
Remember me




Initial screening of the retrieved patient lists resulted in 262 patients who were eligible for further in-depth assessment. A total of 159 patients were excluded: the causes for exclusion are available in Supplementary Material 1. A total of 103 patients (60 men, 43 women) met the inclusion criteria and had a mean age of 45.7 (range: 23–75) years. The mean age of the women was 44 (range: 23–71) years and the men 47 (range: 24–75). The age of one patient at diagnosis was not identifiable, since the patient had presented with symptoms outside of Sweden and did not remember the date of diagnosis, nor were original copies of medical records available.
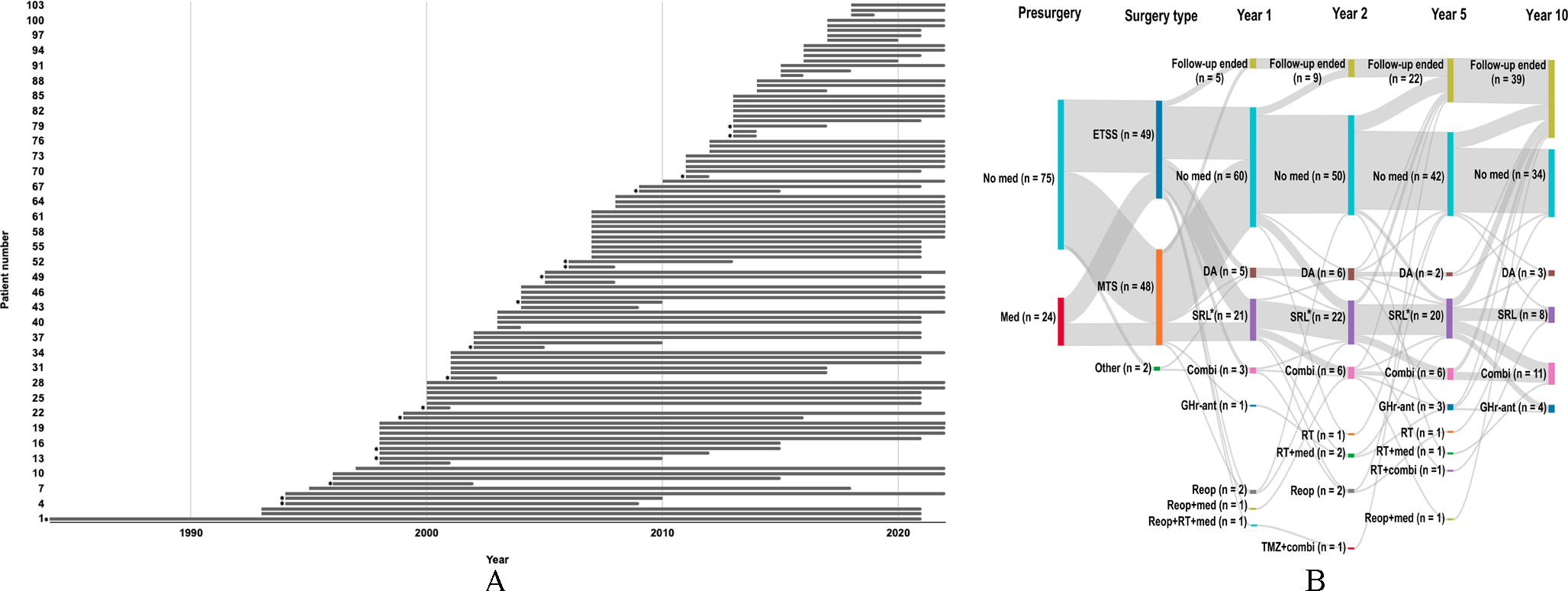
Fig. 1
Overview of the long-term follow-up. (A) Timeline (1984–2022) of patient follow-up from initial diagnosis to last follow-up. Two patients had their initial diagnosis in another country but, in the chart, this is depicted from the time their diagnosis was established in Swedish medical care. Patients may still be under surveillance in 2022 even though their latest follow-up was in, for example, 2021. *Patient deceased at the end of the study period. (B) Treatment pattern on a group level for the cohort. Nodes represent: (1) medication or not before first surgery at Sahlgrenska University Hospital; (2) surgery type; and node 3–6) current treatment option at follow-up 1-, 2-, 5- and 10-year post-surgical follow-up. Abbreviations: Combi, combination therapy (SRL and/or DA and/or pegvisomant); DA, dopamine agonist; ETSS, endoscopic transsphenoidal surgery; GHr-ant, GH-receptor-antagonist/pegvisomant; Med, medication for acromegaly; MTS, microscopic transsphenoidal surgery; Reop, reoperation; SRL, somatostatin receptor ligand; RT, radiotherapy; TMZ, temozolomide. *, Including treatment with second generation somatostatin receptor ligand
The duration of follow-up for individuals in the cohort is presented in Fig. 1A. All surgical treatments were primary treatments except for two individuals who had already undergone previous surgery at other centers. A total of 93 patients (90.3%) underwent a single surgery and the remaining underwent two (n = 9) or three (n = 1) surgeries. All of the cases of acromegaly were sporadic, except one patient who was diagnosed with multiple endocrine neoplasia type 1.
Radiological characteristicsPre-operative magnetic resonance imaging was available for adenoma size measurement in 99 of 103 patients: a macroadenoma was identified in 76 (76.8%) and microadenoma in 23 (23.2%). It was possible to interpret invasiveness in 97 of 103 patients: the adenoma was locally invasive in 46 (47.4%) and non-invasive in 51 (52.6%).
Table 1 Adenoma characteristics and patient gender by type of IHC hormone expression of 101 casesHistological diagnosesThe majority of interventions (96/111; 86.5%) were performed before 2016. IHC stains for transcription factors were therefore not available for most cases and only a low frequency stained for cytokeratin CAM5.2. Most of the histological diagnoses in the cohort were based on hematoxylin and eosin, and IHC stains for somatotropin, prolactin, and adrenocorticotropic hormone. Some cases were also stained with antibodies against thyroid-stimulating hormone. The following groups were therefore constructed: somatotropin, somatotropin/prolactin, and prolactin. Distribution of cases is presented in Table 1. Of the 103 patients, 101 had a histopathological hormone profile for diagnosis. For the two patients who did not, one of which was simply described as “relapse of pituitary adenoma” and, in the other, the tissue was not definitely identified as adenoma but was described as a macroadenoma on magnetic resonance imaging.
Surgical outcomeFor the cohort of 103 patients, 111 surgeries were performed during 1994–2022 at Sahlgrenska University Hospital. Three additional interventions were performed in other centers. Ten patients underwent reoperation during their course of disease. All but two of the 111 surgeries were performed by neurosurgeons or a cooperation between neurosurgeons and otorhinolaryngologists. Two of the operations were performed by otorhinolaryngologists alone with the purpose of obtaining a biopsy specimen. In the cohort, 101 patients had their first pituitary surgery at Sahlgrenska University Hospital within the study period. A total of 28 individuals had medical treatment for acromegaly before any of their surgeries although only 24 of these had sufficiently complete records to be included in Fig. 1B. The dominant surgical technique during the period shifted away from microscopic transsphenoidal surgery to endoscopic transsphenoidal surgery. Mean hospital stay in the neurosurgical and endocrine ward all together was 12 (range: 4–30) days.
Table 2 Post-surgical complications until discharge from hospitalPost-surgical complications (surgical and/or hormonal) until discharge from hospital are summarized in Table 2. For the primary surgeries, only one required premature termination due to excessive bleeding at the surgical site. Surgical complications occurred for 15% of procedures. Six patients had suspected liquorrhea but only two of them required treatment (one with lumbar drain alone and the other with lumbar drain and reoperation). Hormonal disruptions, including either an excess or deficiency of anti-diuretic hormone and hypopituitarism necessitating hormone replacement therapy, were observed in 25% of cases. Of the eight cases of diabetes insipidus, five patients were still treated with desmopressin around the time of their 3-month post-surgical follow-up. Counting cases with surgical and/or hormonal complications together, the rate of complications was 37%.
Table 3 Number of patients with records at follow-up times and reasons for missing recordsTable 4 Hormone replacement therapies at follow-upThere were 88 patients who had a recorded hospital contact between the time of discharge up to 3 months post-surgery. One patient had a complication 1 week after discharge but no visit within the 3-month follow-up interval, which accounts for the discrepancy in Table 3. In this cohort, four (4.5%) individuals suffered epistaxis sufficiently severe to the point medical assistance was needed and four (4.5%) other individuals contracted a local infection in relation to the operated area. One (1.1%) additional patient had bleeding in the residual adenoma and also had an ischemic stroke. No mortalities related to surgery were identified during this period. Apart from the aforementioned complications, 13 out of the total 88 patients (14.8%) complained about subjective symptoms but did not experience any severe complications. The most common complaint noted in the medical records was headache or pain (n = 7). Other subjective symptoms were tiredness and nasal congestion.
Long-term follow-upIn November 2022, 68 patients (66%) of the initial cohort were still under active monitoring. The average follow-up duration was 12.7 (range: 0–37) years. The cause of no recorded follow-up at the set follow-up times is presented in Table 3. The most frequent cause of no recorded follow-up at 10 years post-surgery was that insufficient time had passed since the intervention.
A total of 53 (51.5%) patients who had a follow-up time of ≥ 1 year did not receive any further medical treatment post-surgery, whereas 43 (41.7%) were given additional treatment for acromegaly during their specific follow-up period. Four cases (3.9%) could not be evaluated due to follow-up < 1 year and three cases (2.9%) were not evaluated due to missing records or did not receive surgery by a neurosurgeon. In this subgroup of patients without further medication, 14 cases were identified as microadenomas and 38 as macroadenomas, and one case did not have data on adenoma size.
For the evaluation of biochemical control of the disease, 74 (71.8%) patients reached biochemical control of acromegaly (IGF-1 ≤ ULN) with multimodal treatment during their follow-up, whereas 15 patients (14.6%) did not. Overall, parts of the medical records were not obtained for 11 (10.7%) cases; thus, no certain conclusion could be made concerning biochemical control. For three (2.9%) patients no post-surgical follow-up was recorded. At 1-year post-surgery, 86 patients had a recorded follow-up and 43 (50.0% of that group but 41.7% of the total cohort) patients had obtained biochemical control of acromegaly. For those patients with data on invasiveness and biochemical remission at one year follow-up, 40% (16 out of 40 patients) with invasive tumors and 71.4% (30 out of 42 patients) of those without invasive tumors reached biochemical control at one year follow-up. At the 2-year post-surgery follow-up, there were 78 records where laboratory results were found and two cases where the laboratory results were not located, which accounts for 80 patients followed up in Table 3: 49 (62.8% of that group but 47.6% of the total cohort) were under biochemical control. At 5-years post-surgery follow-up, 69 patients had a recorded appointment and 45 (65.2% of that group but 43.7% of the total cohort) patients had biochemical control, although 11 (10.7% of the total cohort) patients still had an IGF-1 > 1.3× ULN at this follow-up. In these 11 uncontrolled patients, the mean IGF-1 ULN was 2.0 (range 1.3–3.6). Out of these uncontrolled patients, 7 had either medical treatment or had prior received radiation therapy. The information about if the remaining 4 patients had intolerance, adherence issues or specific patient preferences is missing, but their IGF-1 ULN were all below 1.8.
Treatment patternThe active treatments given to the cohort at set times during the follow up (1, 2, 5 and 10 years post-surgery) are displayed at a group level in Fig. 1B. A total of 99 (96.1%) patients had records complete enough to be included in the figure. One individual with a GH- and prolactin-secreting pit-NET required chemotherapy with temozolomide during their recorded follow-up. A total of 53 individuals received some type of medical treatment for acromegaly between the time of diagnosis to the end of their follow-up. The most commonly administered medical treatment to the 103 patients was an SRL. Specific treatments during follow-up were SRLs (n = 50, 48.5%, out of which two patients received 2nd generation SRL), combination therapy (n = 23, 22.3%), dopamine agonists (n = 21, 20.4%), radiotherapy (n = 7, 6.8%) and temozolomide (n = 1, 1.0%). Multiple different types of combination medical therapy were used, the two most common combinations were 1st Generation SRL combined with GH receptor antagonist (n = 16) and 1st generation SRL combined with dopamine agonist (n = 7). Radiotherapy was given to 7 patients, of which three received traditional fractionated radiotherapy, two received treatment with gammaknife and two received stereotactic single fraction radiotherapy.
During the study period, hormone substitutions were given according to the numbers in Table 4. The most frequent substitution at all times of follow-up were sex hormones. At 1-year follow-up, only one patient needed desmopressin and no patients had GH substitution. Cortisol substitution was required by four to six patients at different follow-up times.
During long-term follow-up, two patients had suspected cerebral infections. One of them developed a cerebral fungal infection, which caused a mycotic aneurysm leading to a fatal brain bleed. The other had suspected cerebral abscesses where the condition worsened, then stabilized, and then the patient died suddenly (no infectious agent was identified). Both events occurred 15 years after pituitary surgery and could not be clearly linked to the intervention.
Comments (0)