Baseline clinical characteristics
From January 2017 to December 2021, a total of 211 patients were enrolled in this study, of whom 120 participants successfully achieved the LDL-C target (Table 1). Among the study population, 72.0% were male, with a mean age of 57 years old. The mean BMI was 26.4 ± 4.1 kg/m2, and patients who did not achieve the LDL-C target had a significantly higher BMI compared to those who met the LDL-C target. In the LDL-C target achievement group, there was a higher proportion of myocardial infarction (40.8 vs. 25.2%, P = 0.027) and a greater use of antiplatelet agents (90.8 vs. 79.1%, P = 0.027) compared to those who did not achieve the LDL-C target. No statistically significant differences were observed between the two groups with regard to other ASCVD, including coronary artery disease, peripheral artery disease, or transient ischemic attack (TIA)/stroke. The rate of other comorbidities, such as hypertension, diabetes mellitus, heart failure with reduced ejection fraction (HFrEF), chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), end-stage renal disease (ESRD), and cancer, was similar between the groups. Additionally, there was no significant difference in the use of HIS, HIS combined with Ezetimibe or PCSK9 inhibitors (alirocumab and evolocumab) between the LDL-C target achievers and non-achievers. Detailed baseline characteristics of both groups are summarized in Table 1.
The lipid profile at baseline
The baseline lipid profile and other biochemical parameters of the study population, stratified by LDL-C target achievement status, are summarized in Table 2. Mean total cholesterol levels were similar between LDL-C target non-achievers and achievers, with values of 206.0 (IQR 170.0, 248.0) mg/dL and 216.0 (IQR 179.5, 263.0) mg/dL, respectively (P = 0.187). Similarly, there was no significant difference in mean LDL-C levels between non-achievers (135.0; IQR 108.0, 172.0 mg/dL) and achievers (147.0; IQR 110.0, 183.5 mg/dL) with a combined mean of 143.0 (IQR 108.0, 174.0) (P = 0.108). HDL-C levels showed no statistical difference between the two groups, with non-achievers having a mean HDL-C of 40.0 (IQR 35.9, 47.0) mg/dL, and achievers at 41.0 (IQR 36.3, 52.1) (P = 0.264). Triglyceride levels were also comparable between the groups, with non-achievers at 130.5 (IQR 98.0, 178.5) mg/dL and achievers at 150.0 (IQR 103.0, 213.0) mg/dL (P = 0.141). Fasting blood glucose levels, glycated hemoglobin (HbA1C), liver function tests and mean creatinine levels were measured, with no significant difference observed between non-achievers and achievers.
Table 2 The lipid profile and other biochemical data at baselineChanges of lipid profile at 12 weeks after initiating PCSK9 inhibitors
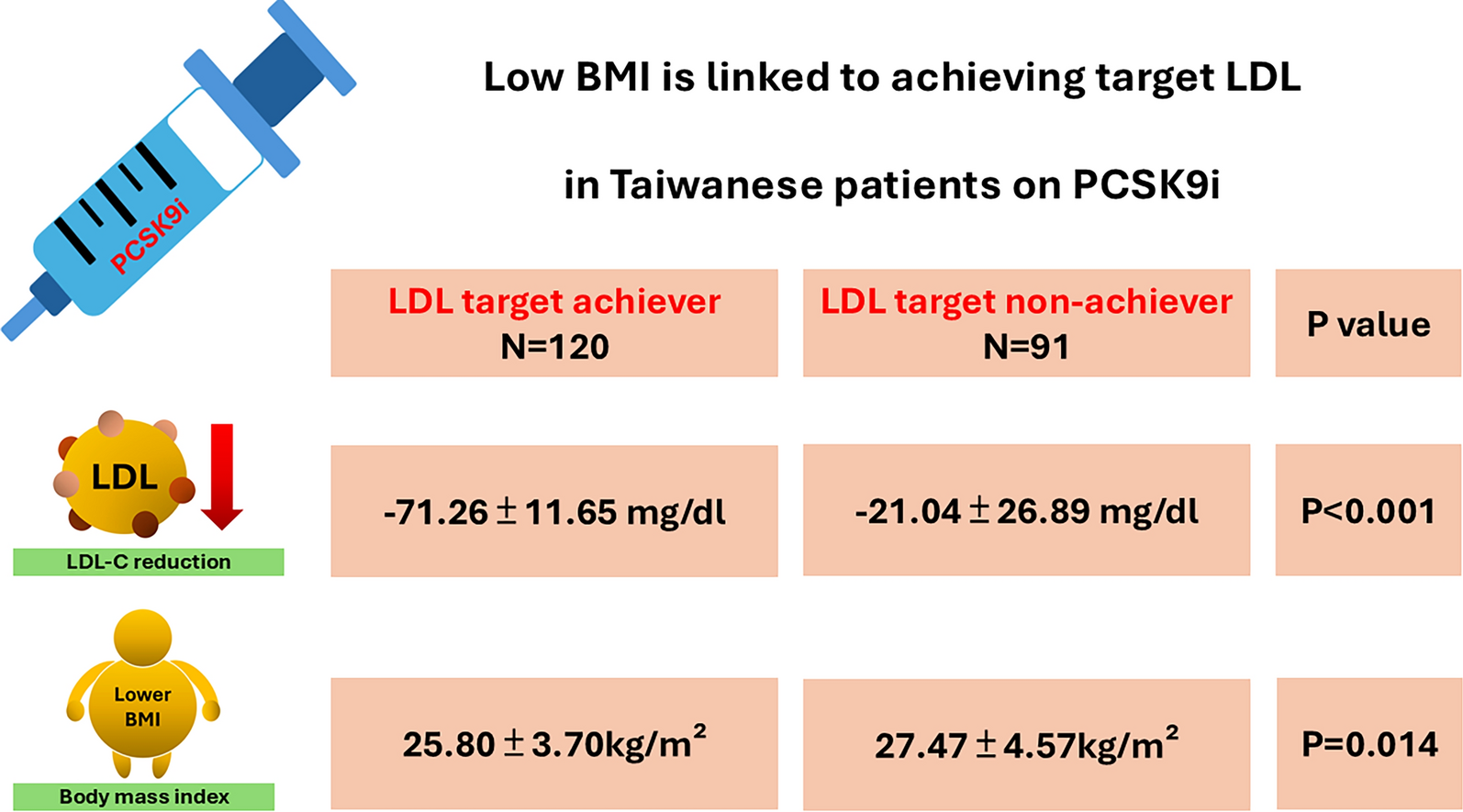
The improvement in lipid profile after 12 weeks of PCSK9 inhibitor therapy, stratified by LDL-C target achievement status, is summarized in Table 3. In the LDL-C target non-achiever group, total cholesterol decreased by − 20.4 (IQR − 28.4, − 6.4) mg/dL, whereas a more pronounced reduction of − 50.9 (IQR − 57.7, − 42.3) mg/dL was observed in the achiever group, with a statistically significant difference between the groups (P < 0.001). A similar trend was noted for LDL-C levels, with a decline of -29.4 (IQR − 38, − 10.5) mg/dL in the non-achiever group and a greater reduction of − 71.5 (IQR − 81.8, − 62.2) mg/dL in the achiever group (P < 0.001). Regarding triglyceride levels, slight increase of 0.8 (IQR − 24.1, 21.8) mg/dL was seen in the non-achiever group, whereas the achiever group experienced a decrease of − 30.8 (IQR − 42.9, − 7.9)mg/dL, with a significant difference between the two groups (P < 0.001). PCSK9 inhibitors also resulted in a more substantial elevation of HDL-C levels in the achiever group compared to the non-achiever group of 5.9 (IQR − 3.2, 22.2) mg/dL vs. 2.3 (IQR − 5.6, 10.3) mg/dL, P = 0.030). No statistically significant differences were observed between the two groups in other biochemical metrics, including fasting blood glucose, HbA1c, liver enzymes, and serum creatinine levels.
Table 3 Changes of lipid profile and other biochemical data at 12 weeks after initiating PCSK9 inhibitors treatmentLDL lowering effect among different starting dose of PCSK9 inhibitors
Table 4 summarizes the impact of different initial doses of PCSK9 inhibitors on LDL-C target achievement. In the non-achiever group, the majority of patients treated with either Alirocumab or Evolocumab were started on a PCSK9 inhibitor dose of 75 mg every 2 weeks (Q2W), whereas in the achiever group, most patients began with a dose of 140 mg Q2W. Among patients receiving alternative dosing regimens, among target achievers treated with Alirocumab, 15.9% of them received 140 mg Q3W to Q4W. Among target achievers treated with Evolocumab, 10.6% of them received 140 mg Q3W to Q4W or 420 mg Q4W. No statistically significant differences were observed between the groups in terms of initial dosing.
Table 4 The starting dose of PCSK9 inhibitorsLogistic regression on factors linked to LDL-C target achievement
Table 5 summarizes the findings of both univariate and multivariable logistic regression analyses assessing factors associated with achieving LDL-C target. BMI was inversely correlated with the likelihood of reaching LDL-C goals. In univariate analysis, the odds ratio (OR) for BMI was 0.904, with a 95% confidence interval (CI) ranging from 0.833 to 0.982 (P = 0.016). This significant association persisted in the multivariable analysis, where the OR was 0.899 (95% CI 0.821–0.984, P = 0.021). Clinical key parameters such as age and sex did not show significant correlations with achieving LDL-C targets while the OR was 1.011 (95% CI 0.990–1.033, P = 0.298) and 1.055 (95% CI 0.575–1.933, P = 0.863), respectively. A history of myocardial infarction was associated with an increased likelihood of meeting LDL-C targets. In univariate analysis, it yielded an OR of 2.040 (95% CI 1.123–3.705, P = 0.019). However, this association lost significance in the multivariable model, with an OR of 2.230 (95% CI 0.996–4.996, P = 0.051). Anti-platelet drug usage was also positively associated with the odds of achieving LDL-C targets in univariate analysis (OR of 2.615; 95% CI 1.175–5.820, P = 0.019); however, these associations were not evident in the multivariable model (OR of 2.864; 95% CI 0.865–9.486, P = 0.085).
Table 5 The univariate and multivariable logistic regression of LDL target achiever in patients receiving PCSK9 inhibitors post 12 weeks 





Comments (0)