
Remember me
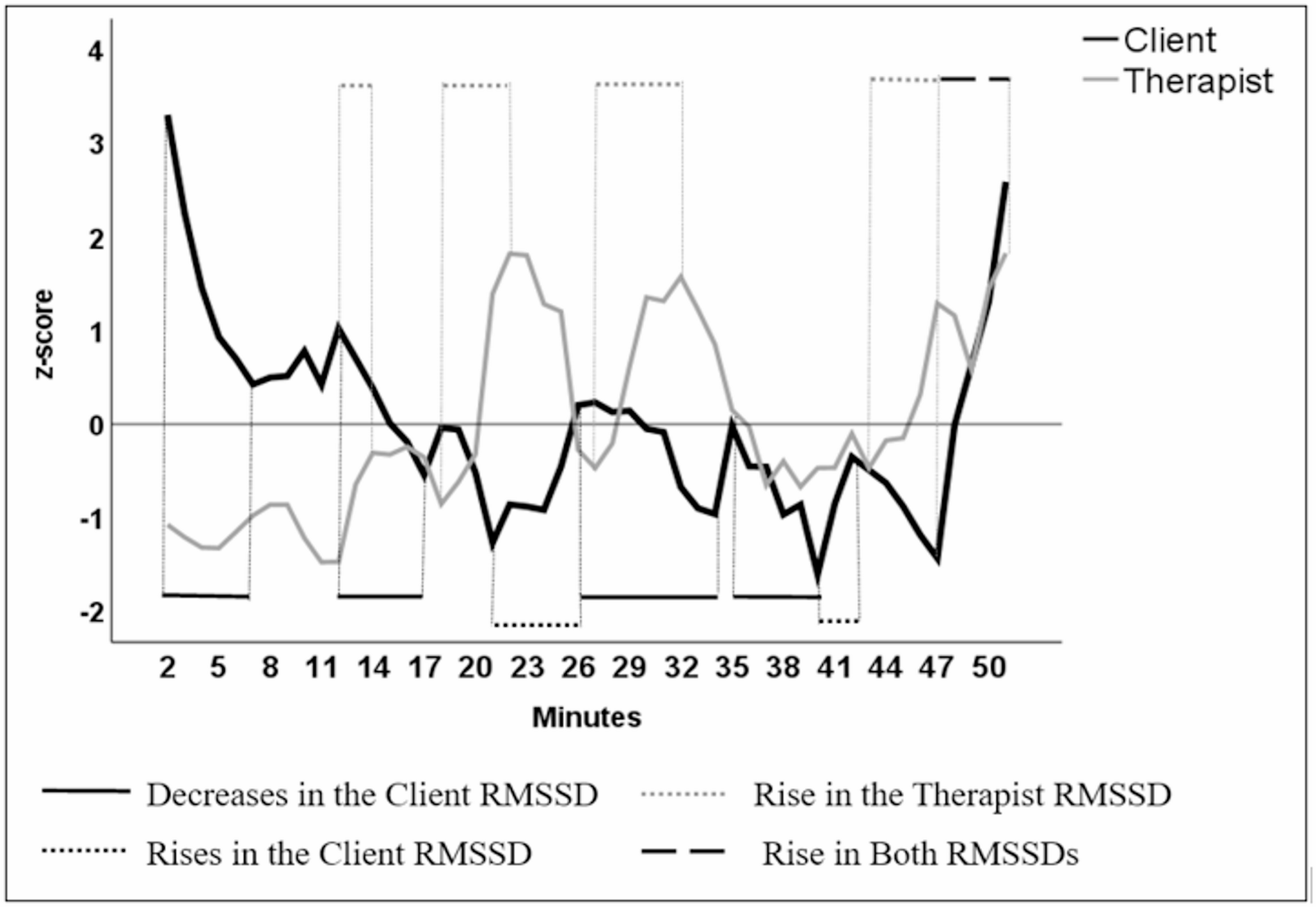


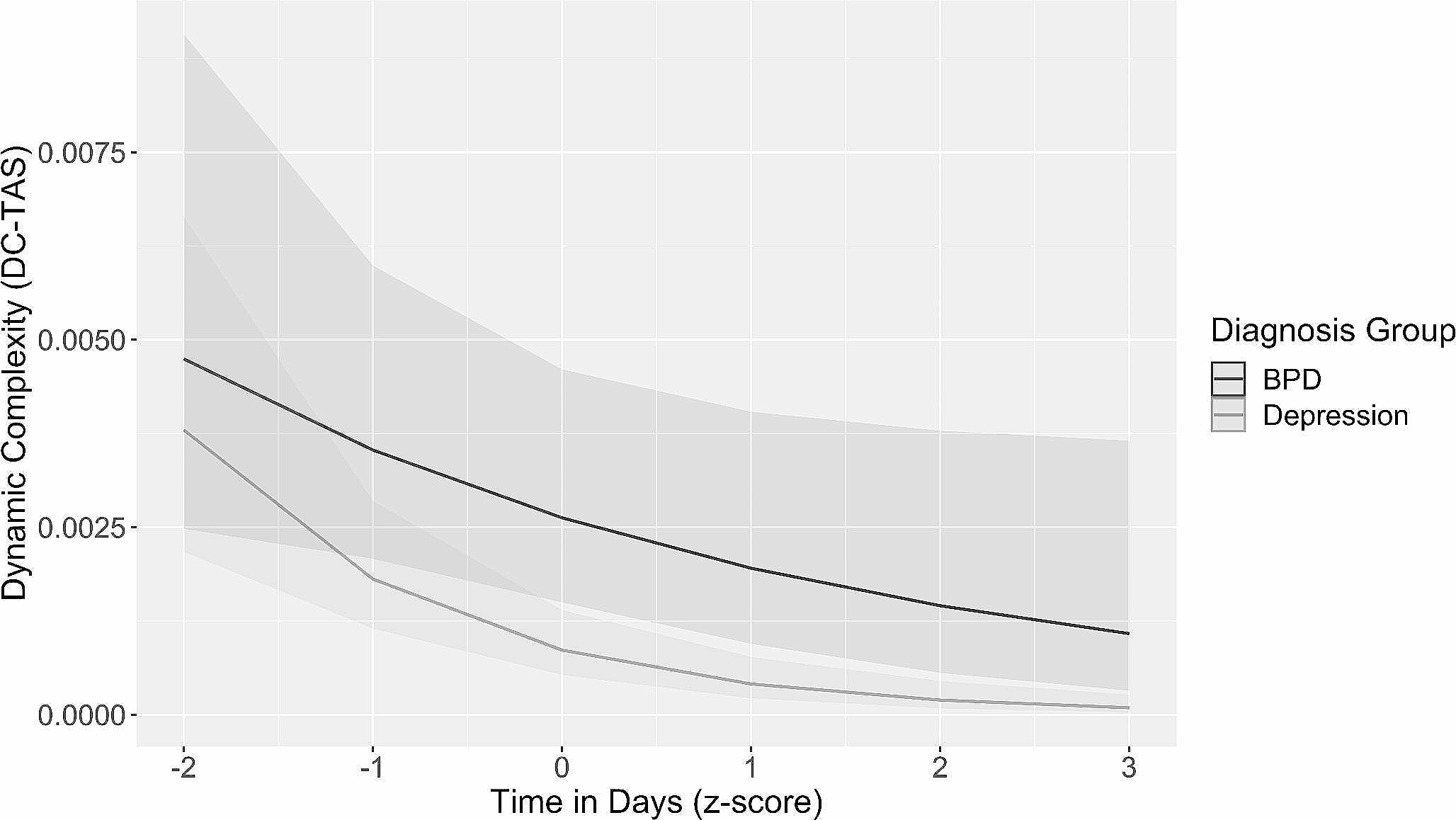
Fig. 1 demonstrates both the client and the therapist RMSSDs over the session. Decreases and rises in the client RMSSD are indicated below and the rise in the therapist RMSSD above the profiles. As decreases and rises in the client and the therapist RMSSDs partly overlap, the descriptions of the dialogue do not form a chronological narrative.
Fig. 1
The client and the therapist RMSSDs over the session
Decreases in the Client RMSSDThere were four time slots with a clear decrease in the client RMSSD lasting more than 2 min, first occurring right at the beginning of the session (2–6 min) and the second soon following it (12–17 min). The third decrease occurred in the second half of the session (26–34 min) and was soon followed by the fourth decrease (35–40 min).
The First Decrease in the Client RMSSD (2–6 min)At the beginning of the session, the client shared her unpleasant physical experiences (“somebody was drawing my head down” and “feeling of vomiting”) when expecting to meet and finally met her close relatives. She talked about her thoughts concerning these family relationships and the controversial feelings and emotions they evoked (e.g., guilt and bad conscience).
The Second Decrease in the Client RMSSD (12–17 min)The client described her will to distance herself from her relatives and her will to stay away from their discussions to protect herself. She told about seeing her future as “empty,” as she had “dropped off.” She described how she felt that the past and the future were slipping away, as if she would be far away from a “distant river of life” and not be part of what was going on around her.
Toward the end of this time slot, the therapist RMSSD started to rise. At 16 min, the therapist noticed that the client was tearful and offered her handkerchiefs. Although the therapist did not say it aloud in the session, at this moment, she remembered the client’s earlier wishes to die. She thus interpreted the client’s present talk in the “wish to die” framework and noted “how sad the thoughts are” and how understandable it was that the client wanted to avoid these thoughts and emotions raised by the visit of the relatives. At 17 min, the therapist directed both the client’s and her own attention to the client’s bodily postures and expressions and expressed her observation that the client was holding her breath. The therapist guided the client to breathe in and sigh, which the client did, but according to the client, it did not feel emotionally helpful.
The Third Decrease in the Client RMSSD (26–34 min)The client talked about her controversial close relationships, about not being able to change herself, and about her anger and grumpiness. At 27 min, the therapist asked how the client felt about the happy feelings expressed by other family members in relation to the family event she was talking about, and the client described her will not to take part in those feelings. The therapist validated this and proposed an interpretation that it was the client’s way to protect herself (and the therapist RMSSD was raised), but she also noted how this led to the client being and feeling an outsider to everything. The client further described her future as an outsider and how she cannot and will not change, although everything else changes.
At 30 min, the therapist said that she also became angry when thinking of how the recent family event had affected the client. At that point, a steeper decrease in the client RMSSD occurred. She sighed, and the therapist encouraged her to fortify the sigh and expressed how the client was probably experiencing a complex array of emotions, including sadness, desperation, and anger. The client agreed but called her feelings grumpiness rather than anger, which she saw as too strong a word. They also wondered whether it was more like disappointment, accusation, and guilt. At 32 min, the therapist asked the client about her possibility of finding secure or soothing images, which the client said was not possible now, except by avoiding situations and people. The client described her ways of regulating her anxiety, which occurred simultaneously with a short rise in her RMSSD.
The Fourth Decrease in the Client RMSSD (35–40 min)The therapist suggested that the client was allowed to express her feelings and questioned whether her negative emotions were unacceptable. The client replied that her feelings, which she felt both unacceptable and too strong, caused her guilt and described how she sees herself as a “weak, wrong, bad, evil, jealous person.” (During this talk, the therapist RMSSD decreased.) The therapist said that it is understandable that the client cannot hold in her mind an image of herself as a bad person and simultaneously feel allowed to negative emotions. She also said that the client’s inner voice accusing her of her thoughts sounded very condemning, as the client’s emotions were extremely human. The client disagreed, saying that her emotions were too extreme and strong. The therapist validated and normalized the client’s emotions in light of the client’s life history, after which the client RMSSD increased.
Comments on the Decreases in the Client RMSSDThe common nominators of these periods of RMSSD decrease are threefold. First, they occurred as she described either her unpleasant physical experiences or her feelings and emotions, which she did not accept in herself. Second, moments of sadness could be recognized as the decreases occurred when the dialog concerned the client’s wishes to die and feelings of being an outsider. The third theme during these time slots was the client’s difficulties in receiving and accepting empathy or validation offered by the therapist or as it did not feel emotionally helpful.
Rises in the Client RMSSDThere were two time slots with a clear rise in the client RMSSD, the first occurring at 21–26 min and the second occurring at 40–43 min. There was also a third one, but as it occurred simultaneously with a rise in the therapist RMSSD, it will be described later.
The First Rise in the Client RMSSD (21–26 min)Around 21 min later, the conversation turned to the client’s fears and desperation. The therapist described her understanding of these feelings using the client’s metaphor of “the distant river” and encouraged the client to think about whether there was any way for her to approach the river. The client pondered whether it was a question of will or a lack of means to do it. The therapist asked whether the opposite of the will was fear. The client further wondered to what extent it was fear and desperation but admitted that she had the will. The therapist provided an interpretation of the client’s situation and emotions, including her anger, within the framework of her history. The client corroborated this interpretation with words and sighs. At around 25 min, the client recognized herself as being “a bit angry” about the situation, and after that, a steep rise in her RMSSD occurred.
The Second Rise in the Client RMSSD (40–43 min)At 40 min, after the client had talked about “guilt” and being a “weak, wrong, bad, evil person” and after having received validation of these feelings from the therapist, the therapist asked whether it would be possible for the client to interpret her feelings somehow other than being a bad person because of the feelings. The therapist shared her thoughts about how wrong it was that the client directed all the hatred toward herself and how sad it was. The client admitted that this was true but said that it was easier for her to be angry at herself and feel guilty than to be angry at others. She described how she showed her feelings to others by being “grumpy” at home, and even this gave her a guilty conscience; thus, it was better to direct her anger toward herself. The therapist validated the client’s feelings and the unfortunate circumstances of her life, which did not align with the client’s expectations. The therapist said that the current situation was sad, but neither of them knew what the future might hold. She reminded the client that she had not chosen to be in such a situation. However, the client explained how she thought she was to blame for her situation. Afterward, the client moved on to her earlier discourse of blaming herself for her thoughts and emotions (this co-occurred with a decrease in her RMSSD, however, this decrease was less than 1 SD).
Comments on the Rises in the Client RMSSDThere were two common nominators in these rises in the client RMSSD. On both occasions, she was able to name her condemnable or forbidden emotions and behavior, as she recognized being “a bit angry” and being “grumpy” at home. She could also stay with these emotions and reflect on them, and probably aimed to regulate them. On either occasion, she did not deny or reject the therapist’s interpretation of her situation, or the validation and empathy offered by the therapist.
Rise in the Therapist RMSSDThere were four time slots in which the therapist RMSSD showed clear rises. The first occurred at 12–14 min, the second at 18–22 min, the third at 27–32 min, and the last at 43–47 min. There was also a fifth one occurring simultaneously with a rise in the client RMSSD; this will be described later.
The First Rise in the Therapist RMSSD (12–14 min)During this time slot, the therapist was hardly talking, as she was mainly listening to the client’s talk about her unpleasant physical experiences and her thoughts and feelings concerning her family.
The Second Rise in the Therapist RMSSD (18–22 min)At 18 min, the client continued talking about her tearfulness last night and her thoughts about how everything was drifting away. Crying last evening had not felt comforting for her; it merely took her to her own space. The therapist validated the client’s emotions at 20 min. The client continued talking about her inability to be a good relative and how she felt that her failures were “being rubbed in her face.” After this, the therapist rephrased and interpreted the client’s thoughts and expressed her own sadness related to the situation. She encouraged the client to think about whether there were any ways in which the client could approach the “river of life”.
The Third Rise in the Therapist RMSSD (27–32 min)The client talked about her thoughts of not being a good relative to a child who was soon to be born to the extended family. The therapist summarized previous topics and interpreted the client’s thoughts about distancing herself from others. They kept talking about the will and fear of being close to the relatives and the client’s belief that she was not able to change. At 30 min, the therapist said that she also became angry about what was going on in the client’s life. The client sighed heavily, and the therapist encouraged her to fortify it. While the client was doing this, the therapists talked about possible feelings of sadness, anger, and guilt inside the client by suggesting that these feelings needed to be let out. The therapist also validated the client’s feelings, which the client did not do.
The Fourth Rise in the Therapist RMSSD (43–47 min)The client talked about how her situation was her own fault, blaming herself for her previous behavior and feeling incapable. The therapist replied by saying how cruel it sounded to blame the client’s younger self and called after self-compassion. The therapist encouraged the client to allow her to feel sorrow and listen to her tears. At 45 min, the therapist said that the sadness and the situation were not the client’s fault, and that the client was not bad; she repeated this phrase several times. Around this part of the session, there were long silences, but the therapist also talked quite a lot, describing the developmental process of the client, encouraging her to be self-compassionate and reminding the client how she can be proud of the work she has done.
Comments on the Rises in the Therapist RMSSDThere were two common features in the four time slots in which the therapist RMSSD rose. In the last three time slots, the therapist expressed her empathy to the client, and in the first one, she probably felt it, even though she did not express it, as she was only listening to the client. Alternatively, the therapist RMSSD rose in the first time slot as a reaction to the prolonged talk by the client and intensive listening while simultaneously preparing to reply. During the three time slots with the therapist’s empathy expressions, she talked a lot. It is plausible that it was the empathy felt by the therapist that mostly explained these rises. Interestingly, the client RMSSD did not rise simultaneously, despite the therapist’s expressions of empathy and validation. However, on three occasions (at 21, 34, and 37 min), a rise in the client RMSSD occurred either toward the end of the therapist’s speech and expression of understanding and empathy or soon after the therapist had stopped talking.
Rise in Both RMSSDsToward the end of the session, both the client and therapist RMSSDs were raised simultaneously; first, this was observed in the client (47–51 min) and then in the therapist (49–51 min). The therapist talked about whether there was a way for the client to defend against her inner voices, which were constantly claiming that the client was evil. The therapist also repeated her earlier remark that the client was not to blame, and that despite sadness, there were no reasons to feel guilty. The client said that she felt able to try to defend herself. The therapist told the client how punishing herself for her feelings felt cruel and wrong. The therapist also offered an interpretation that the client somehow felt rewarded for punishing herself, as if it were an absolution. She also reminded the client that accepting sadness and self-compassion needed rehearsal. Perhaps the empathy provided by the therapist was accepted by the client; the client teared up a little, which coincided with the time when her RMSSD was at its highest.
Comments on the Rises in Both RMSSDsIt is plausible that the therapist RMSSD mainly continued to rise as she interpreted and validated the client’s situation, that is, due to talk and empathy. It is probable that the empathy expressed by the therapist was finally received and accepted by the client at the end of the session, when she also teared up. Hence, it can be understood that the increases in the RMSSDs reflect both the shared understanding and emotions and the closure of the session, which may have allowed the emotion to finally be more freely expressed by the client.
Comments (0)