
Remember me






Autoimmune diseases arise when the immune system mistakenly attacks the body's own cells, driven by self-reactive T cells and autoantibodies, leading to chronic inflammation and progressive tissue damage. There are over 100 known autoimmune diseases and the top 10 affect almost 15 million people in the USA alone (Supplementary Figure 1). Despite the introduction of innovative disease-modifying therapies, much work remains to address unmet needs for autoimmune diseases, including side effects from treatments, lifelong treatment dependency, waning effectiveness over time and resistance despite treatment cycling.
Central to many therapeutic innovations is the recognition that B cells have key roles in autoimmune disorders. Because of their pleiotropic role, spanning antibody production, antigen presentation and cytokine release, B cells are a compelling therapeutic target for immune modulation. Current treatments, such as monoclonal antibodies (mAbs) targeted at the B-cell antigen CD20, provide temporary B-cell depletion, validating the effectiveness of this approach, although with varying success across indications. Emerging modalities, including cell therapies and multi-specific antibodies, hold promise for more sustained depletion, leveraging T-cell persistence. It is hypothesized that deep and sustained B-cell depletion could ‘reset’ the B-cell repertoire and re-establish immune tolerance, potentially leading to drug-free remission or even an eventual cure for autoimmune diseases.
This theoretical promise became clinical reality in 2022 when Schett and colleagues demonstrated through an investigator-initiated trial that CAR-T cell therapy could achieve rapid and sustained B-cell depletion and normalization of immunological parameters in five patients with refractory, life-threatening systemic lupus erythematosus (SLE). Remarkably, these patients remained in long-term, drug-free remission. This compelling evidence that the immune system could indeed be reset catalysed a global race to apply the approach in autoimmune disease (Supplementary Figure 2).
There are now around 85 different therapeutic candidates aiming to reset the immune system in clinical development, being studied across more than 380 clinical trials (Supplementary Box 1). Here, we analyse the characteristics of the candidates competing in this race and key trends in the field.
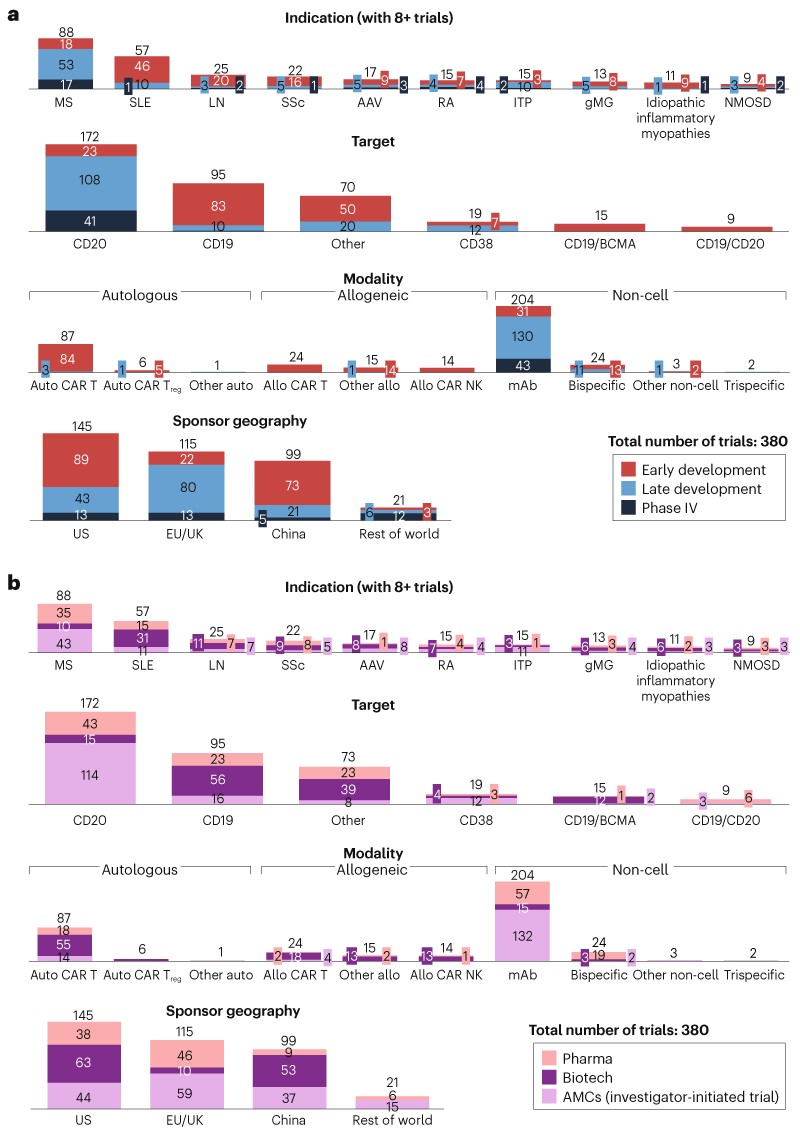
Competitor characteristicsKey modalities. The therapeutic candidates in development intended to provide sustained B-cell depletion fall into three main categories: autologous cell therapies, allogeneic cell therapies and non-cell-based therapies. While novel modalities such as allogeneic gamma delta CAR-T cells, allogeneic NK cells and autologous CAR-Treg cells have been extensively developed in oncology, their application in autoimmune disease R&D remains relatively limited (Supplementary Figure 3). This may be due to the more complex and diverse role of these cells in immune regulation.
Autologous cell therapies, such as the CD19-targeted CAR-T cells used by Schett and colleagues, are the most extensively researched modality, with almost 95 trials ongoing (Fig. 1). However, randomized controlled trials have not replicated the initial 100% response rates observed in earlier investigator-initiated trials, which may contribute to the observed volatility of stock prices for relevant biotech companies, despite positive data overall.

Fig. 1 | Characteristics of candidates aiming to reset autoimmune diseases. a, Candidates by development stage. b, Candidates by sponsor type. There are a total of 380 interventional-stage trials in this landscape analysis, sourced from ClinicalTrials.gov (see Supplementary Box 1 for details). Monoclonal antibodies (mAbs) are included for comparison, although these do not provide sustained B-cell depletion from a single treatment. ‘Other’ refers to single/multiple target assets not listed separately in the graph and undisclosed targets. AAV, ANCA-associated vasculitis; gMG, generalized myasthenia gravis; ITP, idiopathic thrombocytopenic purpura; LN, lupus nephritis; MS, multiple sclerosis; NMOSD, neuromyelitis optica spectrum disorder; RA, rheumatoid arthritis; SLE, systemic lupus erythematosus; SSc, systemic sclerosis.
Because autologous cell therapies are manufactured using each patient’s own T cells in individualized batches, substantial challenges remain with regard to scaling manufacturing, supply chain/patient logistics and patient monitoring for autoimmune disease populations. Biotech companies are at the forefront of early-stage development of these therapies, sponsoring 62 trials (66%). However, long-term success with this modality requires large-scale manufacturing, medical affairs and commercial capabilities that are typically possessed by large pharma companies.
Allogeneic cell therapies, which use donor T cells for an ‘off-the-shelf’ solution, have substantial advantages over personalized, autologous cell therapies with regard to manufacturing. They are 10–100-times cheaper and much simpler to deliver, improving accessibility for broader patient populations. However, data in oncology so far has shown modest efficacy compared with autologous cell therapies, probably due to limited persistence of donor-derived T cells, which are recognized and eliminated by host immune cells. So, a key scientific question is whether one-time depletion of B cells using allogeneic cells is sufficiently deep, despite limited persistence, to achieve a reset in autoimmune diseases, potentially leading to drug-free remission. Despite starting later than autologous cell therapies, allogeneic candidates are rapidly advancing, with several clinical readouts due in 2025.
Non-cell-based therapies that recruit endogenous T cells to target B cells, such as bispecific and trispecific antibodies, have shown promise in oncology, with 9 FDA-approved products. Although initial clinical data in oncology indicates strong efficacy, they are thought to have more transient effects in some indications compared to autologous CAR-T cell therapies.
Like allogeneic cell therapies, multi-specific agents are anticipated to offer a more streamlined manufacturing process, improved accessibility and a simplified healthcare delivery model compared to autologous cell therapies. In 2024, a series of case reports in which bispecific antibodies approved for oncology indications (blinatumomab, teclistamab) were used to treat patients with autoimmune diseases (such as systemic sclerosis, rheumatoid arthritis and SLE) provided initial proof of concept, prompting another wave of investment.
Key targets. Across the three major categories, several therapeutic targets are being explored, most notably CD19, CD20, CD22, CD38 and BCMA, enabling selective depletion of B-cell subsets to optimize the clinical profile for specific indications. Currently, CD20-targeted therapies dominate the landscape, with ~170 clinical trials ongoing (Fig. 1). This focus reflects the well-established clinical success for CD20 in blood cancers, for which it is a validated target for B-cell depletion.
Key indications. The 85 therapeutic candidates are being tested in almost 50 different indications, with crowding in indications that have the greatest commercial opportunity, strongest clinical proof of concept and most compelling scientific rationale (that is, B-cell-mediated autoimmune diseases). The most indications with the most crowding are multiple sclerosis (88 trials ongoing) and SLE (57 trials ongoing), while newer entrants are expanding into niche indications such as generalized myasthenia gravis and ANCA-associated vasculitis.
Key geographies. The US remains the leader in this space, with 145 trials ongoing, followed by China, with almost 100 trials ongoing. In both countries, biotech companies are the primary driver of trials, followed by academic medical centres, which contribute through investigator-initiated trials, and then pharmaceutical companies.
China has several structural advantages, including a large patient pool, a streamlined regulatory framework (dual-track for cell therapy), and cost advantages with contract research organizations, labour and manufacturing, enabling rapid, cost-effective, iterative experimentation. US and EU-based companies are taking note, sponsoring phase I cell therapy trials in China due to their speed and cost advantages in preclinical and early clinical development. It remains to be seen whether the early lead in the US will be sustained or if China-sponsored trials will quickly close the gap, as seen in other modalities.
OutlookWith 380 ongoing trials, only a limited number of treatments will emerge as market leaders —even blockbuster drug classes such as TNF inhibitors eventually supported only a handful of approved products. For autologous cell therapies in particular, existing operational capacity will soon be overwhelmed by the volume of trials, due to their operational complexity and infrastructure limitations (there are only ~200 hospitals in the US capable of providing bone marrow transplant and autologous cell therapy). In addition, clinical care for most autoimmune patients today occurs in large, non-academic hospitals that are unable to offer care for cell therapy, creating a mismatch of where the patients are today and where the future care needs to be delivered. If immune system reset is truly as transformative as the early promise suggests, it will be essential to scale cell therapy capabilities and expertise to ensure that research and care delivery can meet demand, allowing approved therapies to reach these patients.
Comments (0)