
Remember me


This study was a randomized controlled trial. The Consolidated Standards of Reporting Trials statement for the study design and reporting was adopted from a previous study [27].
SettingThis study was conducted in cardiac centers of the three teaching, specialty, and subspecialty Nemazee, Faghihi, and Al-Zahra hospitals affiliated with Shiraz University of Medical Sciences (SUMS). These three hospitals are the main centers in southern Iran and offer specialized heart and vascular disease services, which are equipped with Coronary Care Units, Post CCU, Post Angiography, Cardiac Operating Room, and ICUs [28].
ParticipantsThe participants included all patients over 18 years of age who were candidates for coronary artery bypass grafting surgery, and their records were available at the heart centers. Sampling continued until the intended number of participants for each group was achieved. Study enrollment started on 25 October 2021 and ended on 15 January 2022.
Inclusion and exclusion criteriaThe study’s inclusion criteria were 18 to 65 years old, being able to speak and write in Persian, being willing to give written consent and having no history of cardiac surgery. The exclusion criteria were not understanding the study methods, being diagnosed with a psychiatric disorder according to DSM-5, having taken part in structural interventions related to patient caring during the past six months, fever and infection after the surgery, and occurrence any problem during surgery and anesthesia, such as causing complications.
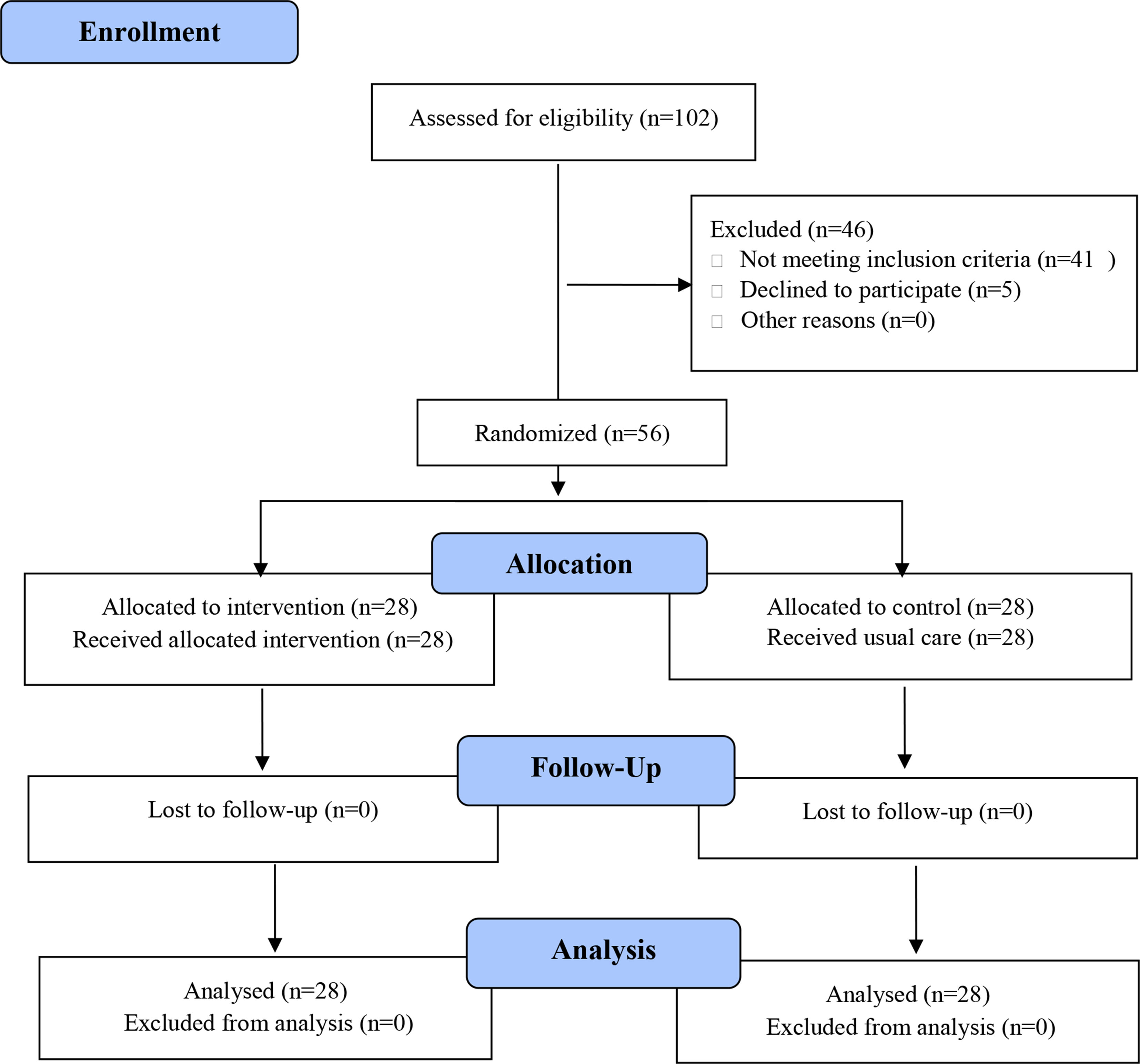
Sampling and sample sizeBased on the study conducted by Abbaszadeh et al. [29], using G*Power3 software and considering the power of 0.8, error of 0.05, and loss rate of 10%, effect size Cohen’s d = 0.796, 56-subject sample size was estimated for the study. The participants were randomly allocated in 14 blocks of 4 into intervention and control groups using a computerized random number generator (Random allocation software), ensuring a 1:1 allocation ratio. Each block, therefore, resulted in the allocation of 28 individuals to each of the two groups.
A trained nurse, who was blinded to the study groups, conducted face-to-face interviews to complete the questionnaires. At first, the nurse explained the information regarding the study process and intervention program to participants and ensured that they received sufficient information and understood the nature of the study to enable them to feel less doubtful about accepting the intervention program. Participants gave informed consent voluntarily and were comfortable and able to accept or reject the information presented. Participants were assured that they could withdraw from the study anytime without interfering with standard care. Then, the participants’ informed consent forms were obtained, and their basic information, including demographic and pre-assessment data, was collected by data collection instruments. Based on the study design one day before the operation, the McGill pain and Spielberger’s StateAnxiety Inventory were completed by the intervention and control groups. Physiological indicators (blood pressure, heart rate, breathing rate, arterial blood oxygen percentage) were measured via monitoring and recorded by the trained nurse in the same situation on the same day. The information related to the post-assessment was collected from all the study participants by McGill pain and Spielberger’s State-Anxiety Inventory and measurement of the physiological indicators via monitoring. Once patients showed signs of recovery, usually 48 h after surgery, they were transferred to the cardiac surgery ward. Post-assessments were performed 24 h after transfer to the ward, before discharge. Patients were usually discharged 24 h after transfer to the ward.
Data were gathered by the same researcher to maintain reliability.
Full blinding of researchers and participants was not possible in this psycho-educational trial; however, blinding was applied to data collection, data management, and statistical analyses.
InterventionThe intervention was provided individually with face-to-face interviews, consultation, and training for each participant in the intervention group through three 30-min psycho-educational sessions with 3-4-hour intervals on the one day before the surgery in cardiac ward. The content of psycho-educational interventions was evaluated and validated by the research team and nursing specialists. Also, the educational booklet and pamphlet, which included a summary of the intervention, were provided to the patients.
Educational interventions included practical breathing exercises after heart surgery and how to use spirometry, self-care training, and nutritional care after surgery, giving information about the period of the disease and treatment, common medications after surgery and their side effects, and how to take care of the surgical site, stitches and chest tube. Psychological interventions included teaching mindfulness breathing exercises. The psychological protocol was done again in a one-hour meeting 48 h after the surgery at the time of transferring the patient from ICU to the ward and before discharging from the ward. At the end of each session, clarification with further teaching was provided if necessary. In this study, the control group participants received the usual care protocols, which included brief verbal instructions on post-surgery care, such as medications, nutrition, activities, and surgical site care. However, after the study, the control group was provided with educational content, including audio files and pamphlets. The CONSORT flow diagram of the study is depicted in Fig. 1.
Fig. 1 InstrumentsDemographic information form
InstrumentsDemographic information formDemographic information form included age, sex, marital status, occupation, and education level.
Short-Form McGill pain questionnaire (SF-MPQ)The McGill Pain Questionnaire (MPQ) was created in 1975 [30] and has become one of the most widely used tests for pain measurement. It provides valuable information on the sensory, affective, and evaluative dimensions of pain experience and can discriminate among different pain problems [31]. In 1987, the short form-MPQ (SF-MPQ) was designed and proven to have excellent validity and reliability [32]. The SF-MPQ was further revised in 2009 for various pain conditions (SF-MPQ-2). SF-MPQ-2 includes 22 items with 0–10 numerical response options. Based on the results of these EFAs, four SF-MPQ-2 subscales were established. The results of the CFA demonstrated a good fit for the SF-MPQ-2 subscale. Internal consistency reliability, a Cronbach’s alpha of r > 0.75, has been reported [33].
The Persian translation of the SF-MPQ-2 is a reliable and valid instrument for evaluating pain in Iranian patients with and without neuropathic etiology [34]. Exploratory factor analysis has revealed four components similar to the original SF-MPQ-2. Cronbach’s alpha was reported to be above 0.80, which showed high internal consistency [34]. Interclass correlation coefficient (ICC) of more than 0.90 has demonstrated adequate test–retest reliability. There was also a high correlation between the mean VAS and the mean total score (r = 0.92) [34, 35]. In this study, Cronbach’s alpha approved the scale’s internal consistency of 0.82.
Spielberger’s State-Trait anxiety inventory (STAI)Spielberger and colleagues developed the State-Trait Anxiety Inventory in the USA in 1970 [36]. It has 40 items, 20 of which evaluate the state anxiety, and the remaining items analyze the trait anxiety. The State Anxiety Inventory (SAI) consists of 20 phrases, which assess the feelings of the respondent at the moment and at the time of response. The Trait Anxiety Inventory (TAI) has 20 items, which evaluate the general and normal feelings of the respondents. The internal consistency coefficient of STAI has been confirmed at Cronbach’s alpha of 0.92. Items scored on a 4-point Likert scale. The lowest score is 20, and the highest is 80 [37]. Internal consistency coefficients for the scale have ranged from 0.86 to 0.95; test-retest reliability coefficients have ranged from 0.65 to 0.75 over a 2-month interval (Spielberger et al., 1983). Test-retest coefficients for this measure in the present study ranged from 0.69 to 0.89. Considerable evidence attests to the construct and concurrent validity of the scale (Spielberger, 1989). The STAI scores of < 40 reveal no or minimal symptoms, and ≥ 40 indicate the presence of moderate or severe symptoms [38]. The STAI has established validity and reliability in Iranian society. Mahram verified scientific reliability using Cronbach’s a, which was 0.9452 in the normal community and 0.9418 in the standard community [39]. In research by Khanipour, the internal consistency coefficient of the instrument was estimated at the Cronbach’s alpha of 0.66 [40]. In study by Gholami Booreng et al. (2017), reliability was 0.87 via Cronbach’s alpha and 0.76 via re-test after seven days [41]. In this study, the State Anxiety Inventory (SAI) was used to measure anxiety levels. Its reliability was assessed, and Cronbach’s alpha confirmed a strong internal consistency (α = 0.79). The SAI scores range from 20 to 80, with higher scores indicating greater levels of anxiety.
Data analysisSPSS version 21 was used for data analysis. Descriptive data were presented using tables and charts (mean and standard deviations). Independent samples t-test and chi-square test were used to determine the homogeneity of the study groups by comparing participants’ characteristics and scores. Additionally, an independent t-test was conducted to assess potential differences between participants at baseline (pre-test).
In the post-test, an independent samples t-test was used to evaluate differences between the two study groups in terms of the mean scores of study variables. Changes in the outcome variable from pre-test to post-test were analyzed using a paired t-test.
All tests were two-tailed, and the statistical significance level was set at 0.05.
EthicsThe Institutional Human Ethics Committee of Shiraz University of Medical Sciences approved this study (IR.SUMS.REC.1400.175). Then, the researchers started the sampling after trial confirmation at the Iranian Registry of Clinical Trials (IRCT) with the code IRCT20090908002432N8 (2021-09-17). Voluntary participation informed consent written forms were obtained from all the participants included in the study after providing complete information about the study objectives and procedures. Moreover, all the participants were assured about the confidentiality of their data and that they could withdraw from the study at any time without interfering with standard care. All procedures performed in this study complied with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Comments (0)