triggered by internal or external factors. Internal factors may involve realizing the consequences of the preceding coping pattern. A shift to Protective Coping can be preceded by realizing that excessive Active Coping went along with intensified fatigue symptoms. External factors can include job-related pressure or financial concerns, triggering a shift from Protective to Active Coping. We recommend collecting typical factors and derive and practice specified functional strategies with the patient that he or she can apply instead of re-engaging in dysfunctional behavioral patterns.
Balancing Active and Protective Coping Behavior To Stabilize ActivityWhen contrasting and regulating Active and Protective Coping behaviors, certain needs or experiences may seem contradictory and difficult to reconcile, appearing to exclude one another like opposing poles. This reflects the inner conflict many individuals face being torn between which needs to prioritize, possibly explaining the observed “all-or-nothing” behavior. According to our model, during any phase of dysfunctional coping, the focus tends to be heavily on one pole of needs, while the other is neglected. For example, our patient focused on reducing activities to avoid health setbacks, thereby neglecting social needs or needs for pleasure (Grawe, 2004). The metaphors of a pendulum vs. a scale can be helpful here, representing the back-and-forth movement vs. balancing between perceived opposing needs. The therapeutic challenge, then, is enabling the patient to acknowledge and integrate both sides within their potential, increasing flexibility towards adaptive behavior. Based on our study case, we will illustrate the conflict between seemingly opposing needs and the therapeutic approach to help her find a balanced solution. For another example, see Online Resource 3.
Our patient has been applying pacing strategies to manage her fatigue symptoms for the past couple of months. She had reduced the pleasurable activities that formerly had been part of her daily routine. She paid attention to receiving enough sleep and breaks, not extending her planned working hours. This led to a change in work content. She eliminated the more exciting and creative tasks and concentrated on administrative tasks that were rather boring but necessary for the job. After several weeks, she reported feeling better and a slight increase in energy levels, also reflected by slowly increasing her working hours. Now she received the opportunity to engage in an additional creative project, which had to take place during the night. However, she faced an internal conflict: wanting to reward herself with more exciting tasks at work (need for pleasure) but fearing overexertion and another setback (need for control over health). She is deeply caught in this conflict and feels pressured to make an all-or-nothing decision as if she must choose one side over the other. The described inner conflict arises from two opposing motives:
Active Coping: “I deserve to treat myself this week. I want to finally enjoy work again.” This reflects her need for pleasure, which she feels entitled to fulfill, especially after sacrificing it for so long.
Protective Coping: “I need to hold back—it would be better for my health [and ability to work] to withdraw. I can’t afford another crash.” This reflects her need for control over her health and needs for self-esteem protection and independence through performance at work.
Guided during the therapeutic process, she was able to reflect on overwhelming aspects of the creative task, including staying up late and being filled with excitement. She anticipated a crash that she only could counteract by extended rest. These insights allowed her to consider restructuring and reducing her working hours for the week to be able to get the rest needed to compensate for this extra task at night – a solution that she earlier would not have considered. In the next session, she reported that she had felt more fatigued for two days, but that she was able to manage the significantly reduced timetable without ending in a crash. She highlighted the joyful moment of creativity and mentioned that her mood had profited significantly from this endeavor. This observation indicates that her balanced approach considering differential needs had a positive impact on her emotional well-being without sacrificing physical health.
Comments (0)