
Remember me





This was a retrospective observational study. The St. Antonius Hospital’s medical ethics committee approved the study protocol (W23.069).
Study populationTelemonitoring groupFrom February through May 2022, 78 patients who underwent PVI were enrolled, and remote follow-up was conducted using PPG. Remote monitoring was overseen by a team of trained eNurses stationed at a telemonitoring centre (TMC). ENurses are nurses trained on specific topics, such as AF. They are able to answer AF-related questions from patients about symptoms, heart rate and heart rhythm and can give medication advise. The eNurses worked online and monitored the measurements from participants remotely but did not perform face-to-face consultations. On-call cardiologists were available to answer questions from eNurses and prescribed medication.
Control groupThe control group comprised 79 patients who underwent PVI between January and April 2019 as a pre-COVID cohort. Follow-up was performed according to standard care, consisting of a visit to the outpatient department at 3 months, during which an ECG was performed to detect AF or sinus rhythm. Referred patients returned to the referral hospital, while local patients had a 12-month outpatient visit. Holter monitoring was performed at the discretion of the treating cardiologist.
Study proceduresOnboarding telemonitoring groupAt the virtual AF clinic, patients received written information on the background and objectives of remote monitoring using TM. They were instructed to download the PPG application, create an account with a two-step verification and perform a test registration, during which they were supported by means of an informative brochure with step-by-step instructions. The brochure also provided information about heart rhythm measurements. Patients were informed they could perform a heart rhythm measurement when it was convenient or if they experienced symptoms. Furthermore, for each measurement, they could indicate whether symptoms were present at that time. The brochure gave tips for performing measurements as well, such as keeping their phone on silent during measurement, ensuring their hands were warm and not talking during the measurement. The application also offered the possibility to contact the healthcare provider if the patient had any questions and read information about heart diseases and medication. Additional support and informed consents were provided by eNurses.
Additionally, patients received questionnaires via email during onboarding and shortly before offboarding, again with the option to contact the eNurses if desired.
Photoplethysmography application in telemonitoring groupFor AF detection, a smartphone-based PPG application (Happitech, Rotterdam, the Netherlands) was used (see in Figure S1 in Electronic Supplementary Material), employing an algorithm previously described [8]. In short, this algorithm utilises peak detection to measure RR intervals, determining the heart frequency and quality of measurements while providing a rhythm classification (regular (= 0, implying sinus rhythm) or irregular (= 1, implying AF)). Patients can report AF-related symptoms in the application, which is integrated into a digital health platform (Luscii, Utrecht, the Netherlands).
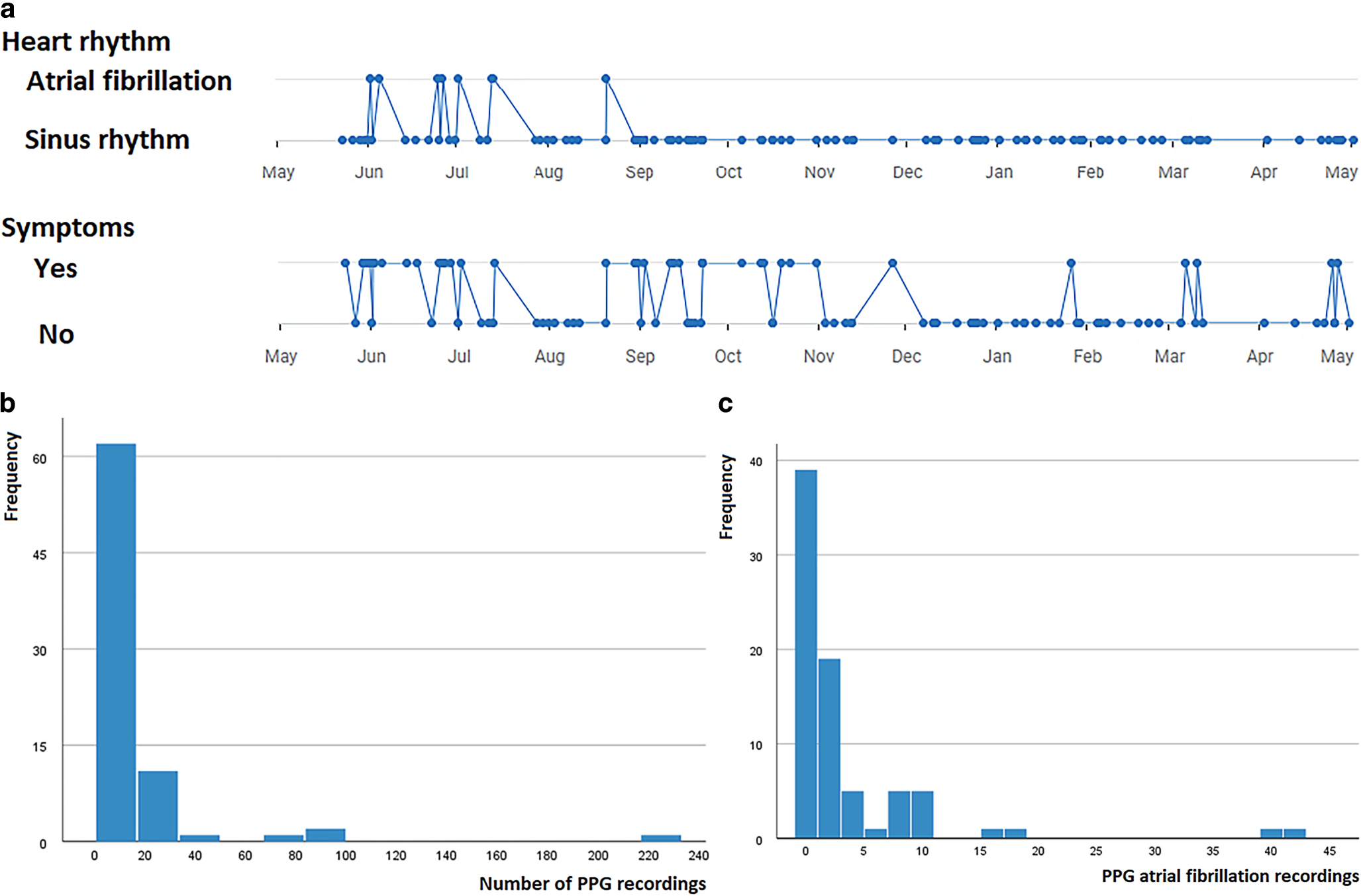
Study participants used the application for heart rhythm measurements if they experienced symptoms. The results of each measurement were displayed and automatically uploaded to a server, accessible from the electronic health record (EHR; Epic Hyperspace, Verona, WI, USA). In the EHR, cardiologists could access patient summaries, which displayed the PVI date, measurements, rhythm classification and symptoms on a time scale (Fig. 1a). Drill-down options allowed access to individual measurements.
Fig. 1
Photoplethysmography (PPG). a Time plots of rhythm classification and symptoms, as shown in digital health platform Luscii, b number of PPG recordings and c number of PPG-determined atrial fibrillation recordings
Offboarding telemonitoring groupThe monitoring period ended at 12 months. The numbers of measurements with and without AF were noted, and a report of these findings was documented in the EHR and sent to the referral hospital.
A validated AF patient-specific satisfaction questionnaire, the Atrial Fibrillation Effect on QualiTy-of-Life (AFEQT) questionnaire, was sent to all patients at the start of the programme (baseline) and after 1 year of follow-up [14]. The AFEQT questionnaire includes questions about how AF affects patients’ daily activities, symptoms, treatment satisfaction and overall well-being. In this study, we used only the overall score.
Data collection and analysisProtocolTM patients were instructed to perform measurements if symptomatic and were free to perform measurements at any other time. No blanking period was observed. Patients were informed that the TMC would be alerted if their heart frequency was < 30 or > 140 bpm. Individual measurements were not routinely assessed. Patients were instructed to contact the TMC for application-related, PPG-related or AF-related questions or problems. A supervising cardiologist oversaw the TMC during office hours, 5 days a week. The TMC was staffed 7 days a week during office hours.
The online Luscii platform was used for the TM of study participants. The platform was accessible 24/7 by all eNurses and cardiologists, including on-call cardiologists. Vital functions, such as heart rate, heart rhythm and symptoms (in the current version, this was a binary variable, i.e. yes or no), were visible when participants performed PPG measurements. Additionally, participants were able to contact eNurses in the Luscii platform via online chat.
At 3 months, a remote consultation with the cardiologist was scheduled, including a discussion of the PPG measurements. If the patient was free of AF symptoms, anti-arrhythmic drugs were stopped. After this consultation, patients were referred back to the referral hospital for a 12-month follow-up or, for local patients, a 12-month consultation was scheduled in our hospital. These scheduled consultations at 3 and 12 months were part of the planned remote contacts. Patients received a questionnaire containing questions whether follow-up by PPG met their needs (see 2 Dutch-language questionnaires in Electronic Supplementary Material).
Data were collected using the Research Electronic Data Capture system. Custom-built electronic case report forms ensured real-time data validation and integrity checks.
AnalysisFor the TM group, PPG measurements and contacts with the TMC were documented, as well as the patient satisfaction results. In all patients, both scheduled and unscheduled remote contacts and outpatient contacts, emergency room presentations, cardioversions and AF-related hospital admissions were documented, together with the numbers of ECGs, event recorders and Holter recordings. The number of hospital contacts in our hospital was collected manually by EHR assessment. The hospital contacts in the referral centres were not included in the analysis. This method was similar in both study groups. Follow-up was conducted at 1 year in all patients.
Statistical analysisData from all included participants were analysed, and missing values were not imputed. Data are presented as mean ± standard deviation (SD) for normally distributed continuous variables, median (interquartile range; IQR) for non-normally distributed variables and number (percentage) for categorical variables. As this was an observational study, there was no formal hypothesis or statistical plan, and no power calculation was performed. Continuous data were compared using the unpaired t-test or Mann-Whitney U test for two-group comparisons. Categorical data were compared using the χ2 test or Fisher’s exact test when a small number of events was observed. Event-free survival is graphically depicted using the Kaplan-Meier method. All tests were two-tailed, and the limit for statistical significance was set at p < 0.05. Statistical analysis was performed using SPSS version 28.0.1.0 (IBM, Armonk, NY, USA).
Comments (0)