
Remember me


A total of six interviews were conducted with people who have daily interaction with palliative care patients and their relatives. The professions of the participants are physicians, coordinators, grief counsellors and social education specialists with a focus on palliative care. The age of the participants is between 27 and 64 years and two of them are male. Due to the small sample size, we are not able to disclose further characteristics, as their anonymity would be affected.
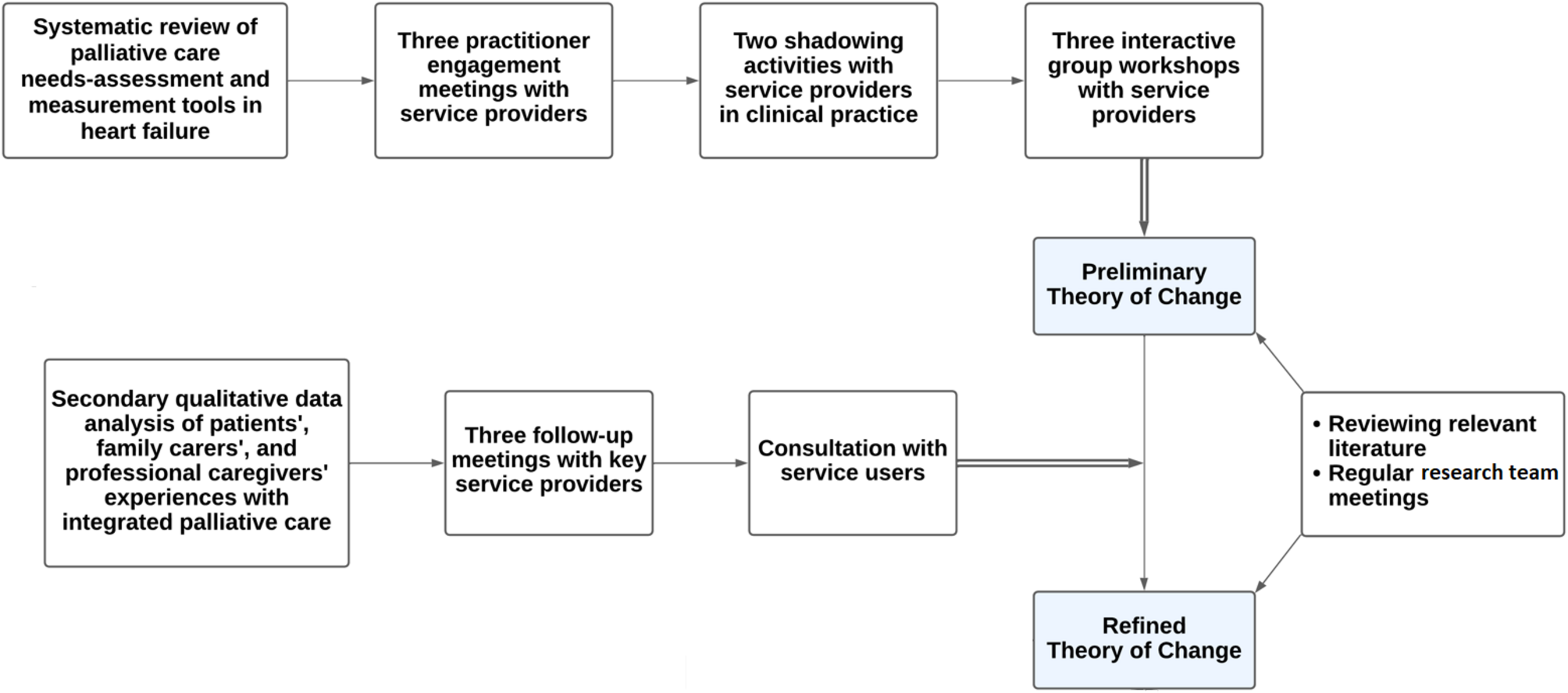
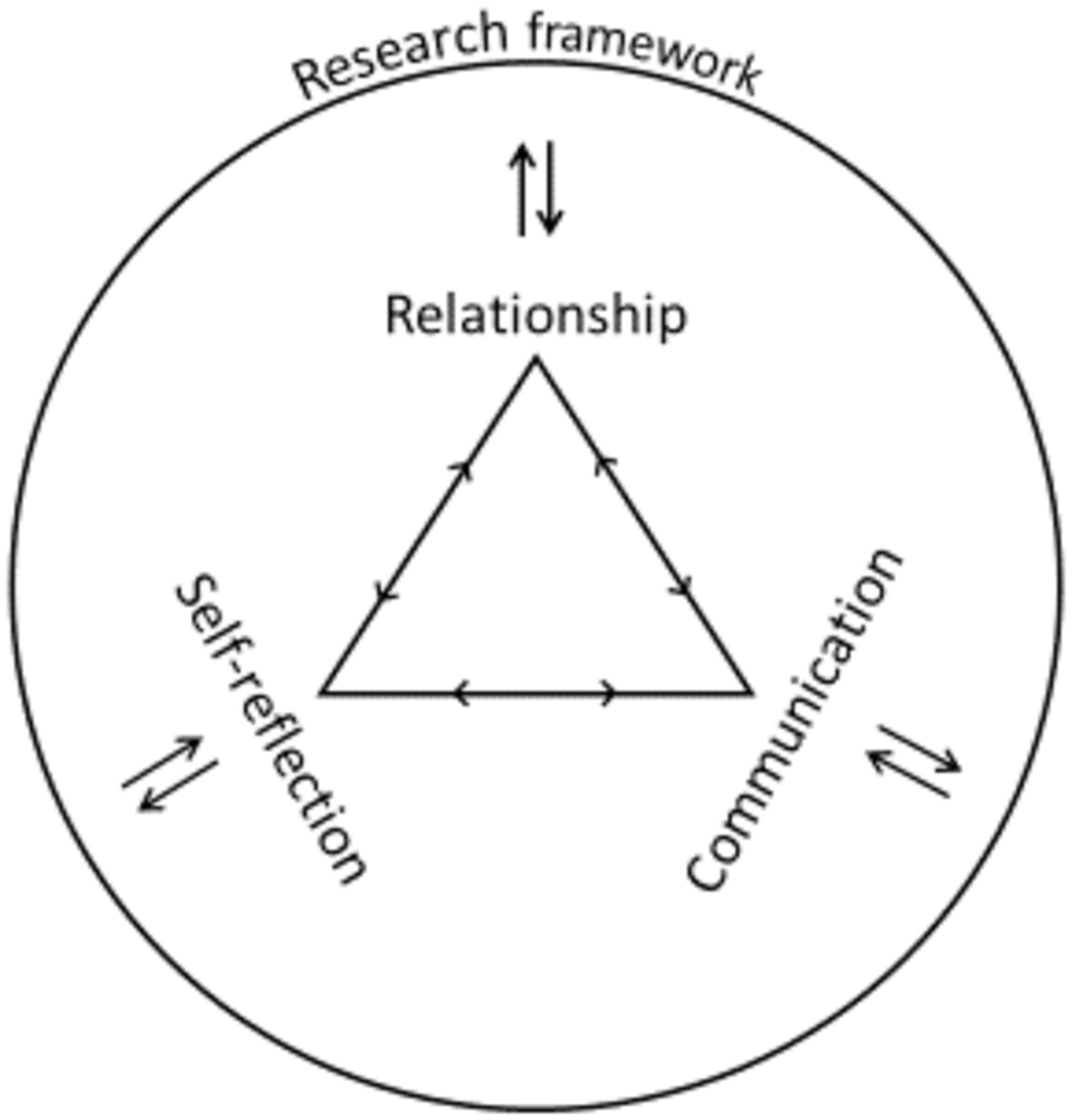
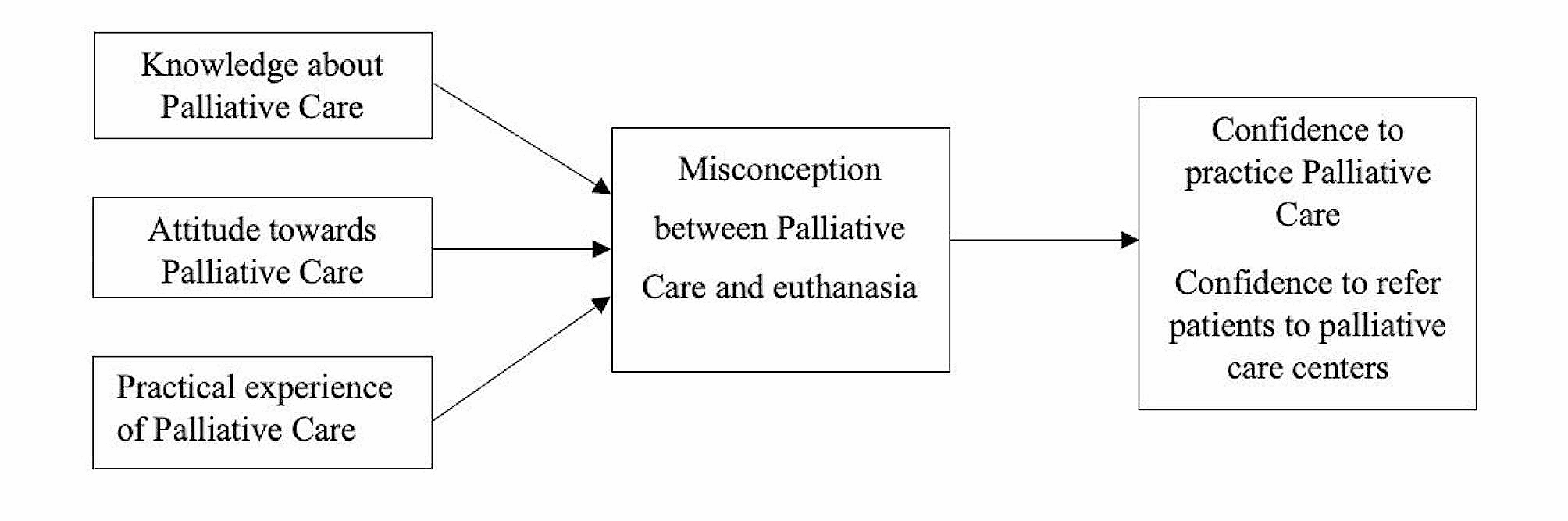
The presented results consist of four major topics that emerged during the analysis of the interviews to ensure that the needs of palliative care patients and their relatives are met in qualitative research interviews and that a clean and high-quality data collection can take place at the same time. Those topics should be considered when preparing and conducting data collection. The topics relationship, communication and self-reflection were developed from the interview data and are based on the previously established interview guide. The fourth theme, the research framework, results from the additional reflection on the results in connection with knowledge and scientific literature on the research process. In general, the interviewed participants have no reservations about offering palliative care patients and their relatives the opportunity to participate in scientific research– as long as the following points are considered in the research project. The three main topics of relationship, communication and self-reflection are of equal and interrelated importance in this context. In addition, the research framework (fourth topic) embeds these aspects and clarifies the overall range of external factors and preparatory measures that structure and support the research process. For a better overview of the topics, see the following figure (Fig. 1).
Fig. 1
Main topics emerged from the analysis
RelationshipIn qualitative research, the relationship between the researcher and the participant is of particular importance, especially when the topic is sensitive, such as in palliative care. A relationship of trust allows for more in-depth and honest conversations, which increases the quality and depth of the data. In addition, a good relationship helps to maintain ethical standards and treat participants with the necessary respect and empathy.
Trust is the foundation of any successful interaction, especially in sensitive contexts such as palliative care. To establish this trust, a researcher’s willingness to demonstrate openness, honesty, and an appreciation for the gravity of a patient’s situation is dependent. A fundamental element of this is the active involvement of the patient in the research process. This implies that the patient’s viewpoint is consistently prioritised, and their requirements and preferences are upheld. Such involvement serves not only to reinforce trust but also to facilitate the establishment of an authentic and collaborative relationship in which the patient feels secure and understood: „So I think it’s always about space, time and, in quotation marks, an understanding counterpart. In other words, open ears and an open heart” (grief counsellor).
In addition to building trust, it is important to recognise the patient as a whole and accept their needs. Researchers need to tune into the patient’s perspective and set aside their own point of view in order to truly understand them. When working with palliative patients, it is crucial to recognise and respect their individual needs and wishes. Needs-orientation means engaging with the patient’s perspective and understanding their ideas and wishes without imposing your own standards or ideas. Acceptance is the key here, as it requires accepting the patient in their entire situation and valuing their decisions and feelings: „I understand what his concerns and wishes are when I don’t start from my quality of life and not from my idea of his quality of life, but when I actually get to the level of communication where it’s really about him and not about me“ (physician).
Being able to respond appropriately to the patient’s needs requires empathy and sensitivity. Empathy involves putting oneself in the patient’s emotional position and understanding their feelings and concerns. Sensitivity, on the other hand, refers to the ability to deal gently with the patient’s emotional and physical needs without losing the necessary professional distance. This closeness enables the patient to feel understood and cared for, which is particularly important in sensitive situations. On the other hand, the researcher must maintain a certain distance in order to protect themselves emotionally and be able to act professionally. This distance is necessary to remain objective and limit one’s own emotional burden: „That you are not only empathetic with the other person, but also empathetic with yourself. In these sensitive conversations in particular, there are often points that are somehow close to you personally. […] So being empathetic, being accommodating. But not only to the person you’re talking to, but also to yourself“ (social education specialist).
One of the main ways of realising these aspects is through honest and respectful communication at eye level. As it has a significant influence on the relationship, its individual aspects should be looked at more closely.
CommunicationCommunicating effectively is not just an exchange of information, but also a way of building trust, understanding needs and establishing an empathetic connection. Especially in sensitive and emotionally challenging situations, the way in which communication takes place can significantly influence the progress and outcome of the conversation.
Honesty, authenticity and equal communication are essential components of a successful and trusting interaction between researchers and participant. It is about communicating openly and honestly. This means that the patient is perceived as an equal partner in the dialogue and that their opinions, wishes and needs are taken seriously. Such communication promotes trust and ensures that the patient feels heard and understood. A respectful exchange at eye level creates an environment in which the patient can express their thoughts and feelings openly and honestly without feeling ignored or patronised: „I think it’s important to be open and honest and tell the patient when they say it’s so bad at the moment that it is bad, and not necessarily sugarcoat it. That there is simply honest communication” (coordinator).
As communication does not occur exclusively on a verbal level, non-verbal communication should also be considered. It includes all forms of communication that take place without words, such as facial expressions, gestures, posture and eye contact. These subtle signals can often reveal more about a person’s inner attitude and emotions than spoken words: “I pay attention to the signals that the person sends me, to their emotional situation, their mood, their wishes, their concerns. I ask them questions. I take breaks in the conversation. I try not to dominate the conversation, but to give them the space they need” (physician). It goes without saying that researchers communicate things about themselves through non-verbal communication as well. Since communication always goes in two directions, the researcher should also pay attention to his own signals.
When non-verbal signals are perceived, it is up to the researcher to react flexibly and spontaneously. They enable an appropriate response to unexpected situations and emotional reactions. Flexible communication means being able to deviate from the planned course of the conversation in order to respond to the current needs and emotions of the other person. This applies both in terms of content and form. Once again, this shows a balance of needs-orientation and good data collection: „I have an internal structure of what I want to know and yes, then I think ahead, but of course I answer or respond to what the patients say. And that’s just so important or so interesting […] and you have to find a compromise somehow so that both of us come out of it well” (physician). At the same time, effective non-verbal communication also requires a high level of sensitivity and awareness of one’s own emotional reactions and boundaries. This is where self-reflection becomes a key element in the process.
Self-reflectionOnly through good self-reflection before, during and after such conversations can high-quality data collection succeed while considering and respecting the needs of all involved. As preparation and follow-up, researchers should reflect on their own experiences with the topic. This is a continuous process and should not only be realised before a study is conducted.
A fundamental palliative attitude can be developed through the process of coming to terms with one’s own finiteness and experiences within this context. It should be noted that this is not a fixed state of being; rather, it is constantly evolving: “But I believe that most, or hopefully all, of those who work in these areas are, on the one hand, very professionally competent and qualified and have hopefully all dealt with their own experiences and experiences that have to do with farewell, grief and death. And if they have done that, […] they have developed such an attitude for themselves, and it can’t be detached from themselves” (grief counsellor). This attitude is mentioned in several passages, as it has a fundamental influence on the entire research process.
Furthermore, the process of self-reflection occurs concurrently while collecting data. Through the awareness of one’s own attitude and perceptions, one is faced with the challenge of endurance. Since reality does not always go hand in hand with what one wishes for or perceives as good, in the research process it also applies to support and endure the participant’s situation and emotional world: “And many of us have an idea of what is beautiful and what is not and what is reasonable and what is not. Everyone has their own idea, and it is often the case that we differ greatly from this and that you have to endure it personally - that was actually a learning process for me, and I don’t think it happens overnight. […] And I also accept that the situation cannot be changed at the moment because that is what the person wants” (coordinator). In order to remain able to act appropriately in such situations, researchers should consider in advance how they would deal with other views and react to them.
In addition to their own palliative attitude, researchers are also required to pay attention to their own emotions and practise mental hygiene. This can be realised by exchanging experiences and views with colleagues in the research team and by reflecting on one’s own needs, such as taking a walk after the interview.
Research frameworkAll the factors mentioned are influenced by external and preparatory measures that are intended to structure and support the research process. The research framework comprises structural and organisational aspects of the research, including the temporal and geographical context as well as preparation and follow-up.
Since the centre of the temporal context consists of flexibility and orientation towards individual needs, the health condition and daily routine of the palliative care patients should be considered when planning the interview times. This also influences the planned duration of the interviews, as it is better to plan additional backup time. On the one hand, greater time capacity means that the interview can take place in a calm atmosphere and the researcher is not rushed. On the other hand, with this flexibility the researcher can integrate breaks as well, when needed: “You notice that the pauses are getting longer or, or, or. That you then just say briefly that we’re going to take a break or simply ask the other person: “How is it for you right now?” Should we take a break? Should we perhaps pick it up again at another time?” (social education specialist). Nevertheless, a broad time frame should be set in advance to obtain a realistic expectation among the parties.
Regarding the geographical context, it is most important that the participant feels safe. The conversation should take place at a location without disruption and for this reason, and to create and maintain a basis of trust, a door can be closed, for example. In most cases, conversations with palliative care patients take place in their own homes. However, this information is particularly useful if the conversation takes place in a different location, such as a hospice: “So I think that the environment should be like this and I always try to ensure that the conversations I have are in a closed room or a closed area where you can actually achieve confidentiality so that outside influences don’t interfere with the conversation” (physician). One participant even named the seating position as a factor, that should be considered. Here too, there is no right or wrong and each person should figure out for themselves whether they prefer e.g. to sit with their back to the door, sideways next to the participant, face-to-face in front of them or in any other way. This example shows that it is often small aspects that can have a big impact on the well-being of those involved in the conversation and consequently on the result of the data collection.
The personal preparation of the researchers for the interviews is also a component of the research framework. Directly before an interview, researchers should check in with themselves and pay attention to their own needs. By fulfilling them in advance, the researcher can concentrate on their interview partner. This kind of ritual can help to approach the situation with calm and a clear mind: “Of course, I have to pay attention to how I’m doing personally. I have to develop rituals to take my time. I also mean making time mentally for this conversation, for this patient. In other words, I have to try to put everything else aside and concentrate only on the patient in this conversation, in this communication.” (physician). Other examples of rituals mentioned in the interviews are taking a deep breath, going for a short walk or wearing certain clothes.
Rituals also play an important role in the follow-up. First of all, the conversation should be documented. A standardised procedure is usually used for this, especially in the context of research. However, the individual’s own feelings should also be reflected and documented in this context. Also, after the interview, the researchers should check in with themselves and consider what is needed. Since the content and context of such interviews can be exhausting for the researcher, self-reflection and orientation towards one’s own needs are also relevant here. It is important to find out whether it is different things, such as a phone call with colleagues or a short walk, or whether the researchers establish a ritual that they carry out after the interviews. For example, one participant mentions: “And I actually have an outlet, I sit in the car afterwards and always like to listen to loud music (laughs). That’s my outlet to relax” (coordinator).
Not only after the interview, but also in other situations, it is important to exchange experiences with colleagues or to ask for collegial supervision. Especially when it comes to sensitive topics that are discussed in interviews with palliative care patients or the situation itself. Exchange with colleagues and the research leader must be ensured throughout the research process. This is the only way to ensure structural security for the researchers and, as a result, for the palliative care patients and their relatives.
Comments (0)